
Abstract
The Medical Reserve Corps (MRC) was established in the Office of the Surgeon General in response to the spontaneous but disorganized outpouring of medical volunteers following the terrorist attacks of 2001. The mission of the federal MRC office is to provide organizational structure and guidance to the nearly 1,000 locally organized and funded MRC units that have grown up across the country and the more than 200,000 volunteer health professionals that staff these units. Despite the large size of this program and its numerous activations over the past decade, including in the Boston Marathon bombing and Hurricane Sandy, relatively little is known about the MRC, including the make-up of the units, the ways units have been used, and the challenges faced by MRC units and their volunteers. Here we report the results of a mixed-methods investigation of MRC unit organization, activities, and challenges.
Despite the large size of the Medical Reserve Corps (MRC) program and its numerous activations over the past decade, including in the Boston Marathon bombing and Hurricane Sandy, relatively little is known about it, including the make-up of the units, the ways units have been used, and the challenges faced by MRC units and their volunteers. Here the authors report the results of a mixed-methods investigation of MRC unit organization, activities, and challenges.
L
At the federal level, the Division of the Civilian Volunteer Medical Reserve Corps (DCVMRC) was established in 2002 in the Department of Health and Human Services (HHS), Office of the Surgeon General. Its mission is to “engage volunteers to strengthen public health, emergency response and community resiliency.” 3 Since its inception, the Medical Reserve Corps (MRC) program has grown dramatically and currently provides an organizational structure, guidance, and technical assistance to nearly 1,000 units and more than 200,000 volunteer health professionals nationwide. Currently, 91% of the US population lives in a locality covered by an MRC unit 4 (Figure 1). The volunteer health professionals affiliated with MRC units can be deployed quickly, as their skills and credentials are verified before they are allowed to participate in a response. MRC units are increasingly being integrated into emergency response plans at the local, state, and federal levels.
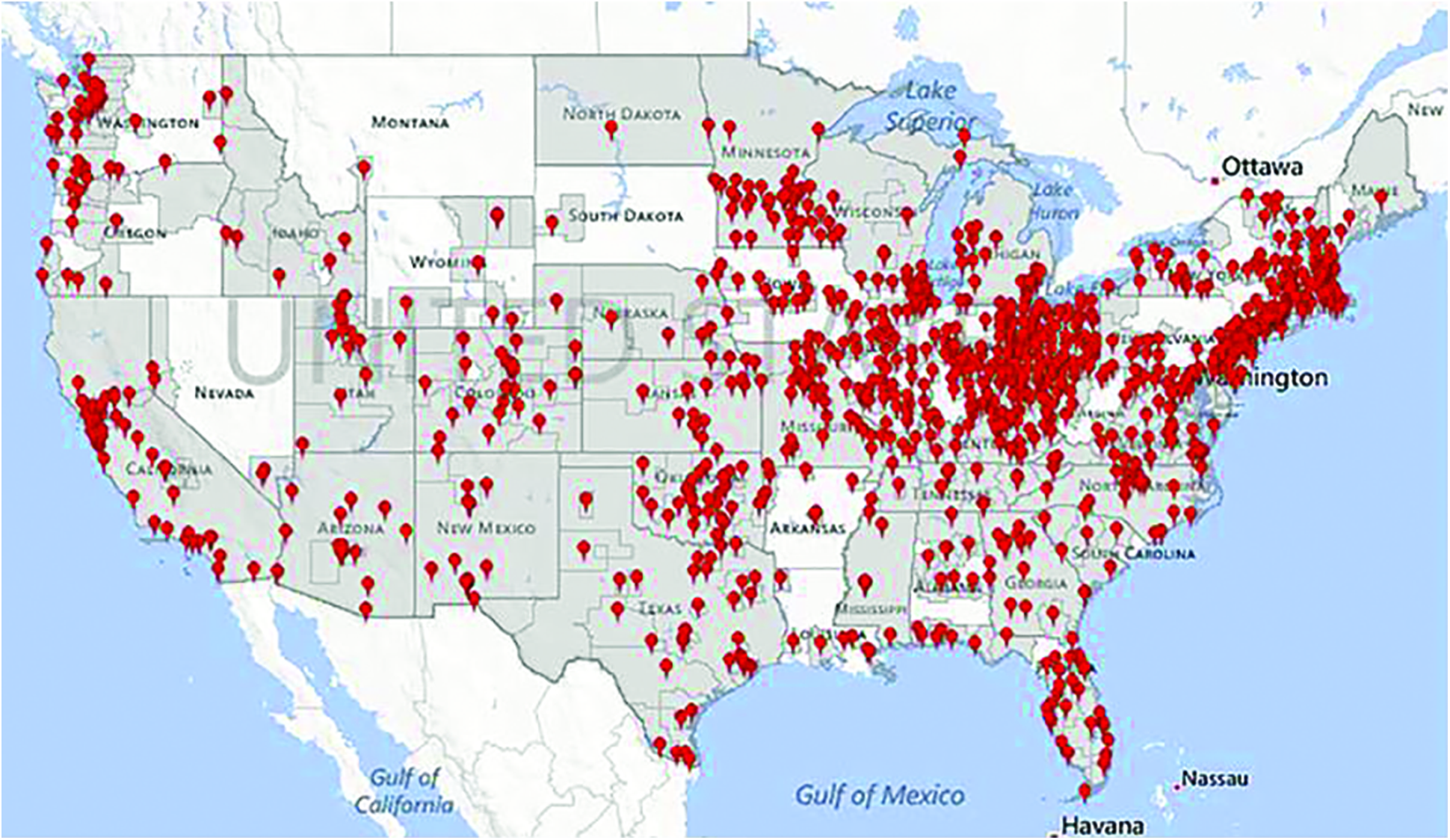
Geographic distribution of MRC units. Regions shaded in gray indicate coverage by an MRC unit. Pins indicate the location of the unit headquarters. (Source: http://www.medicalreservecorps.gov/FindMRC) (Color graphics available at www.liebertonline.com/bsp)
Recent examples of incidents in which volunteer health professionals have contributed to the response effort include the Boston Marathon bombing (2013),5,6 Hurricane Sandy (2012), 7 the Joplin tornado (2011), 8 and the H1N1 influenza pandemic (2009) (Figure 2). 9 When not responding to emergencies, MRC units provide support to local public health efforts, including routine vaccination campaigns, blood pressure screenings, and other health-related activities. 10

Major US events involving VHP response, 2001-2013
There is broad agreement that volunteers are a critical disaster response asset. Recent federal policies and academic literature explicitly consider the role of volunteers. The Implementation Plan for the National Health Security Strategy states that “an adequately sized national health security workforce has a sufficient supply of staff and volunteers to meet everyday community health and related needs as well as a surge in demand for services.”11(p20) The same document identifies “a systematic approach … in place to coordinate and manage health care delivery volunteers during an incident”(p21) as a long-term goal for strengthening the nation's health security. 11 Along the same lines, volunteer management is a common capability in recent preparedness guidance issued by the Centers for Disease Control and Prevention (CDC) and HHS's Assistant Secretary for Preparedness and Response (ASPR).12,13 Finally, Schultz and colleagues identify volunteer management and the use of government response teams as 2 core competencies for acute care medical professionals. 14
We undertook this project to provide a current description of the overall MRC program, outline the roles volunteers play in disaster and nondisaster settings, identify challenges faced by MRC units, and provide recommendations aimed at overcoming those challenges. The role of other government agencies involved in medical response, such as the National Disaster Medical System (NDMS) and FEMA's Urban Search and Rescue teams, while critically important, are not considered in this analysis. The role of nongovernment organizations (NGOs), such as Team Rubicon and the American Red Cross (ARC), are considered only with respect to their relationship with MRC.
Methods
We used a mixed-methods approach, consisting of semistructured interviews, a survey, and data analysis, to characterize the units, document their experiences, and understand their successes and challenges. The research was submitted and classified as exempt by the UPMC IRB.
Qualitative Methods
After a review of the relevant literature on volunteer health professionals, the MRC, and recent disaster responses that have involved volunteer responders, we used qualitative methods to better understand the organization, its strategic focus, and the successes and challenges of volunteer health professionals' disaster response in general and of the MRC program in particular. The research team first conducted 9 semistructured telephone interviews with 17 representatives from MRC units and other response partners, such as ARC, AmeriCorps, and hospitals. Participants in these discussions were drawn from a convenience sample and represented urban, suburban, and rural MRC units. Participants were asked to describe their programs, notable disaster responses, and the challenges they face as MRC volunteers. If participants were not affiliated with an MRC unit, the interviews focused on general volunteer management and experiences working with MRC volunteers. The interviews were conducted on a not-for-attribution basis. Notes were taken to ensure accuracy. The case studies and interviews were analyzed for common themes, and these themes were then converted into research questions to guide the subsequent quantitative analysis.
Quantitative Methods
The DCVMRC granted the research team access to the large set of data collected about the MRC units nationwide in July 2012. The data were coded, summarized, and analyzed in light of the research questions identified from the qualitative phase of this research. Other questions that could not be answered from DCVMRC data were put into a separate survey created using SurveyMonkey (Palo Alto, CA). This survey gathered additional information from MRC unit coordinators about unit composition, organization, the role their volunteers played during emergency response, and their perceptions regarding the challenges they face. The survey was sent to the coordinator of each of 982 MRC units with the support and cooperation of the DCVMRC staff. The survey was open for 30 days in August and September 2012. Of the unit coordinators who received the survey, 201 responded, yielding a response rate of 20%.
We summarized the responses to the additional survey using both overall percentages and percentages by unit type (mixed, rural, suburban, and urban). A one-way ANOVA was used to detect whether there were differences in responses between types, and if there were, we performed Fisher-Hayter tests for pairwise comparisons.
Results
Qualitative Results: Lessons from Past Disasters
The MRC program was established to provide an organizational framework for augmenting the medical response to disasters, which MRC members have done for the past decade (Figure 2). 10 The first national mobilization of MRC units was the 2005 response to Hurricane Katrina. Approximately 1,500 MRC volunteers participated in an optional deployment to the Gulf Coast region to provide medical care, primarily in ARC shelters.10,15 An additional 6,000 volunteer health professionals were involved in activities organized by their local MRC units, including providing care to evacuees. 15
Our participants indicated that the most appropriate roles for volunteer health professionals in disaster response can vary and are determined by the nature of the incident. Because of the wide range of educational and technical backgrounds represented in MRC units, volunteer health professionals could notionally be used to provide everything from inpatient-level care, to basic first aid, to activities that do not require medical training. The majority of response activities undertaken by MRC units and other volunteer health professionals were geared toward basic first aid rather than providing hospital-level care. For example, in the 2009 H1N1 influenza pandemic response, MRC volunteers focused on staffing vaccination clinics, and in the response to the Joplin tornados and Hurricane Sandy in 2011, efforts were focused on search and rescue, first aid, and patient evacuation and transport.
Participants also indicated that, in every disaster involving response by volunteer health professionals, consideration must be given to the legal protections that allow volunteers to work without fear of unwarranted legal consequences. Serious legal questions may arise during times when crisis standards of care are in effect, and medical volunteers who are unprotected by liability safeguards may be vulnerable to litigation. In past disaster responses, including Hurricanes Katrina and Sandy, the participation and roles of volunteer health professionals appear to have been limited by a lack of legal protections or inadequate legal protections. For example, during a number of disasters, MRC members who served in ARC shelters noted that they were not permitted to provide any medical care more advanced than first aid because of ARC liability concerns. Advances have been made in this area, but it is unclear how legal protections and volunteer health professionals' perceptions of legal protections affect MRC units' ability to respond to disasters.
Quantitative Results
Data Provided by DCVMRC
The DCVMRC collects and maintains data on their units' makeup and activities. In this section, we analyze the data elements that provide an overview of local MRC units.
Units and Workforce—In 2012, the DCVMRC listed 982 locally based units, which vary in size based on geographic location. In total, there were more than 200,000 volunteer health professionals registered with MRC units in 2012. The mean unit size was 210 volunteers. Among these volunteers, there was a wide range of training and professional backgrounds, including physicians (7%), nurses (28%), emergency medical technicians and paramedics (5%), public health personnel (11%), and other health providers (11%). The remaining 38% were nonmedical volunteers who, despite not having medical training, contributed valuable services including logistics, technical support, and legal services. The MRC has continued to grow over time. Using Frasca's reported MRC enrollment in 2009 as a baseline, MRC membership grew by 8% between 2009 and 2012. 10
Unit Coordinators—MRC unit coordinators provide leadership and organization and serve as a point of contact with the DCVMRC staff. In 2012, 18% of unit coordinators were volunteers themselves; 82% were employed in some emergency response or management capacity, but not necessarily as full-time MRC coordinators. Over half of unit coordinators (63%) spent between 1% and 25% of their effort on MRC-related activities.
Sponsoring Organization—In 2012, 64% of MRC units were sponsored by local health departments, which may help to explain their nonemergency support of local public health activities. The second most commonly reported sponsoring organization was an emergency management agency (10%). The remaining units were supported by a range of other government or nongovernment entities.
Support for Local Public Health Efforts—Nonemergency activities are a significant aspect of MRC unit operations. MRC members provide support to routine efforts such as seasonal influenza vaccination campaigns (63%), health screenings (31%), and health education (67%). This volunteer support is especially significant in light of recent cuts to the nation's public health workforce. 16
Funding and Planning—MRC units conduct operations on relatively limited budgets from a range of federal, state, local, and private sector partners. Following DCVMRC guidance, MRC unit coordinators receive funding from multiple federal agencies. Commonly reported funding sources include FEMA's Citizen Corps (26%), ASPR (23%), the Office of the Surgeon General (24%), CDC (17%), “other” HHS (14%), “other” Department of Homeland Security (8%), Metropolitan Medical Response System (MMRS, 9%), and the Urban Area Security Initiative (6%). Twenty percent reported receiving no federal funds, and 20% reported “other” federal funding.
Support from state and local partners was similarly varied. In-kind support from sponsor (72%) and partner (43%) organizations was commonly reported. Financial contributions or grants from state governments (35%), foundations or NGOs (18%), local governments (18%), and the private sector (16%) were also reported. Seven percent reported “other” nonfederal funding, and only 1% reported receiving no nonfederal funding.
In 2012, 45% of MRC unit coordinators reported an operating budget of $5,000 a year or less. When queried about an optimal funding level, 17% indicated that an amount between $0 and $5,000 was optimal; 25% responded between $5,000 and $10,000; and 23% between $10,000 and $25,000. Finally, MRC unit coordinators reported being well integrated into both local and state emergency planning, with 81% and 74% indicating “high” levels of integration with local and state agencies, respectively.
Challenges—According to data collected by DCVMRC, most (88%) MRC unit coordinators reported some challenge in their ability to respond. Reported challenges included volunteer availability (60%), MRC leader time constraints (51%), funding (41%), number and/or type of volunteers (31%), a lack of a legal protections (26%), a lack of integration into response plans (15%), and conflict—real or perceived—with other volunteer organizations (14%); 12% reported no challenges.
Results from MRC Coordinator Survey
To better describe MRC unit composition, activities, and challenges, we conducted a separate survey aimed at gathering data on unit organization, activation and deployment, and associated legal issues. A convenience sampling of all the MRCs contained in the DCVMRC database resulted in 201 completed responses (Table 1).
Descriptive Statistics, MRC Coordinator Survey
The 201 MRC units in our sample consisted of 44 rural units, 18 suburban units, 18 urban units, and 121 mixed units. Mixed units have assigned jurisdictions consisting of urban, suburban, and rural areas. Respondents to our survey were, on average, larger in terms of number of volunteers relative to all MRCs in the US. The average number of volunteers for each MRC unit in our sample was 346. Urban MRCs had the highest average number of volunteers at 539, while rural MRCs had an average of 159 volunteers. The majority (65%) of our respondents indicated that they used the Emergency System for Advance Registration of Volunteer Health Professionals (ESAR-VHP) system along with a local system (16%). Almost all (89%) of the MRCs in our sample indicated that their volunteers are organized by specialty and can be contacted according to needed specialty.
Unit Activation—Nearly 85% of our respondents indicated that they expected their volunteers to participate in all response activities, whether or not the activity involved providing medical care. Most (57%, n=115) reported having responded to an actual emergency or disaster. Survey respondents indicated that, once activated, MRC-affiliated volunteers performed a number of clinical and nonclinical tasks (Figure 3) in a range of settings (Table 2). Tasks relating to drug and vaccine dispensing, health education, and basic medical care and triage were the most commonly reported activities, while more advanced medical procedures and activities were reported infrequently.

VHP Skill Utilization
Medical Reserve Corps Activation Characteristics
The most common setting in which MRCs worked was at a point of dispensing (POD) for medical countermeasures (Table 2). PODs are intended to expedite the administration or dispensing of therapeutics or vaccines in the event of an epidemic or bioterror attack. Overall, 73% of the MRCs responding to our survey indicated that they had worked at a POD. MRC units were extremely active during the 2009 pandemic, and the broad geographic nature of that emergency would contribute to high rates of POD use and, therefore, reporting. 8 Other common settings for MRC activation included ARC shelters (39%) and community health centers (33%).
Notably, use of volunteers in healthcare settings was infrequently reported, with only 7% of unit coordinators reporting volunteer activity in an alternative care facility. Very few unit coordinators reported having performed more advanced care or having operated inside hospitals. Among the 115 MRCs that had been activated, nearly a third of their effort during activation was devoted to nonmedical activities. Half (51%) of MRCs felt that their clinical skills were used well or very well, compared to 49% who reported that their skills were used fairly well or not well. Overall, 78% of MRCs reported that their volunteers were somewhat or very satisfied with their roles. MRCs serving mixed and urban jurisdictions had higher volunteer satisfaction rates (82% and 86%) when compared to MRCs that served rural jurisdictions (53%).
Unit Deployment—Of the 115 MRCs that were activated, 35 (30%) reported sending volunteers outside of their assigned jurisdiction, with most of the 35 (83%) remaining in the state. While reporting that the deployments were successful (4.4 on a 5-point scale, where 1 is least and 5 is most successful), more than half reported barriers to deployment. Available transportation (58%), volunteer availability (58%), funding support (53%), and a lack of integration guidance (53%) were all cited as barriers among the 19 MRCs that reported encountering barriers.
Legal Issues—While the need for volunteer health professionals during emergencies is unquestioned, the legal and regulatory framework underlying the use of volunteers has long been understood to affect the use and participation of volunteers, both within and outside of emergency response situations. 10 Licensing, credentialing, and privileging of volunteer health professionals; civil and criminal liability of volunteers and volunteer organizations; and workers' compensation benefits for volunteers are commonly cited legal issues affecting volunteer health professional integration.10,15,17
More than half of the MRCs in our sample (58%) reported being somewhat to very confident about their legal protection during an emergency response. Conversely, less than half (41%) indicated being confident about their legal protection during a nonemergency response, and 59% of the MRCs in our survey were either neutral or somewhat or very unconfident about legal protections during a nonemergency response (Table 3). MRCs that serve suburban jurisdictions were least likely to feel confident about their legal protections in either medical (50%) or nonmedical (39%) responses. Finally, when asked about how comfortable they were about their personal knowledge on legal protections, 55% of the overall sample responded that they were somewhat to very comfortable with their own knowledge, with only a third of suburban coordinators responding that they were comfortable with their personal knowledge.
Medical Reserve Corps Legal Protections
A majority of MRCs (80%) reported providing legal education to volunteers. Nearly a third of all survey respondents indicated that legal concerns affected their ability to recruit volunteers. Concerns were highest among suburban MRCs, where 39% responded that it affected their ability to recruit. One-quarter of respondents indicated that legal concerns affected volunteer willingness to respond. These concerns were highest among the volunteers in the suburban MRCs (39%) and lowest among the rural and urban MRCs (14% and 11%, respectively). Among all MRCs, 9 (4%) reported having had the need to invoke protections for a volunteer. Seven (3%) reported having had to invoke legal protections for the MRC unit.
MRC units are also advised to take precautions to manage risk more generally and to provide for a safe working environment for volunteer health professionals and the public they serve. 18 Almost two-thirds of MRCs required that their volunteers undergo background checks. Rural MRCs (52%) and suburban MRCs (44%) were less likely to require a background check compared to mixed (69%) and urban MRCs (72%). Of those MRCs that reported conducting background checks on volunteers, 59% reported that these checks were either easy or not very burdensome.
Discussion
We present the findings of a mixed-methods evaluation of the Medical Reserve Corps, including the results of a nationwide survey of MRC unit coordinators. We sought to describe how, when, and where volunteer health professionals are being used and to identify opportunities for improvement.
To fully maximize the utility of the volunteer health professional workforce, ongoing efforts to integrate MRC units into existing response plans and mechanisms should continue. To that end, MRC unit coordinators should give priority to establishing and deepening partnerships with their local healthcare coalitions. These organizations are heterogeneous but typically consist of hospitals, a local public health department, and traditional first responders, and their purpose is to organize emergency healthcare response. These coalitions have developed during roughly the same timeframe as the MRC, and they were catalyzed by the availability of federal funding. 19 We found little evidence that volunteer health professionals are used in hospitals. Prioritizing the operation of alternative care facilities in concert with local hospital preparedness coalitions would allow MRC-affiliated volunteer health professionals to use their skills and contribute to medical surge capacity. Alternatively, MRC volunteers could provide surge capacity elsewhere in the healthcare system, including in long-term care facilities, although additional planning and training would be required.
MRC unit coordinators should also continue to emphasize outreach to and joint training with other agencies with a medical response mission. The partnership between MRC and ARC is especially important, as MRC volunteers frequently reported providing care in ARC shelters. The fact that only 14% of unit coordinators cited “conflict—real or perceived—with other volunteer organizations” as a challenge would seem to indicate progress on this front. In addition, NGOs such as Team Rubicon may share an operating area or patient population with responding MRC units. Establishing and maintaining these partnerships would enhance the exchange of information and best practices, may help to prevent redundancies or interagency tension, and may ultimately improve the care rendered during a response.
MRC programs at both the federal and local levels are challenged by increasing constraints in resources. In FY2014, the HHS Public Health and Social Services Emergency Fund includes a request for $9.0 million to fund the DCVMRC. 20 This funding level represents a 29% decrease from DCVMRC's FY2010 high of $13 million. At the unit level, 45% of MRC coordinators reported an operating budget of $5,000 a year or less. As indicated by our survey results, one challenge presented by this level of funding is a limited ability to deploy volunteers on extended or long-distance assignments. Unlike other federal preparedness programs that build emergency response capacity at the state and local levels, DCVMRC does not provide funding to support individual units. Therefore, to ensure sustainability unit leaders are advised to seek support from a range of federal, state, local, and private sector stakeholders. That diversification, as evidenced by the broad array of funding sources reported above, has thus far enabled the establishment and ongoing operations of MRC units across the country.
Legal challenges have long been pointed to as a barrier that impedes volunteer health professionals' response. Indeed, extensive efforts, particularly after 9/11, have been undertaken to understand and strengthen laws affecting the integration of volunteer health professionals into disaster and emergency response.10,21,22 That most respondents report that they are confident in legal protections applicable during emergencies and that the laws in place are thought either not to hinder or even to help both recruitment and willingness to respond indicates that much of the work over the past decade has not been without benefit. However, the results also indicate that legal protections are seldom invoked, signaling that while there is an apparent shared perception that the legal environment supports volunteer health professional integration, it would appear that the laws are largely untested. Notably, unit coordinators are more concerned about the adequacy of legal protections for volunteer health professionals working in nonemergency settings than those responding to an emergency. Such concerns are remarkable considering the increasingly important role that MRC volunteers are playing in supporting local public health efforts in their communities.
Several caveats to this research deserve mention. Our findings, both qualitative and quantitative, are among the first documented to characterize the activities and challenges among MRC units. However, both our interviews and web survey of MRC unit coordinators were samples of MRC units, and our findings may not be generalizable to other units. Moreover, our results are subject to recall bias, as respondents self-reported information on past unit activations and activities. Finally, larger MRC units from mixed and nonrural jurisdictions were overrepresented in our sample, potentially biasing our findings if the rural jurisdiction response rate is related to any of the MRC characteristics explored in the survey.
In general, both the federal MRC division and their nearly 1,000 local MRC units have proven to be a flexible and sustainable addition to the nation's emergency response capabilities. The MRC is unique among medical response agencies in that it contributes most to the extremes of the response spectrum, bolstering local nonemergency public health efforts on the one hand, and enhancing surge capacity in the healthcare system during catastrophic events on the other. MRC units provide a practical outlet for the goodwill and altruism of more than 200,000 volunteers and serve to bolster community resilience across the nation.
Footnotes
Acknowledgments
We gratefully acknowledge Capt. Robert Tosatto, Director, DCVMRC, and his colleagues for granting access to the DCVMRC database and for facilitating distribution of the survey. We declare that we have no conflict of interest.