
Abstract
In 2011, an EF5 tornado hit Joplin, MO, requiring complete evacuation of 1 hospital and a patient surge to another. We sought to assess the resilience of healthcare workers in these hospitals as measured by number reporting to work, willingness to work, personal disaster preparedness, and childcare responsibilities following the disaster. In May 2013, a survey was distributed to healthcare workers at both Joplin hospitals that asked them to report their willingness to work and personal disaster preparedness following various disaster scenarios. For those with childcare responsibilities, scheduling, costs, and impact of hypothetical alternative childcare programs were considered in the analyses. A total of 1,234 healthcare workers completed the survey (response rate: 23.4%). Most (87.8%) worked the week following the Joplin tornado. Healthcare workers report more willingness to work during a future earthquake or tornado compared to their pre-Joplin tornado attitudes (86.2 vs 88.4%, t=−4.3, p<.001; 88.4 vs 90%, t=−3.1, p<.01, respectively), with no change during other scenarios. They expressed significantly higher post-tornado personal disaster preparedness, but only preevent preparedness was a significant predictor of postevent preparedness. Nearly half (48.5%, n=598) had childcare responsibilities; 61% (n=366) had childcare needs the week of the tornado, and 54% (n=198) required the use of alternative childcare. If their hospital had provided alternative childcare, 51% would have used it and 42% felt they would have been more willing to report to work. Most healthcare workers reported to work following this disaster, demonstrating true resilience. Disaster planners should be aware of these perceptions as they formulate their own emergency operation plans.
In 2011, an EF5 tornado hit Joplin, MO, requiring complete evacuation of 1 hospital and a patient surge to another. The authors sought to assess the resilience of healthcare workers in these hospitals as measured by number reporting to work, willingness to work, personal disaster preparedness, and childcare responsibilities following the disaster. Most healthcare workers worked the week following the Joplin tornado. Nearly half had childcare responsibilities, and some required the use of alternative childcare. If their hospital had provided alternative childcare, half would have used it and many felt they would have been more willing to report to work.
D
In this article, we define resilience as the ability to return to work rapidly or the willingness to work in future disasters. Resilience is a key factor in survival, as it decreases the negative impact of a disastrous event. It is vital for healthcare system managers to understand factors that could influence healthcare workers' resilience to disasters and to help mitigate those factors causing the most distress so that surge capacity can be maximized.17-19
In Spring 2011, a powerful Enhanced Fujita (EF) 5 tornado swept through the city of Joplin, Missouri, destroying a section of the city up to a mile wide, killing 158 people, and injuring more than 1,000 others. 20 In addition, the tornado hit directly one of the city's major hospitals, resulting in 6 fatalities and the need for a complete hospital evacuation. A nearby hospital, which had only minimal damage, received many of the evacuated patients and injured community members, resulting in a substantial patient surge. Additionally, many schools and daycare centers were closed or damaged.
The purposes of this survey were to determine Joplin healthcare workers' perceptions following this real disaster as they relate to the following factors: (1) factors associated with reporting to work during the week following the 2011 Joplin tornado; (2) factors associated with future willingness to work following hypothetical natural and man-made disasters; (3) impact on personal disaster preparedness; and (4) worker childcare responsibilities and alternative childcare plans.
Methods
Healthcare workers from the destroyed hospital and the one still standing in Joplin were surveyed 2 years after the tornado. A link to an online survey was sent to the director of disaster preparedness of each hospital in May 2013; the directors were asked to forward the survey link to all hospital staff and employees. Reminder emails were sent to disaster preparedness directors 2 weeks later. All employees/staff members who had been employed at either one of the hospitals at the time of the tornado were eligible to participate. Participants were asked to identify their employing hospital at the time of the disaster to account for any switchover in staff that may have occurred following the tornado.
Survey Questionnaire
Instruments used in past willingness to work disaster surveys were used to develop this study's questionnaire1-6,9,11,12,14,21,22; however, this specific survey was not validated before it was distributed. The 52-item instrument (see Supplementary material at www.liebertonline.com) measured healthcare workers' self-reports of:
• work during the week following the tornado; • willingness to work following various hypothetical disaster scenarios (eg, tornado, earthquake, pandemic with a 2% defined mortality with and without an effective vaccine, and dirty bomb), both before and after the 2011 Joplin tornado; • personal disaster preparedness, both before and after the 2011 Joplin tornado; • perceived impact of having childcare responsibilities on willingness and ability to work; • availability, use of, associated costs, and perceived concerns associated with alternative childcare; • extent to which childcare responsibilities affected their ability to work regular and/or unscheduled shifts; • personal responsibilities other than children at the time of the Joplin tornado (eg, elders, disabled family members, pets, farm animals); • extent of home damage, ability to live in their home the week following the tornado, and what utilities they lost; and • attitudes regarding hypothetical alternative childcare programs.
Willingness to work was assessed on a continuum of 0 to 100, with 0 indicating complete unwillingness to work and 100 indicating complete willingness to work in each scenario, resulting in continuous variables. There were 8 objective measures of personal preparedness: 3 days of food, 3 days of water, flashlight, radio, first aid kit, emergency childcare plan, emergency pet care plan, and emergency elder care plan. Each personal plan item was assigned 1 point. If individuals had that item in their plan, they were given 1 point for it; if they did not have it, they were given 0 points for that item. Items 1 to 5 were included in the score for all individuals. Only those who indicated that they had responsibility for a child(ren), pet(s), farm animal(s), or an elderly or disabled person were scored on whether or not they had a corresponding emergency care plan to address this responsibility (1 point if yes; 0 points if no). Therefore, denominators could range from 5 to 8, depending on the number of identified responsibilities. A personal disaster preparedness score was calculated as a percentage of possible preparedness indicators, to account for the varying denominators.
With respect to childcare issues, we analyzed responses of all employees with childcare responsibilities, rather than just parents, who were defined as providers with the responsibility for the care of at least 1 child under 18 years of age during the week of the tornado. The study was considered exempt by the university's Institutional Review Board.
Data Analysis
The Statistical Package for the Social Sciences (SPSS 20.0) was used for all analyses. Descriptive statistics were computed for all variables, and a critical p-value of 0.05 was considered significant. Univariate analyses were conducted using demographic variables and attitude/belief items. A hierarchical multivariate logistic regression was then conducted to determine predictors of working the week after the Joplin tornado. Good model fit, indicated by a nonsignificant chi-square value, was calculated with the Hosmer and Leme show goodness-of-fit test for the logistic regression. For all regression analyses, only variables that were significant in univariate analysis were included in the multivariate analyses. Variables that were significant on univariate analysis but nonsignificant on multivariate analysis were dropped from the model; only final models are reported.
Paired t-tests were used to compare healthcare workers' willingness to report to work before versus after the tornado across different disaster scenarios (eg, earthquake, tornado, pandemic in which a vaccine is available, pandemic without vaccine, and a dirty bomb). Linear regression was used to identify factors associated with willingness to work following a future event. McNemar tests were used to compare personal disaster preparedness scores before versus after the tornado, and the percentage of individuals who had each individual component of a personal disaster plan before the Joplin tornado versus how many have the item in their post-tornado plan. A Poisson regression was used to identify factors associated with higher personal disaster preparedness scores.
Chi square was used to compare the relationship between the following: (1) having childcare responsibilities and whether or not personnel worked the week after the tornado; (2) those who had an alternative childcare plan in place prior to the tornado when comparing whether or not the hospital employee actually worked the week of the tornado; and (3) comparing the impact on willingness and ability to work among those who had childcare responsibilities and needed childcare versus those with childcare responsibilities who did not need childcare. An analysis of variance was used to assess differences on perceived impact of willingness and ability to work during the week of the tornado when comparing the age of the worker's youngest child; Tukey post hoc test was used to identify differences in age categories. A McNemar test was used to compare the percentage of individuals who had an alternative childcare plan before the 2011 Joplin tornado to the number who currently have such a plan. Logistic regression was used to describe factors associated with currently having an alternative childcare plan.
Results
In total, 1,234 of 5,261 hospital personnel completed at least some portions of the survey, resulting in a response rate of 23.4%. Most (87.8%) worked the week following the tornado. The vast majority of hospital respondents were women (83.8%, n=980/1,170 respondents), and 96.9% were white. All age groups responded, with almost equal representation across these age groups (18-24, 25-34, 35-44, 45-54, 55-64, and 65+). The education level of the workers was reported as follows: 32.4% (n=379) were high school graduates or had some college; 28.9% (n=339) had an associate degree; 28.8% (n=338) had a bachelor's degree; and 9.7% (n=114) had a master's degree or higher. Half (49.6%, n=591) of the 1,191 hospital respondents were clinical workers, and of those, 54.3% (n=315) were registered or licensed practical nurses. Another quarter of respondents were clerical or housekeeping staff (24.6%, n=294/1,191 respondents).
All areas of the hospital were represented, with two-thirds of respondents indicating that they worked in either inpatient care (33.5%, n=392) or non–patient care areas (31.3%, n=366). The majority (86.9%, n=1,017) reported that they worked full-time. Most respondents (62.3%, n=769) reported that, prior to the tornado, they had been employed by the intact hospital, while approximately one-third (37.7%, n=465) reported that they had been employed by the severely damaged facility.
Working After the Tornado
From logistic regression (Table 1), the determinants of working the week after the Joplin tornado included the following: (1) house not being completely destroyed by the tornado; (2) being employed at the less-damaged hospital; (3) perceiving that childcare responsibilities did not adversely affect the individual's ability to work; (4) being employed full-time; and (5) reporting a higher willingness to work during a future tornado. There was no significant relationship between actually working the week following the tornado and the following factors: (1) demographic variables, (2) having childcare responsibilities, (3) having responsibility for a pet or elderly person, (4) willingness to work following other disaster scenarios, (5) personal preparedness prior to the tornado, and (6) having received prior incident command service (ICS) training.
Factors Significantly Associated with Working the Week Following the Joplin Tornado a
OR=odds ratio; CI=confidence interval.
Logistic regression
With the exception of actual work attendance the week after the tornado, there were no significant associations between the employing hospital and variables of interest to this study. For this reason, the data from the responses from all employees were combined in the analyses below.
Willingness to Work Before vs After the Tornado
Hospital personnel were asked to report how willing they would have been to report to work during various hypothetical disaster scenarios before and after the 2011 Joplin tornado. Respondents indicated that, before the 2011 Joplin tornado, they were most willing to work following a hypothetical tornado (88.4%) or earthquake (86.2%) and least willing to work during a pandemic in which there was no effective vaccine (64.5%; Table 2). Respondents were significantly more willing to report to work following a hypothetical tornado than any other hypothetical disaster scenario (p<0.001 for all comparisons), including an earthquake.
Hospital Workers' Willingness to Report to Work Before Versus After the 2011 Joplin Tornado (N=1,234)
NS=not significant.
Willingness to work during each disaster scenario
Determined by the paired t test
Following the Joplin tornado, the hospital personnel again reported that they would be most willing to work following a hypothetical tornado (90%) or earthquake (88.4%) and least willing to work during a pandemic in which a vaccine is not available (64.0%; Table 2). They reported significantly more willingness to work following a hypothetical tornado compared to all other types of hypothetical disasters (p<0.001 for all comparisons). Hospital personnel's willingness to work after the Joplin tornado increased significantly for natural disasters but not for pandemics or man-made disasters (Table 2; tornados, 88.4% to 90.0%, t=−3.1, p<0.01; earthquakes, 86.2% to 88.4%, t=−4.3, p<0.001).
Healthcare workers who had childcare responsibilities with childcare needs the week of the 2011 Joplin tornado expressed a decreased willingness to work during a future tornado (β=−1.5, SE 0.57, p<0.01). Additionally, significant determinants of post-tornado willingness to work following a future hypothetical tornado included post-tornado willingness to work during an earthquake or dirty bomb, and pre-tornado willingness to work during a tornado or dirty bomb (Table 3).
Factors Significantly Associated with Willingness to Work Following a Future Tornado a
SE=standard error.
Linear regression, controlling for age, gender, and race, determined by one-way analysis of variance (ANOVA).
Items that were not significantly associated with willingness to work following a future hypothetical tornado included: hospital at which they worked at the time of the tornado, having responsibility for an elderly or disabled person, having responsibility for a pet or farm animal, work area, occupation, education level, prior ICS training, personal disaster preparedness, and extent to which their home was damaged during the Joplin tornado.
Personal Disaster Preparedness
Eight components of a personal disaster plan were assessed, both before and after the Joplin tornado (Figure 1). Personal disaster preparedness scores increased significantly after the Joplin tornado compared to before (0.63 post- vs 0.47 pre-Joplin tornado, p<0.001). In addition to an increase in overall scores, the individual components of personal disaster preparedness increased significantly from pre- to post-tornado for all plan components (p<0.001 for all comparisons; Figure 1). Prior to the Joplin tornado, the components of personal disaster preparedness most frequently reported by hospital personnel were a flashlight (72.4%, n=894), an emergency childcare plan (61.2%, n=224), and a first aid kit (58.6%, n=723). The components of personal disaster preparedness most frequently reported by the hospital personnel following the tornado were a flashlight (84.4%, n=1,042), an emergency childcare plan (82.2%, n=301), and an emergency elder care plan (79.6%, n=238).
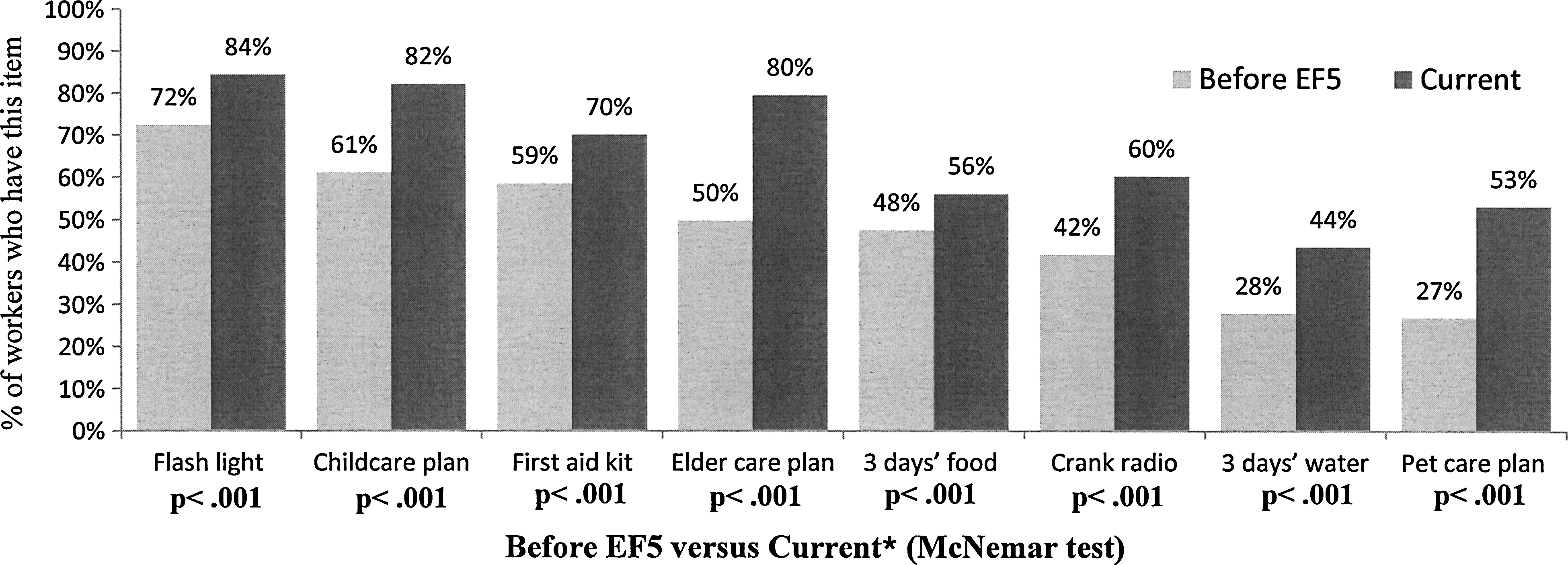
Hospital Personnel's Personal Preparedness Before and After the 2011 Joplin Tornado
The 2 biggest areas that showed improvement in personal disaster preparedness for hospital personnel following the disaster were having an emergency pet care plan (from 26.9% to 53.3%, n=472, p<0.001) and having at least 3 days' worth of water stockpiled (from 28.0% to 43.7%, n=539, p<0.001); these were also the least-reported components of plans reported by the hospital staff prior to the Joplin tornado. Almost three-quarters of the hospital respondents (71.8%, n=886) reported that they had responsibility for a pet(s) or farm animal(s) the week following the Joplin tornado.
In addition, 24.2% (n=299) reported that they had responsibility for an elderly or disabled person the week following the Joplin tornado. Prior to the tornado, half of these individuals (49.8%, n=149) had reported having an emergency care plan for the elderly or disabled person for whom they had responsibility. The percentage of hospital personnel who reported having an emergency elder care plan increased significantly 2 years later (from 49.8% to 79.6%, p<0.001).
From Poisson regression, the only significant determinant of hospital personnel's post-tornado personal disaster preparedness was being more personally prepared before the Joplin tornado (β=2.3, CI 1.6–3.4, p<0.01). Personal disaster preparedness was not significantly different when comparing the following healthcare workers' characteristics: demographics (gender, age, race, etc); pre-tornado hospital of employment; having responsibility for a child(ren), a pet, or farm animal; occupation; work area; education level; or the extent to which their home was damaged during the Joplin tornado.
Children and Childcare Responsibilities
Of the 1,234 respondents, 48.5% reported that they had responsibility for at least 1 child under the age of 18 in their household the week following the 2011 Joplin tornado. The remainder of the study results in this section will refer only to the cohort of respondents who reported having responsibility for at least 1 child during the week following the 2011 Joplin tornado (n=598).
Healthcare workers with childcare responsibilities were more likely to work the week after the tornado compared to those without (89.8% vs 85.8%; X2=4.5, p<0.05). Most (61.2%, n=366) of these respondents with childcare responsibilities indicated that childcare was needed for at least 1 of their children in order for them to be able to work during the week following the tornado. However, with respect to actually reporting for work, there were no significant differences between those who required childcare compared to those who did not. Still, of those with childcare needs (n=366), over a third reported that these responsibilities had a significant impact on their ability (36.6%) and willingness (36.9%) to work. In contrast, of those who did not have childcare needs (n=232), significantly fewer reported that having responsibility for a child the week of the tornado had a significant impact on their ability (19%) and willingness (19.8%) to work (X2=19.6 and X2=21.2, respectively, p<0.001 for both; Table 4).
Perceived Impact of Childcare Needs on Employees' Willingness and Ability to Work in the Week After the 2011 Joplin Tornado
Determined by chi square.
Most (68.2%, n=407) reported that their youngest child was 10 years of age or younger, with 26.1% (n=156) having at least 1 child 3 years of age or younger. While there was no relationship between the age of the youngest child and whether or not hospital personnel actually worked, the perceived impact on willingness and ability to work the week after the tornado differed significantly by the age of the worker's youngest child [F (3, 24 and 3, 35)=3.2 and 4.8; p<0.05 and p<0.01, respectively]. Those whose youngest child was 3 years of age or younger reported the biggest perceived impact on willingness and ability to work compared to those whose youngest child was 11 to 17 years old (Table 5).
Impact of Age of Youngest Child on Hospital Personnel's Perceived Willingness and Ability to Work the Week After the Joplin Tornado
Likert-type scale: 1=no impact to 5=very significant impact.
Significant difference between age of youngest child being ≥3 years and age of youngest child being 11-17 years.
Alternative Childcare Plans
Of those with childcare responsibilities the week following the tornado (n=366), 61.2% (n=224) reported that they had an alternative childcare plan in place before the tornado. Of those with an alternative childcare plan (n=224), 59.8% (n=134) reported that they used this plan the week following the tornado. While having an alternative childcare plan in place was not significantly associated (in the regression analysis) with employees having actually worked the week following the tornado, those without alternative childcare plans in place prior to the tornado were significantly more likely to report that childcare needs had a significant impact on their perceived ability to work during the week following the tornado (43.7% vs 32.1%, X2=5.0, p<0.05). Finally, for those without prior alternative childcare plans in place (n=142), 45.7% (n=64) reported that they would have been more able and/or willing to work if they had had alternative childcare plans beforehand.
Significantly more individuals with childcare responsibilities reported having an alternative childcare plan in place after the tornado (82.2% current vs 61.2% pre-tornado, p<0.001). From logistic regression, the only significant predictor of having a post-tornado alternative childcare plan (at the time of the survey) was having a plan in place prior to the tornado [OR=57.1, CI (17.4–187), p<0.001]. Thus, the following were not significantly associated with having a post-tornado alternative childcare plan: demographic variables; hospital at which they were employed prior to the tornado; extent to which their home was damaged during the tornado; perceived responsibility for having alternative childcare plans; prior ICS training; personal preparedness before and after the tornado; perceived impact of childcare needs on willingness or ability to work; and attitudes toward alternative childcare if it had been offered by the hospital.
Impact and Cost of Alternative Childcare
Almost half (45.4%, n=166/366) of the respondents who indicated that they had childcare needs the week following the tornado reported that their usual childcare arrangements were in place the week after the tornado and that that was the only provider they used. Of the remaining respondents with childcare needs the week following the tornado, 30.5% (n=111) reported that, even though their usual childcare arrangements were in place and were used, they also needed to use alternative childcare in the week following the tornado, and an additional 24% (n=87) reported that none of their usual childcare arrangements were in effect (2 nonrespondents).
In addition, of the 366 respondents with childcare needs, 54.3% used alternative childcare solely or in combination with their usual care. These workers (n=198) were then asked the extent to which the use of alternative childcare affected their ability to work during the week following the tornado, costs associated with alternative childcare, and their level of concern about their child(ren)'s well-being and safety related to the use of alternative childcare. While 27.3% (n=54) reported that the need for alternative childcare had no impact on their ability to work, 56% (n=111) reported being able to work but with “slight to extreme difficulty,” and 8.6% (n=17) reported being “unable to work some or all of the time” during the week after the tornado because of lack of childcare.
When compared to a typical week preceding the tornado, 67.7% (n=113) reported their childcare costs were the same in the week after the tornado. Still, 20.3% (n=34) reported they paid an additional $1 to $100, and 12% (n=20) indicated that they paid an additional $100 or more. One quarter of the respondents (25%, n=43) also indicated that they were “somewhat to very concerned about their child(ren)'s well-being or safety” when using an alternative childcare provider or agency.
Impact of Altered Work Schedules on Those with Childcare Needs
Workers with children requiring childcare who were able to work the week of the tornado (n=311) were asked to describe the extent to which their schedule the week following the tornado affected their ability to find childcare. Most (86.8%, n=270) reported that their work schedule had no impact on their ability to obtain childcare, either because they worked their usual shift (46.6%, n=145) or because they were able to find childcare despite working a different shift in the week after the tornado (40.2%, n=125). Still, 11.6% (n=36) reported that working a different shift in the week after the tornado made it much harder to find childcare, and 1.6% (n=5) indicated that working a different shift made it easier to find childcare.
Impact of Home Damage
Of the 1,125 respondents who worked the week following the tornado, 13.1% (n=147) reported that they were unable to live in their damaged homes after the tornado, and 3.5% (n=36) added a text comment that their home had been completely destroyed in the disaster. In addition, 36.7% (429/1,170) reported having at least some damage to their home or loss of utilities; of those, 73.2% (n=314) lost power, 41.5% (n=178) lost water, and 12.4% (n=53) were without gas. Although the extent of home damage and loss of utilities were associated with decreased likelihood of working the week after the tornado when examined through univariate analysis, these variables were nonsignificant on multivariate analysis; only complete home destruction negatively affected actually working after the tornado.
Perceptions of Hypothetical Alternative Childcare
Hospital personnel who had childcare needs the week following the tornado were asked a series of questions related to their attitudes toward a hypothetical alternative childcare program. Of the 355 respondents:
• 51% (n=171) indicated that they would have used a hospital-provided alternative childcare service if their employer had offered it during the week following the tornado;
• Many (47.2% vs 42.4%, X2=201, p<0.001) felt an employer-based alternative childcare service would have increased their ability to work compared to increasing their willingness to work; and
• 41.5% (n=169) indicated that a hospital-provided alternative childcare service would have decreased their concern for their child(ren)'s well-being.
In addition, 44.9% (n=93/207) of respondents with a prior alternative childcare plan reported that they would have, nevertheless, used a hospital-provided childcare program had it been made available. When comparing those with and without alternative childcare plans prior to the tornado, hospital personnel who did not have a prior plan were significantly more likely to report that they would have used a hospital-provided alternative childcare service and that such a program would have increased both their ability and willingness to work and decreased their concern for their children (Table 6).
Alternative Childcare Plans and Attitudes Regarding Hospital-Provided Alternative Childcare Services
Denominator reflects missing/incomplete data.
Determined by chi square.
Finally, when respondents were asked who they believed had the primary responsibility to provide childcare for their children following disasters, the majority (77.9%, n=448/575) reported they believed that the employee had the primary responsibility for securing this childcare. Still, 22.1% (n=127) felt other agencies were responsible for providing emergency childcare; 11.1% (n=64) indicated the government or a relief agency had the responsibility; 8.7% (n=50) said the hospital had the primary responsibility; and 2.3% (n=13) thought the employee and employer hospital shared the responsibility equally.
Discussion
Following the EF5 tornado in 2011, healthcare workers in Joplin, MO, displayed incredible resilience, with the vast majority of the respondents reporting to work shortly after the disaster. Still, the healthcare workers in this study experienced very different events from a work environment perspective. One hospital was intact but experienced a significant patient surge, while the other was destroyed. This did have an impact on working during the week following the Joplin tornado, with those with full-time employment in the intact hospital being more likely to report to work. However, this difference did not have a significant effect on willingness to work in future disasters or personal preparedness. We did not explore the reasons behind this difference in this study, but we postulate that there were likely fewer actual positions for people to fill in the destroyed hospital.
Having an intact home was an important factor in reporting to work following the Joplin tornado. While many of those whose homes were completely destroyed did report to work, there were significantly fewer of them. This certainly makes sense in light of the divided responsibilities of work and a destroyed home. Hospital disaster planners might consider directing resources toward those with destroyed homes and part-time employees, as this may improve the hospital response in a real disaster.
Interestingly, hospital personnel who had childcare responsibilities were more likely to work the week after the tornado compared to those who did not have childcare responsibilities. Since the survey did not specifically address why these workers felt the obligation to come to work, we can only speculate on these reasons. Perhaps having financial dependents created a greater need to generate a paycheck, or perhaps those with childcare responsibilities felt more of a community obligation to come to work. A follow-up study would be required to address these speculations.
In this study, we found that healthcare workers expressed a greater willingness to work in a future natural disaster after having experienced one. This suggests that these workers may have gained further resilience for natural disasters because of their experiences. This resilience crossed all occupations, personal preparedness levels, and the physical impact on homes and places of work. However, this increased resilience did not extend to man-made and biological disasters, supporting the concept that experiencing one type of disaster may not necessarily increase healthcare workers' willingness to work following all disaster types. As other researchers have previously pointed out, healthcare personnel consider pandemics and dirty bombs to have a higher risk of personal harm compared to natural disasters, and this translates into less willingness to work during these events.3,23,24 Still, the data suggest that the experience itself appears to lead to this resilience rather than any particular demographic or disaster-related factor. For instance, prior training in ICS did not lead to increased personal preparedness nor alter willingness to work.
Despite the resilience demonstrated, healthcare workers at the survey hospitals went into the disaster with limited personal disaster preparedness both in terms of provisions and emergency care plans for their dependents. This was a concerning finding given that limited personal disaster preparedness has been linked to increased rates of seeking shelter during a tornado. 25 As might be expected, items commonly used in households outside of disasters, such as flashlights and first aid kits, were often in place, whereas more disaster-specific items, such as food and water stores, were reported less frequently. There were significant reported gains in all areas of personal disaster preparedness after the tornado, with some of the largest gains seen in emergency care plans for children, elders, and pets. Still, it is important for hospital planners to encourage healthcare workers to store water as part of their family disaster plans, as this was one of the lowest preparedness items, both before the Joplin tornado and 2 years after. In addition, prior work has demonstrated that, while home disaster preparedness increased in those exposed to a disaster threat, this was not sustained. 26 Our study was conducted 2 years following the real disaster, and it would be interesting to see if these results are sustainable over a longer time period.
While prior work suggests that disaster experience leads to increased confidence in nurses facing disasters, 27 the elevated concern for a disaster does not necessarily lead to increased personal preparedness. 28 Thus, one conclusion that might be drawn is that any opportunity to afford staff a realistic disaster experience may improve disaster response. Perhaps disaster preparedness education campaigns for hospital personnel might include personal stories from healthcare personnel who have already experienced a real disaster so these workers could better understand the importance of having a personal disaster plan. This, in turn, may help increase resilience among their healthcare colleagues.
In addition, having childcare responsibilities was the only other factor found to influence willingness to work in future tornados. More specifically, it was having childcare needs, not merely having childcare responsibilities, which significantly affected workers' perceptions. Thus, this group of healthcare workers with childcare needs will likely require more extensive planning and support to increase their resilience to future disasters.
Healthcare workers were more likely to have back-up care plans for their children compared to plans for elders or pets for which they have responsibility during a disaster. After the disaster, preparedness plans increased in all areas, but childcare still remained the area of most preparation. This may be due to the perception that pets are able to fend for themselves while children are not, but this is only postulated, because attitudes toward personal disaster planning were not examined in this survey. Unlike previous research,29,30 this study did not find a connection between having responsibility for children and overall personal preparedness, either before or after the tornado. There was also no association between post-tornado personal disaster preparedness and actually working the week following the tornado or willingness to work in future disasters.
During the week following the tornado, 45.6% of the caregivers were able to execute their normal childcare plans and 54.3% used alternative childcare plans solely or in combination with their usual care. When using alternative childcare, parents sustained a financial burden above and beyond their usual childcare costs, as well as an emotional cost: A quarter of parents reported increased concern for their children. Focusing on reducing the financial and emotional burdens for hospital workers may be the most productive approach for hospital-based disaster planners. For instance, the financial burden might be best addressed with a small stipend provided by the hospital. There are indications in the literature that providing added reimbursement to hospital workers for alternative childcare may result in increased willingness to work. 2 A stipend could also engender feelings of being “supported” by the hospital, a known encourager of willingness to work. 31
In addition, planners should encourage hospital employees to develop a childcare plan, as this may help reduce the stress of executing such plans following a real disaster. Maintaining normal shifts as much as possible during disasters may also help alleviate stress for employees: 53% of employees with children reported having different shifts than normal in the week following the tornado. Still, unlike prior work, this study showed that only 11.6% reported that working alternative shifts made it much harder to find childcare, thus calling into question the significance of this variable in causing additional stress for these workers.
Based on this and prior work, hospital planners can project that approximately half of their employees will be responsible for children following a disaster, and that approximately two-thirds will have children who will be unable to care for themselves (ie, age 10 and under). While this study could not establish an association with childcare needs and actually reporting to work, it was able to demonstrate, similar to previous work, that childcare concerns had a significant impact on workers' perceptions. This was especially true for those with the youngest children.
For this reason, hospital-provided alternative childcare would likely be popular among hospital workers with children, especially among those without existing alternative childcare plans. Still, if workers actually used such a hospital-provided program, the total number of families and children would be considerable. For instance, in a hospital with 2,000 employees, and assuming approximately 50% of the employees would have childcare responsibilities and approximately 50% of these employees would need to use such a program for just 1 of their children, it can be estimated that approximately 250 children would use such a program. Still, as far as feasibility, one report described the creation of a makeshift daycare facility that cared for a peak of 180 children following a hurricane. 32 While most employees in our study agreed that childcare responsibilities were primarily the responsibility of the employee, there was a significant minority who felt that it was the responsibility of the hospital, government, or relief agency to provide such a service. Thus, the feasibility of hospital-provided alternative childcare, perhaps in hospitals with existing childcare systems already in place and/or in partnership with community relief organizations, deserves further consideration.
This is the first study to assess hospital personnel's willingness to report to work before and after a real disaster, and the first to assess resilience in relation to personal disaster preparedness. It is also the first examining the details of how childcare needs affect healthcare workers' perceptions following a real disaster. Still, some limitations must also be noted. All data, including pre-Joplin tornado willingness to work, were collected 2 years after the 2011 Joplin tornado; this may introduce some recall bias, especially with respect to the respondents' reported willingness to work before the actual disaster. Also, with a 23.4% response rate, this study may have some selection bias in that those most interested in disaster preparedness and/or response may have been more likely to participate; it is possible that nonresponders would have answered the survey questions differently than those who chose to participate. It is also possible that some hospital personnel who lived in Joplin during the tornado no longer live there and thus may not be in the sample. Finally, these findings may have limited generalizability, since all data were collected from healthcare workers in Joplin, Missouri, and may not reflect the perceptions of workers in other parts of Missouri or in other states who have likewise experienced real disasters.
Conclusion
After experiencing a real disaster, 88% of healthcare workers reported to work, demonstrating true resilience. Healthcare workers expressed a greater willingness to work in future natural disasters, but not in man-made or biological events. More research is needed to determine factors influencing healthcare workers' personal preparedness so that resources can be directed to those who would most likely benefit. Those with childcare needs reported less willingness to work in future disasters, and the perception of childcare needs appears to have placed an emotional and financial burden on these workers. Disaster planners should be aware of these perceptions as they formulate their own emergency operation plans.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.