
Abstract
The Global Health Security Agenda's objectives contain components that could help health departments address emerging public health challenges that threaten the population. As part of the agenda, partner countries with advanced public health systems will support the development of infrastructure in stakeholder health departments. To facilitate this process and augment local programs, state and local health departments may want to include concepts of health security in their public health preparedness offices in order to simultaneously build capacity. Health security programs developed by public health departments should complete projects that are closely aligned with the objectives outlined in the global agenda and that facilitate the completion of current preparedness grant requirements. This article identifies objectives and proposes tactical local projects that run parallel to the 9 primary objectives of the Global Health Security Agenda. Executing concurrent projects at the international and local levels in preparedness offices will accelerate the completion of these objectives and help prevent disease epidemics, detect health threats, and respond to public health emergencies. Additionally, future funding tied or related to health security may become more accessible to state and local health departments that have achieved these objectives.
The Global Health Security Agenda's objectives contain components that could help health departments address emerging public health challenges. State and local health departments may want to include concepts of health security in their public health preparedness offices in order to simultaneously build capacity. This article identifies objectives and proposes tactical local projects that run parallel to the primary objectives of the GHSA. Executing concurrent projects at the international and local levels in preparedness offices will accelerate the completion of these objectives and help prevent disease epidemics, detect health threats, and respond to public health emergencies.
T
The GHSA is an ambitious step toward addressing the emerging public health challenges that threaten the global population; however, the agenda's principal objectives primarily focus on capacity building by the US federal government and other international leaders. A top-down investment begins the process. To facilitate this process, state and local health officials who aim to meet these standards may consider implementing a health security program in their jurisdiction in order to concurrently build capacity from the bottom up. These agencies can also address current gaps in their preparedness offices by developing projects with intersecting objectives.
Implementing Health Security at the Local Level
Capability and capacity building will be needed to establish the foundation of global health security. Participating health departments that are building public health programs should also consider implementing a localized health security program. The method of implementing this program will be as important as the objectives themselves. In addition to capability building, a successful health security program will incorporate a multidisciplinary coordinating function. Many of the objectives of health security involve engaging nontraditional public health partners, analyzing data and information in new ways, and augmenting typical public health operations.
Budget restrictions and limited staffing will make it difficult for health departments to create new offices without additional funding. Many health departments might choose to include health security objectives in an existing office with a similar mission. In many instances, this will be a public health preparedness office.
There are similarities between the core capabilities of public health preparedness and the outlined objectives of health security. As the emergency management branch of public health, preparedness offices must coordinate action plans and projects in a multidisciplinary fashion. Many of the stakeholder agencies in the GHSA are current partners of these offices at the state and local levels. Furthermore, the GHSA objectives are priority areas that assume that some basic public health capabilities exist, including epidemiologic surveillance, laboratory testing, medical materiel management, and basic emergency operations coordination. These core functions are closely aligned with many of the capabilities outlined in the Centers for Disease Control and Prevention (CDC) Public Health Preparedness Capabilities, which dictate the actions of many health preparedness offices. 2 Each of the health security projects proposed in this article are related to specific resource elements outlined in the preparedness capabilities that state and local health departments must address.
A natural place in a health department for a health security program might be in its preparedness office. Current federal grants that support public health preparedness offices, including the CDC Public Health Emergency Preparedness (PHEP) and the Assistant Secretary for Preparedness and Response (ASPR) Hospital Preparedness Program (HPP) Cooperative Agreements, provide guidance for these offices to incorporate characteristics closely related to health security. The HPP and PHEP funding opportunity announcement for budget period 3 (FY2014) outlines specific requirements for awardees that are related to health security. One is a joint requirement that dictates that awardees shall “support integration with [a] daily healthcare delivery system.” Another PHEP requirement states that awardees shall “coordinate with cross-cutting public health preparedness partners.” 3
There are additional international agreements that support the development of a health security program—most notably, the International Health Regulations (IHR), which is an agreement among nearly 200 nations to protect against the spread of disease. 4 Future guidance and grants may incorporate public health security. By creating a health security program now, state and local health departments would be better organized to meet future grant guidelines and federal mandates. In the meantime, individual projects can be tailored to include elements of both health security and PHEP or HPP requirements. This would be building capacity and reducing gaps at little or no additional cost to the health department, and these gaps, if not addressed, could further complicate future public health emergencies, which would be costly in money, staff time, and lives.
The recent international commitment to health security indicates that the topic is relevant. Its importance goes beyond international boundaries; however, the threats related to health security would directly affect a state, locality, or province. It is important that they are prepared for these threats. For this reason, health departments have a justification for integrating health security programs into preparedness programs. These departments should implement health security programs concurrently as federal and international entities commence the GHSA. This method will help health departments expedite the completion of the GHSA objectives and ensure that they are operating at full capacity to prevent, detect, prepare for, and respond to health threats at the state and local levels.
To accomplish this, state or local health security programs would need to be closely aligned with the international GHSA. The objectives, and the projects instituted to meet these objectives, would need to run parallel across the 3 mission areas of prevention, detection, and response. The GHSA international partners focus on developing and enhancing systems and coordinating information among governments. 1 A local program would need to focus on developing relationships, skill sets, policies, and capacities to support these systems that would enable information sharing. The following is a set of 9 proposed objectives in the prevention, detection, and preparedness and response areas that state, local, or provincial health departments could focus on while creating a health security program. These objectives are related to those outlined in the GHSA (Figure 1) and would facilitate completing the objectives of the GHSA while helping to meet current public health preparedness funding requirements.
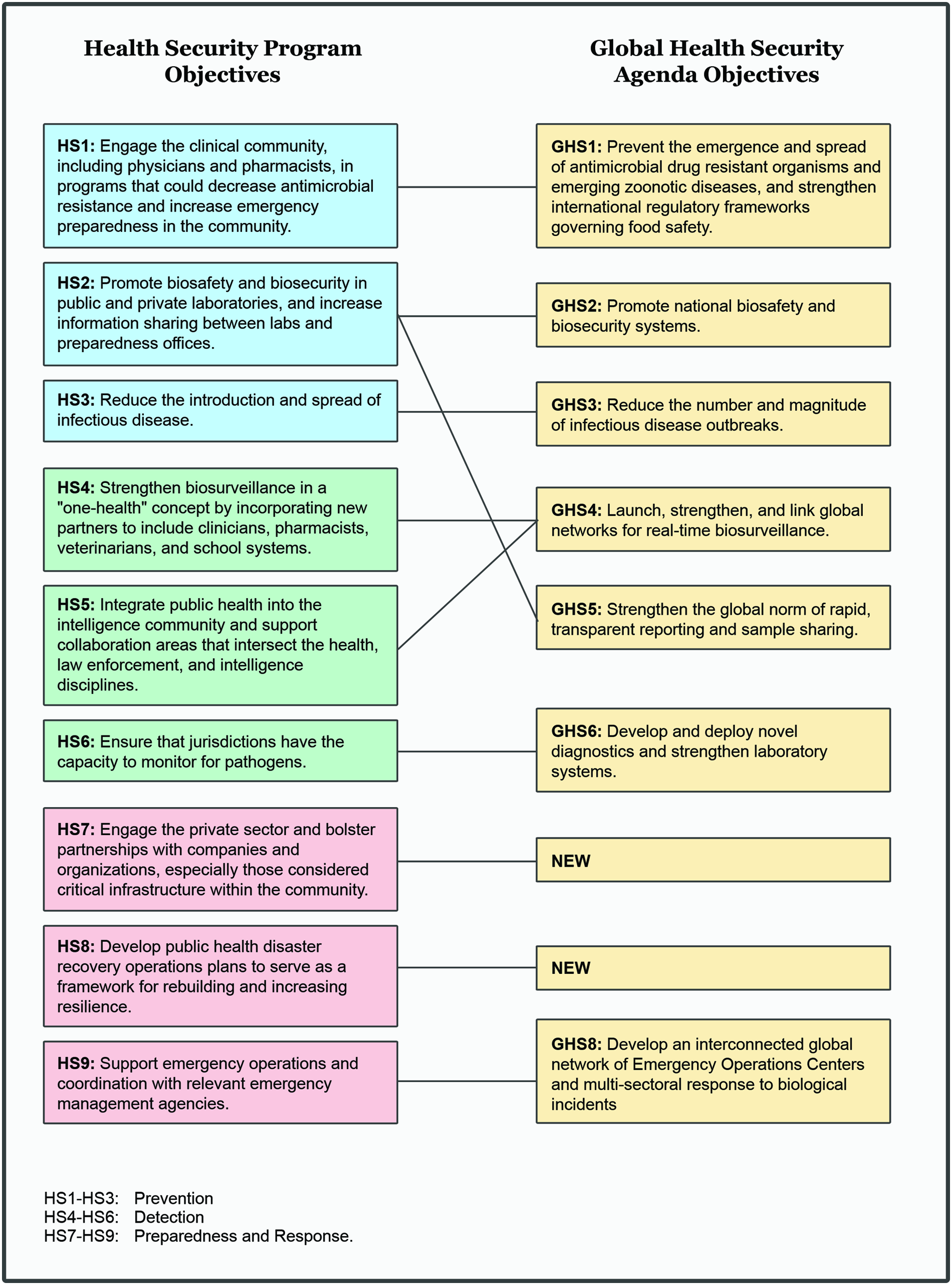
Comparison of the 9 health security program objectives outlined in this article and the objectives of the GHSA. Color images available online at www.liebertpub.com/bsp
Prevention
Any public health emergency or disease epidemic that is prevented is one that cannot affect people's health. Jurisdictions that work on prevention practices may benefit by seeing a reduction in the cost and impact of future public health emergencies on the health department and residents. There are at least 3 specific, achievable objectives that could bolster the prevention mission area in a health security program. These objectives, outlined below, include engaging the clinical community, promoting biosecurity and information sharing, and reducing the spread of disease.
• Engage new partners in the clinical community, including physicians and pharmacists, in programs that could decrease antimicrobial resistance. CDC has identified resistance to antibiotics as one of the chief global threats facing the US and the world. Many infections from antimicrobial resistant bacteria are becoming common and cannot be effectively treated. 5 CDC cites appropriate prescribing, administration, and stewardship of antibiotic medications as “the single most important action needed to greatly slow down the development and spread of antibiotic-resistant infections.” 5 Public health departments should develop and refine antibiotic and antiviral medication prescription guidance and conduct appropriate outreach activities to clinicians. Developing guidance to pharmacies and increasing partnerships with clinicians are dictated in CDC's preparedness capabilities. Perhaps more important, health departments should consider training clinicians in antibiotic stewardship. A secondary consequence would be that health departments could include emergency preparedness training and material to clinicians in tandem. Recent studies and reports, such as Rubin et al, 6 demonstrate that the general continuum of care is being expanded to include additional clinical services, such as pharmacists. Public health departments should consider including pharmacies and pharmacists in any program aimed at reducing antimicrobial resistance and increasing emergency preparedness.
• Promote biosafety and biosecurity in public and private laboratories, and increase information sharing between laboratories and emergency preparedness offices. Microorganisms continue to evolve and threaten human beings; therefore, continued laboratory and scientific research with infectious microorganisms with the purpose of identifying and countering these organisms remains necessary. 7 Although such research is needed, it is important to understand that some risks, such as laboratory-acquired infections and accidental environmental release, cannot be completely eliminated. 7 Health departments should take the lead in reducing these risks by formulating comprehensive biosafety and biosecurity programs and reports. These programs should have multisectoral and multidisciplinary stakeholders that could include public advocacy groups, academia, the biotechnology industry, and relevant government agencies and laboratories. Emergency management and preparedness agencies will also be essential partners, as they often are expert in both predisaster mitigation projects and postdisaster response operations. These collaborative planning efforts related to biosafety and biosecurity will foster relationships between the agencies in the multidisciplinary workgroup. This could pay future dividends in health security during a biosecurity or bioterrorism incident that demands information sharing among all of these organizations.
• Reduce the spread of infectious disease by implementing prevention programs. Novel viruses and bacteria form as microorganisms continue to evolve. To reduce the introduction of disease and mitigate the consequences of future epidemics, it is important that health departments develop work groups that focus planning efforts on diseases emerging outside of the department's jurisdiction. Currently, this could include the Middle East respiratory syndrome coronavirus (MERS-CoV), avian influenza A (H7N9) virus, or the recent outbreak of Ebola virus disease. Participating in international disease surveillance is the first step necessary to developing the first line of defense, which includes infection control guidance, precautions, and practices for international ports of entry. In addition to health department work groups, it is essential that planning among these ports and public health agencies occurs. Some ports may have developed operational plans for isolating and quarantining passengers who exhibit symptoms of some specific communicable diseases; however, it is equally necessary to have protocols outlining communication pathways between airports, seaports, and rail stations and appropriate government agencies. This facilitates threat assessment, prevents the introduction of disease, and mitigates disease spread and the impact of an epidemic on local resources.
Detection
Rapid detection of disease and dissemination of intelligence and information related to public health emergencies mitigate the consequences of these incidents. There are 3 objectives that focus on detection and information sharing: strengthening multidisciplinary biosurveillance, integrating the public health and intelligence communities, and augmenting monitoring systems.
• Strengthen biosurveillance by incorporating new partners, including clinicians, pharmacists, veterinarians, environmental health experts, and school system leaders. Traditional epidemiologic surveillance is one of the basic foundations of public health. Many health departments that have established these epidemiologic processes have also added syndromic surveillance systems, which monitor and quantify disease indicators such as patient symptoms or chief complaints. 8 These indicators remain the basis of syndromic surveillance, but opportunities exist for incorporating additional data sources and linking other, existing surveillance systems outside of the healthcare sector. Some examples are zoonotic disease data from agricultural agencies, behavioral health risk factor information, prescription information or drug-monitoring information from pharmacies, data related to climate change, and student absenteeism data from school systems. These data exist and are being collected. The opportunity for health security programs is to include and analyze this information in new ways to produce health-related detection triggers that do not currently exist.
• Integrate public health systems into the intelligence community and support collaboration areas that intersect the health, law enforcement, and intelligence disciplines. Preventing attacks on the homeland is one of the primary objectives listed in the National Security Strategy. 9 One method for accomplishing this is continuing to develop state and urban area fusion centers that actively share classified and unclassified information related to crimes and terrorism and reports related to suspicious activity. 9 Although there are many law enforcement–centric data programs related to counterterrorism in place in the US, Europe, and other countries, there is an opportunity for public health agencies to include their data, especially biosurveillance and laboratory information, in these programs. Early disease detection could inform law enforcement and intelligence officers of a potential emergency or attack. These data also can be used during investigations and to determine attribution. This information can be analyzed at the health department and issued to intelligence centers, or a health analyst can be placed in a fusion center to analyze health-related data and information. This partnership would also facilitate information sharing during a potential nefarious attack that necessitates public health input, such as a biological or chemical incident. These attacks typically require laboratory testing to confirm the presence of an agent. Specific information related to the attack provided by law enforcement or intelligence entities allows public health laboratories to specify assessments and hasten both total testing time and results. In this case, rapid detection enables actionable results, which allows for a quicker public health response.
• Ensure that jurisdictions have the capacity to monitor for pathogens. Traditional laboratory and epidemiologic detection systems, such as environmental testing and syndromic surveillance, are the backbone of public health monitoring; however, states and localities are the political jurisdictions in which public health staff, scientists, and academics reside. There are many opportunities for these practitioners to develop novel diagnostics and epidemiologic systems. These could include sensor systems with on-site analysis capabilities. Novel monitoring programs could also include collaboration with nongovernment organizations and private companies who develop new ways of detecting disease and programs that can predict or identify health threats through the analysis of data or social media.
Preparedness and Response
Predisaster preparedness planning and response to public health threats are essential to reducing the negative health consequences associated with an emergency. There are 3 objectives that focus on preparedness and response: engaging the private sector before and during incidents, developing public health disaster recovery operations plans, and supporting emergency operations in response to a disaster.
• Engage the private sector and bolster partnerships with companies and organizations in the community, especially those considered critical infrastructure. Private sector organizations often comprise the center of a community. Approximately 91.9% of employed people who do not work at home are employed in a business that is not considered a “long commute.” 10 Many people work at or near their community, and all employed people work within a community. It is essential that these organizations be included in community resilience planning being conducted by government agencies. Many employers already have emergency or contingency planning divisions, but these programs may not include employee health. Employers also have an active interest in their employees' health. Public health departments should engage the private sector on multiple fronts. This could include incorporating private partners in situational awareness related to residents' health, creating and disseminating a health security newsletter related to employee health, participating in regular meetings hosted by contingency planning associations, working alongside existing critical infrastructure protection programs, and allowing the private sector to participate in government-sponsored preparedness drills, exercises, and real-world events. In turn, companies may be more likely to include employee health considerations, such as advancing sick leave or time off during an infectious disease outbreak or epidemic, in contingency planning.
• Develop public health disaster recovery operations plans to serve as a framework for rebuilding communities and increasing resilience. A secure jurisdiction would need to not only respond to a disaster but also be prepared to recover from any incident that has an impact on the health and well-being of its residents. Operational recovery plans focus on how government agencies can work to “restore, redevelop, and revitalize” communities and build resilience after a disaster. 11 Public health agencies should develop recovery plans that focus on the restoration of healthcare services and ensure that affected residents have access to these services and health-related information following a disaster. A completed plan for community recovery helps build resilience. Perhaps more important, a public health recovery plan that includes an impact assessment of the healthcare system and steps to recover from these effects will reduce negative health outcomes following an emergency. Public health recovery plans should include health impact assessments and provisions for epidemiologic, laboratory, environmental health, and healthcare systems.
• Support emergency operations and coordination with relevant emergency management agencies. Rapid public health response to emergencies is imperative to reduce consequences. Nearly every emergency affects residents' health in some way. For this reason, it is critical that public health agencies are actively engaged in emergency operations for the jurisdiction throughout the entire process. Local, state, and jurisdictional public health programs should provide subject matter expertise during incidents to affirm that a primary goal of any emergency response is to maintain or strengthen public health. Health departments should focus on the local equivalent of the critical functions of emergency response for public health as outlined by the World Health Organization. This includes acting as the jurisdictional health decision-making leader; collecting, analyzing, and disseminating health-related information; providing technical expertise appropriate to the jurisdiction's health needs to emergency managers; and ensuring that core health services remain available to a community during a disaster. 12 Partnerships with emergency management agencies and political leaders formed prior to an emergency will ensure that public health agencies have an appropriate role during the response to an emergency.
Conclusion
The GHSA provides a focused approach to building uniform health security capabilities in public health departments. The technical assistance provided by the countries leading this effort should be beneficial to public health department operations and residents' health. Much of the international aid and program guidance is focused on high-level attributes in broad categories. 13 This mode is useful for international stakeholders with public health programs with varied capacities who need a degree of latitude while developing and augmenting systems. The top-down approach of providing expertise, and the associated resources available during the 5-year international commitment to the GHSA, will almost certainly improve the status of international and local health security. Still, there is a need for state, local, provincial, and jurisdictional health departments to concurrently outline and implement an explicit health security program from the bottom up. Localized health security projects that meet the programs outlined in the international GHSA in the middle will accelerate the completion and success of the GHSA. Public health preparedness offices in health departments have the opportunity to include the concepts of health security in future projects. This, in turn, will help partner nations and the world prevent avoidable disease epidemics, detect public health threats, and respond to public health emergencies.