
Abstract
Background:
Patients with rheumatoid arthritis (RA) experience joint swelling and cartilage destruction resulting in chronic pain, functional disability, and compromised joint function. Current RA treatments, including glucocorticoid receptor agonists, produce adverse side effects and lack prolonged treatment efficacy. Cannabinoids (i.e., cannabis-like signaling molecules) exert anti-inflammatory and analgesic effects with limited side effects compared to traditional immunosuppressants, making them excellent targets for the development of new arthritic therapeutics. Monoacylglycerol lipase (MAGL) inhibition reduces inflammation in mouse models of acute inflammation, through cannabinoid receptor dependent and independent pathways. The current study investigated the efficacy of inhibiting synthetic and catabolic enzymes that regulate the endocannabinoid 2-arachidonoylglycerol (2-AG) in blocking paw inflammation, pain-related behaviors, and functional loss caused by collagen-induced arthritis (CIA).
Methods:
Male DB1A mice subjected to CIA were administered the glucocorticoid agonist dexamethasone (DEX), MAGL inhibitor JZL184 (8 or 40 mg/kg, s.c.), alone or in combination, or diacylglycerol lipase β (DAGLβ) inhibitor KT109 (40 mg/kg, s.c.). CIA-induced deficits were assayed by arthritic clinical scoring, paw thickness measurements, and behavioral tests of pain and paw function.
Results:
DEX or dual administration with JZL184 reduced paw thickness and clinical scores, and JZL184 dose-dependently attenuated grip strength and balance beam deficits caused by CIA. Traditional measures of pain-induced behaviors (hyperalgesia and allodynia) were inconsistent. The antiarthritic effects of JZL184 (40 mg/kg) were largely blocked by coadministration of the CB2 antagonist SR144528, and the DAGLβ inhibitor KT109 had no effect on CIA, indicating that these effects likely occurred through CB2 activation.
Conclusions:
MAGL inhibition reduced paw inflammation and pain-depressed behavioral signs of arthritis, likely through an endocannabinoid mechanism requiring CB2. These data support the development of MAGL as a target for therapeutic treatment of inflammatory arthritis.
Introduction
Rheumatoid arthritis (RA) is a debilitating autoimmune disorder characterized by chronic inflammation, swelling, cartilage destruction, and pain in the synovial joints.1–3 Earlier in the disease progression, pain has a higher correlation with functional disability compared to joint destruction alone, but joint destruction is highly correlated with disability as the disease progresses.4,5 Immunosuppressants, such as disease-modifying antirheumatic drugs or biological therapies, are the main treatment for RA, but can induce aversive side effects, and patients often experience pain despite improvement in inflammation.6–8 Synthetic glucocorticoid agonists are often prescribed to RA patients for prompt suppression of pro-inflammatory mediators.9–11 Despite the therapeutic potential of glucocorticoid agonists, the magnitude of nonspecific immunosuppression and endogenous glucocorticoid feedback insensitivity that they facilitate can become dangerous. 12
Alternative treatments, including cannabinoid receptor agonists, have been used by some patients to treat symptoms of chronic inflammatory pain by activating cannabinoid subtype 1 (CB1) and subtype 2 (CB2) receptors.13,14 While CB1 is expressed throughout the body, and in high levels in neural tissues, CB2 is expressed on peripheral immune cells, activated microglia, and at low levels in the brainstem and is responsible for the anti-inflammatory effects of cannabinoids. 15 Increased levels of the endogenous cannabinoids (i.e., endocannabinoids) 2-arachidonylglycerol (2-AG) and anandamide and both CB receptors are found in the synovial joints of RA patients,16,17 whereas synovial lymphocytes and monocytes of RA patients express CB2.18–20 Furthermore, the oromucosal mouth spray Sativex, which contains a mixture of the Cannabis extracts Δ 9 -tetrahydrocannabinol (THC) and cannabidiol (CBD), decreases self-reports of RA-induced pain in humans. 21 But clinical application of nonselective cannabinoid agonist treatments is limited by undesirable side effects, including somnolence and cognitive impairment, occurring at clinically relevant doses. 22
Modulation of the endocannabinoid system is an alternative strategy to direct CB receptor agonism that has the potential to circumvent the common side effects of cannabinoid agonists. The endocannabinoid 2-AG is primarily degraded by the catabolic enzyme monoacylglycerol lipase (MAGL). 23 Repeated pharmacological inhibition of MAGL attenuates acute mitogen-induced paw inflammation and preclinical models of hyperalgesia, neuropathic pain, and chemotherapy-induced pain.24–26 However, repeated high doses of MAGL inhibitors induce physical dependence and CB1 receptor functional tolerance.27–29
The synthetic glucocorticoid receptor agonist dexamethasone (DEX) reduces inflammation in the collagen-induced arthritis (CIA) model. 30 A combination of DEX and the anti-inflammatory cytokine IL-4 attenuates CIA-induced paw inflammation and prevents the resurgence of CIA-induced paw swelling after treatment is terminated.31,32 These data indicate that combination therapies may limit the need for long term use of glucocorticoids, thereby reducing undesirable side effects. 31 Furthermore, combinations of nonsteroidal anti-inflammatory drugs or gabapentin and MAGL inhibitors attenuate neuropathic pain at doses lower than either drug by itself.33,34 The current study was designed to determine the antiarthritic effects of the MAGL inhibitor JZL184, the synthetic glucocorticoid DEX, or a combination of the two, as well as the diacylglycerol lipase β (DAGLβ) inhibitor KT109, in decreasing the inflammatory and behavioral/functional deficits caused by collagen induced arthritis.
Materials and Methods
Animals
Male DBA/1J mice (Jackson Laboratories, Bar Harbor, ME) 9–12 weeks old were randomly assigned to all treatment conditions. Females were excluded because they resist developing CIA.35–37 Mice were housed 3–5 per cage in polysulfone cages on corn cob bedding in an AAALAC International accredited facility on a 12-h light/12-h dark cycle maintained at 21°C±1°C and 50%±5% humidity. The Institutional Animal Care and Use Committee at West Virginia University approved all experimental protocols. All testing was conducted during the light phase, by an experienced experimenter blinded to the treatment conditions.
Collagen-induced arthritis
Under isoflurane anesthesia (Phoenix Pharmaceuticals, Burlingame, CA), 100 μL of an emulsion of bovine type II collagen (2 mg/mL) (Chondrex, Inc., Redmond, WA), dissolved in 0.05 M acetic acid, in an equal volume of complete Freund's adjuvant (CFA) was injected intradermally, ∼1 cm from the distal end of the tail. Twenty-one days later,38,39 mice received a second “booster” exposure to the collagen emulsion, in an equal volume of incomplete Freund's adjuvant (IFA), injected midway between the tail base and first exposure site. Control mice received an emulsion of IFA and acetic acid without collagen for both injections. CFA consisted of heat inactivated Mycobacterium tuberculosis (4 mg/mL) (Difco Laboratories, Detroit, MI), 85% heavy mineral oil (O122–1; Fisher Scientific, Pittsburgh, PA), and 15% mannide monooleate (AC332130250; Fisher Scientific). The IFA was prepared identically but without M. tuberculosis.
Drugs
The MAGL inhibitor JZL184 was purchased from Cayman Chemical (Ann Arbor, MI). The selective CB2 receptor antagonist SR144528 (SR2) was generously provided by the NIDA Drug Supply Program (Bethesda, MD). The DAGLβ inhibitor KT109 was synthesized in the Hsu laboratory, as previously published. 40 The synthetic glucocorticoid DEX was purchased from Sigma-Aldrich (St Louis, MO). All drugs were dissolved in a vehicle solution of 5% ethanol, 5% Kolliphor EL (Sigma-Aldrich), and 90% normal saline. 41 All solutions were injected subcutaneously at a volume of 10 μL/g body mass. All compounds were injected starting the day of the collagen booster immunization, continuing daily. SR144528 was injected 30 min before JZL184. In the combination experiment, JZL184 and DEX were administered separately. Mice in control conditions received vehicle.
Clinical scores
After the “booster” injection, forepaws and hind paws were examined daily using a clinical scoring system commonly used in the CIA model39,42–45 that quantified the magnitude of paw inflammation by assigning the numbers 0–4 to qualitative categories as follows: 0, normal; 1, erythema and mild swelling confined to the ankle joint or toes; 2, erythema and mild swelling extending from the ankle to the midfoot or ankle joint; 3, erythema and moderate swelling extending from the ankle to the metacarpal/metatarsal joints; and 4, erythema and severe swelling encompassing the ankle, foot, and digits. The scores for each limb were summed for each mouse, resulting in a composite arthritis score with a maximum of 16 total points.
Paw thickness
Hind-paw thickness (i.e., the distance between the plantar surface and dorsum, as measured between the walking pads) was measured to the nearest 0.01 mm using a digital micrometer. 42 The mean of the hind-paw measures for each mouse was used for analysis presented as change from initial “booster” measurement. Hind-paw thickness is a prevalent measurement of CIA-induced paw swelling, particularly in mice,39,42–44 which have small ankle joints that are difficult to measure, and research suggests that a micrometer is more accurate than plethysmometer in measuring small changes in mice paw edema. 46
Mechanical allodynia
On test days, mice were brought into the testing room, weighed, and injected. Immediately afterward, mice were placed in ventilated polycarbonate chambers (7.5×9 cm) on an aluminum mesh table and acclimated for at least 60 min before testing. 47 Mechanical allodynia was tested by stimulating the plantar surface of each mouse hind paw with von Frey filaments ranging 0.16–6 g (North Coast Medical, Morgan Hill, CA) using the “up-down” method.33,48
Thermal Hyperalgesia
Mice were placed in ventilated polycarbonate chambers (7.5×9 cm) on a glass table and acclimated for at least 60 min before testing. 49 A custom-built plantar stimulator with a noxious heat source (the focused beam of a red incandescent projector light bulb) was positioned directly beneath the hind paws of each mouse, heating the glass table, and the latency for the mouse to lift its paw from the glass was recorded.49,50 A 20 s cutoff time was used to avoid the possibility of tissue damage.42,49
Grip strength
Individual mice were placed on a metal cage top that was gently inverted over a padded surface.51,52 Mice were then suspended upside down for a maximum of 60 s, and the latency to fall from the metal cage top was used as a measure of grip strength. The task was performed every other day, and the highest score over three trials, each separated by 300 s, was used for analysis.
Balance beam
The balance beam test assesses mouse motor performance and coordination. 53 Mice were placed on the end of a 0.6 to 2.5 cm wide 100 cm long beam suspended 50 cm above the bench. Mice were given three trials to traverse an 80 cm length of the beam within a 60 s maximum trial time. All four paws had to pass the starting and finishing line to activate and inactivate the time, respectively. A bright light was directed toward the starting platform, and a black escape box filled with food and nesting materials was positioned at the other end. Mice were tested at baseline and on day 14 postbooster.
Statistical analyses
All data were analyzed by ANOVA, followed by Bonferroni post hoc comparisons. Data for clinical scores, edema, grip strength, and balance beam were compared using two-way mixed ANOVA, with experimental treatment as a between-subjects variable and days postbooster as a within-subject variable. All other behavioral data were analyzed using one-way ANOVA. All data are represented as mean±SEM with α=0.05.
Results
JZL184 does not potentiate DEX attenuation of CIA-induced paw swelling
Subeffective doses of DEX and JZL184 (Supplementary Fig. S1) were administered together to assess potential additive antiedematous and analgesic effects. Mice were administered the MAGL inhibitor JZL184 (4 mg/kg), the steroid DEX (0.015625 mg/kg), a combination of JZL184 (4 mg/kg) and DEX (0.015625 mg/kg), or vehicle subcutaneously once daily for 19 consecutive days. Coadministration of JZL184 and DEX attenuated CIA-induced clinical scores, while DEX alone attenuated clinical scores [F(72,738)=5.842; p<0.0001; Fig. 1A] and CIA-induced paw swelling, as per caliper measurements [F(72,738)=3.152; p<0.0001; Fig. 1B]. CIA did not alter the paw withdrawal thresholds in the von Frey test [F(4,41)=2.154; p=0.0914; Fig. 1C] or induce thermal hyperalgesia [F(4,41)=1.625; p=0.1862; Fig. 1D], as tested 18 days postbooster. Lacking a CIA pain effect, there was no significant attenuation of pain-related behaviors by JZL184, DEX, or JZL184/DEX.

Repeated dual administration of the steroid dexamethasone and MAGL inhibitor JZL184 attenuates CIA-induced paw swelling. Mice were administered JZL184 (4 mg/kg; s.c.), DEX (0.015625 mg/kg; s.c), JZL184 (4 mg/kg; s.c.) + DEX (0.015625 mg/kg; s.c.), or vehicle once daily for 19 days. DEX or JZL184/DEX attenuated CIA-induced arthritic clinical scores
High dose JZL184 attenuates CIA-induced paw swelling and behavioral functional deficits
The effects of a high dose of JZL184 (40 mg/kg) on CIA-induced paw swelling and functional deficits were assessed. Because CIA effects approached asymptote by day 12 postbooster in the previous experiments, we shortened the timeline to 2 weeks postbooster. After the booster immunization mice were administered JZL184, SR144528 (3 mg/kg) + JZL184, or vehicle once daily. JZL184 lowered CIA-induced clinical scores [F(45,495)=4.079; p<0.0001; Fig. 2A] and hind-paw thickness [F(45,495)=3.329; p<0.0001; Fig. 2B]. The CIA mice coadministered JZL184+SR2 differed from control mice in paw swelling (p<0.05; Fig. 2A) and paw thickness (p<0.01; Fig. 2B). Paw thickness but not clinical scores in JZL184+SR2-treated CIA mice differed from JZL184-treated CIA mice, suggesting partial attenuation of anti-inflammatory effects (Fig. 2A, B). CIA-induced grip strength functional deficits were detected starting at day 7 postbooster [F(21,231)=2.593, p<0.001; Fig. 2C], whereas mice coadministered JZL184+SR2 showed no differences from controls. JZL184 prevented CIA-increased latency to cross the balance beam [F(3,33)=4.424, p<0.05; Fig. 2D], and this functional deficit was not present in the JZL184+SR2 group, suggesting that the JZL184 effects are likely mediated by a CB2 mechanism.
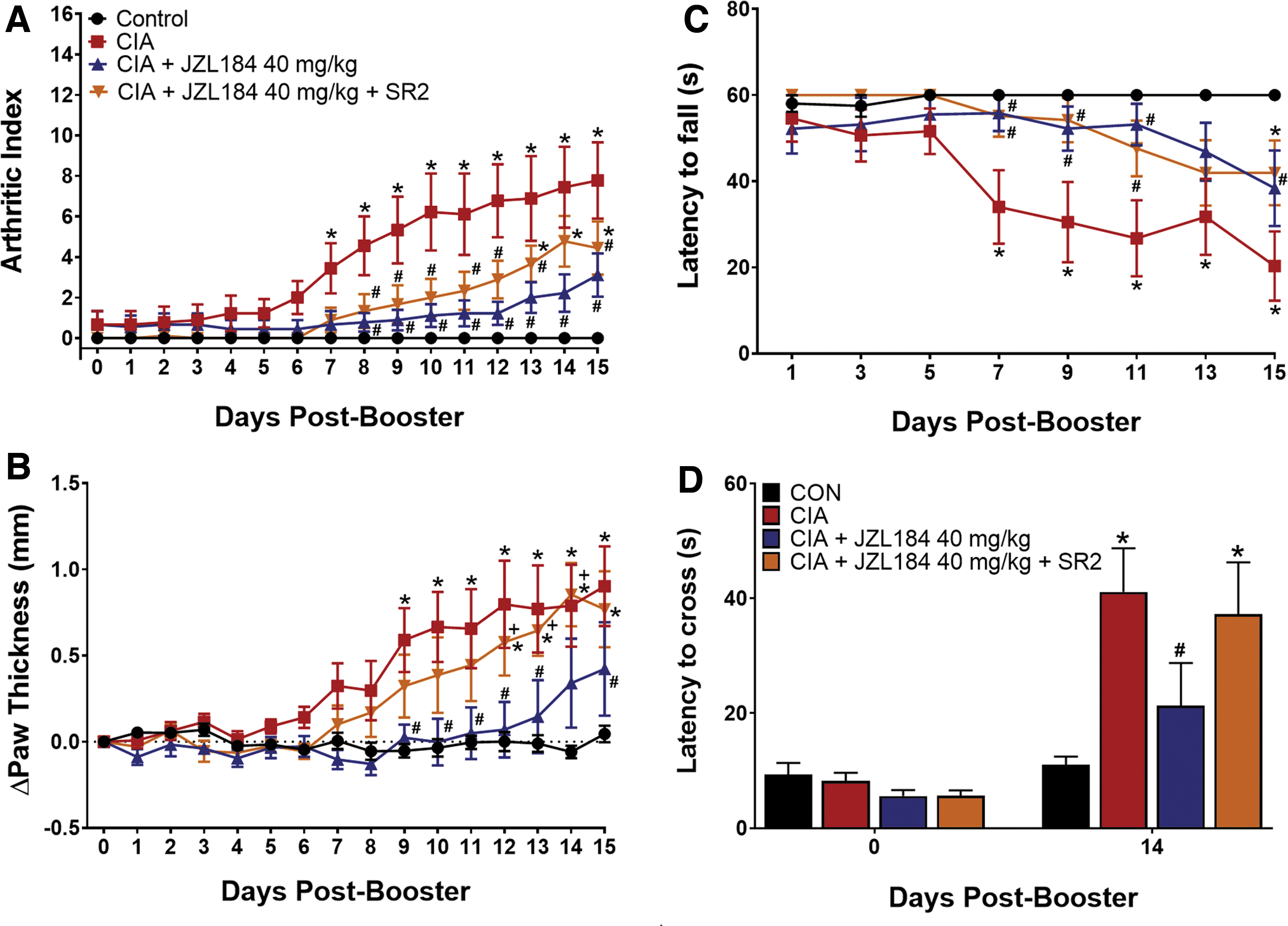
MAGL inhibition attenuates CIA-induced paw swelling and pain-depressed behaviors. Mice were administered JZL184 (40 mg/kg), JZL184 (40 mg/kg) + SR144528 (SR2; CB2 antagonist; 3 mg/kg), or vehicle (sc) for 16 days starting at the booster. SR2 blunted the efficacy of JZL184 (40 mg/kg) to attenuate CIA as measured by arthritic clinical scores
In addition to indirectly activating cannabinoid receptors by increasing available 2-AG, MAGL inhibition through JZL184 decreases arachidonic acid precursors of prostanoid synthesis, resulting in cannabinoid receptor-independent anti-inflammation. To assess possible cannabinoid receptor-independent effects of JZL184 in the CIA model, we repeatedly administered the DAGLβ inhibitor KT109 (40 mg/kg), which had no effect on either CIA-induced clinical scores [F(30,420)=8.075, p<0.0001; Fig. 3A] or paw thickness [F(30,420)=4.207, p<0.0001; Fig. 3B]. As in the previous experiment, CIA decreased grip strength (F(14,196)=6.459, p<0.0001; Fig. 3C). Surprisingly, KT109 exacerbated the decreased latency to fall in CIA-treated mice. KT109 had no effect on latency to traverse the balance beam [F(2,30)=7.891, p<0.01; Fig. 3D].
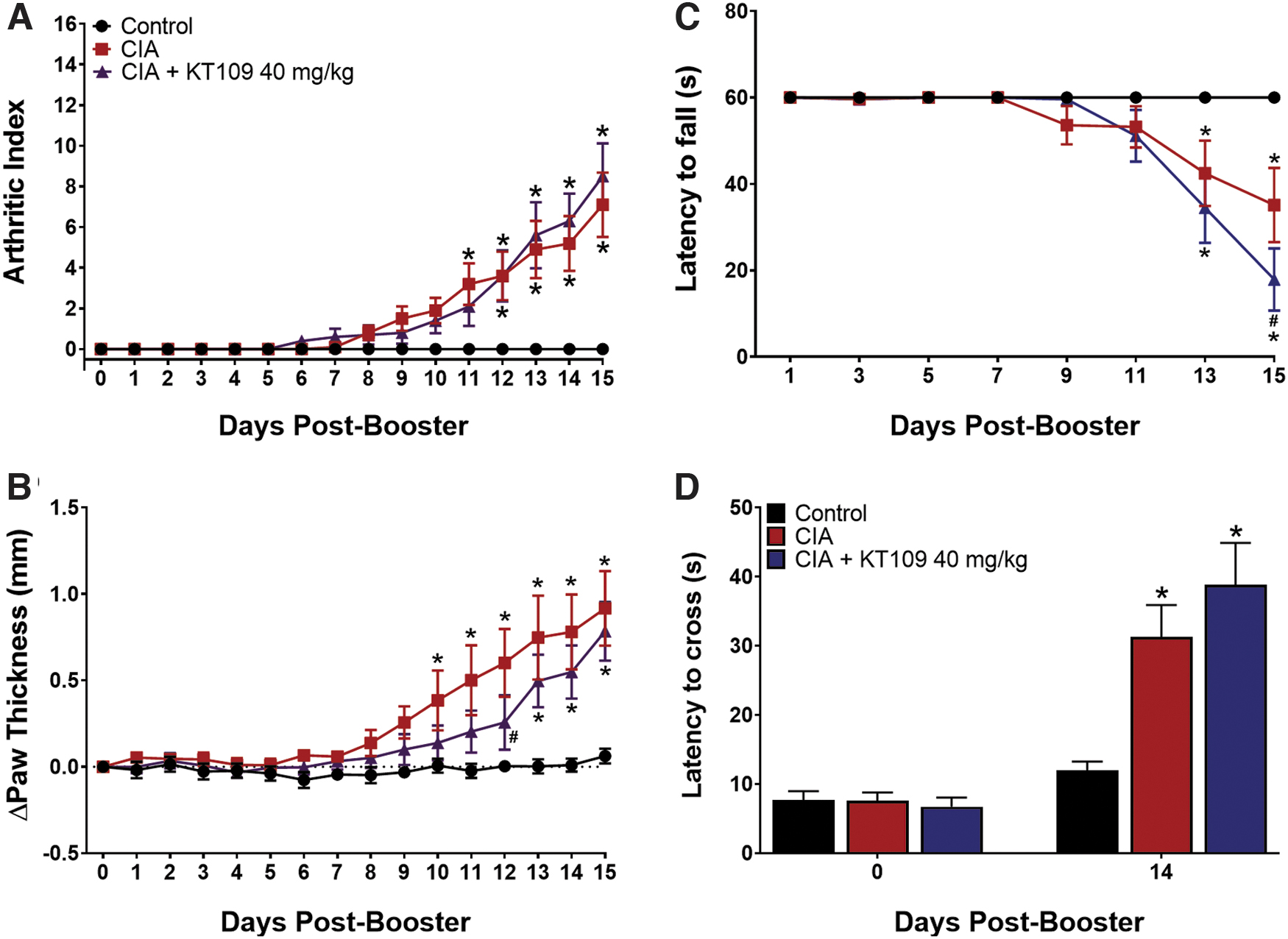
DAGLβ inhibition has no effect on CIA-induced paw swelling and behavioral deficits. Starting at the booster, mice were administered KT109 (40 mg/kg; s.c.) or vehicle for 16 consecutive days. KT109 (40 mg/kg) did not attenuate paw clinical scores
Discussion
The present study demonstrated that MAGL inhibition dose-dependently attenuates signs of CIA. Repeated administration of a high dose of JZL184 (40 mg/kg) suppressed morphological (i.e., clinical scores and paw thickness), as well as functional (i.e., balance beam and grip strength), deficits caused by CIA. The endocannabinoid 2-AG, catabolized by MAGL, is a full agonist at the CB1 and CB2 receptors.54,55 It is worth noting that repeated administration of high doses (e.g., ≥16 mg/kg) of JZL184 reduces CB1 expression and sensitization27,29 and induces tolerance to the analgesic and gastroprotective effects.24,26,29 However, repeated activation of the CB2 receptor does not induce tolerance, receptor desensitization, or CB1 mediated psychotropic effects.19,43,56,57 Furthermore, JZL184 attenuation of acute inflammatory pain and anxiety-like behavior is suppressed by coadministration of synthetic CB2 selective antagonists,24,58 but not the CB1 antagonist rimonabant. Although the present antiarthritic effects of JZL184 appear to be mediated by a CB2 receptor mechanism of action, the repeated high dose of JZL184 administered here also induces dependence and cross-tolerance with CB1 agonists.27,29
In the present study, the CB2 selective antagonist SR144528 attenuated the anti-inflammatory effects and increase in CIA motor function of JZL184, suggesting that the antiarthritic effects of JZL184 occurred through a CB2 receptor mechanism. The selective CB2 agonists HU-308 and JWH133 prevent CIA-induced paw swelling, as quantified by clinical scores, and reduce joint and bone destruction.19,43,44 Furthermore, in the human RA synovium, CB2 is expressed on macrophages, T cells, and B cells, as well as fibroblast-like synoviocytes,16,18–20 and HU-308 and JWH133 attenuate the secretion of IL-6 and IL-8 from stimulated fibroblast-like synoviocytes.18,19 Therefore, we expect that if JZL184 is attenuating paw swelling and motor dysfunction through the CB2 receptor, then JZL184 will also reduce joint destruction and inflammation, but future studies will need to validate this hypothesis. We also cannot rule out the possibility that CB1 plays a role in the attenuation of CIA-induced paw swelling by JZL184. However, the antiarthritic effects of fatty acid amide hydrolase inhibition, and anti-inflammatory effects of MAGL inhibition in models of acute inflammatory pain, are also blocked by the CB2 antagonist SR144528, but not the CB1 antagonist rimonabant,24,42 limiting the likelihood of a strong CB1 receptor contribution in the observed antiarthritic effects of JZL184 in the present study.
Pharmacological combination therapies may (1) increase analgesic and anti-inflammatory efficacy of either drug alone or (2) maintain the efficacy of single administration using lower doses of each drug, thereby decreasing the negative side effects. 59 We confirmed previous data that high doses of DEX attenuate CIA-induced paw inflammation.30,31 However, steroid hormones are not a viable long-term clinical treatment for arthritis, especially at high doses, due to their harmful side effects, such as metabolic problems and mood changes.9,11 Similarly, high doses of repeated JZL184 can lead to tolerance and dependence. Therefore, we extended these findings by demonstrating that subthreshold JZL184+DEX attenuates CIA-induced paw swelling, although the selected dose of DEX alone was more effective than expected, potentially masking any effects of JZL184. Indeed, the approach using subeffective doses to probe additivity is inferior to other approaches, including drug potency shifts or isobolographic analysis of multiple drug ratios. Given the length of each CIA study and variance in severity of CIA across experiments, the feasibility of such designs is limited. Future studies will also incorporate histological measures of joint inflammation and structure, molecular analyses, and imaging assessment of joint destruction.
In the work by another laboratory, mice administered dual DEX/IL-4 treatment had less of a “rebound” effect of exaggerated paw swelling when repeated DEX administration was halted compared to mice in the DEX-only treatment.31,60 Although not assessed here, it is plausible that dual administration with another anti-inflammatory mediator at a subeffective dose may continue anti-inflammatory efficacy even after DEX treatment is terminated.
We also noted inconsistent pain-induced (i.e., increased frequency of incidence after pain manipulation) behaviors 61 across the present studies, in which CIA did not reliably induce allodynia or hyperalgesia. This is possibly due to the robust inflammatory response in the CIA model and explains the paucity of research on behavior using the CIA model of inflammatory arthritis. In other words, CIA resulted in a lack of response to nociceptive paw stimuli that as operationalized would indicate an antinociceptive effect of CIA. However, assays of paw function, such as grip strength, indicated profound functional deficits, suggesting that the lack of response to the von Frey and plantar stimulator test might be due to reduced function of arthritic paws. Therefore, the present study also focused on pain-depressed (i.e., functional impairment) behaviors 61 induced by CIA, as a proxy for functional disability observed in RA patients.5,62
Despite the demonstrated anti-inflammatory and analgesic effects of DAGLβ inhibition, KT109 had no effect on CIA morphological or functional impairments in the current study. Notably, DAGLβ is expressed at higher levels in macrophages than leukocytes40,63 and CIA autoimmunity, like RA autoimmunity, is T cell mediated. 64 The acquired immune response to collagen requires leukocyte activation, 39 and thus, DAGLβ inhibition may exert stronger anti-inflammatory effects in response to challenges to innate immunity, which have a relatively stronger macrophage component. 65 Moreover, as with MAGL inhibition, DAGLβ inhibition reduces pro-inflammatory prostanoid signaling. 40 Regardless, the lack of KT109 efficacy against CIA in the present study further supports the notion that the antiarthritic effects of JZL184 are likely mediated by CB2 activation rather than reductions in arachidonic acid and prostanoid synthesis.
Pain management is multifaceted, often requiring multiple approaches for a patient-focused treatment strategy. The THC/CBD preparation Sativex (i.e., nabiximols) reduces self-reported pain in RA patients. 21 A recent self-report survey for 21 different disease states found that cannabis was used for arthritic pain treatment by 9.3% (n=188) of the patients surveyed 66 with many patients in the study replacing prescription opioid treatment with cannabis. These data, while not as rigorous as a double-blind placebo controlled experiment, are consistent with the notion that the endocannabinoid system may reduce symptoms of inflammatory arthritis in humans and that patients were willing to use cannabinoid treatments, despite potential unwanted CB1-mediated psychoactive side effects. Localized administration of a MAGL inhibitor that does not cross the blood–brain barrier may limit such negative side effects.
The ultimate goal of the present preclinical research is to inform the development of therapeutic treatments for inflammatory arthritis. MAGL inhibition, especially outside the central nervous system, may serve as an adjunctive treatment with current (e.g., steroidal) or future antiarthritic or analgesic pharmacotherapies.
Footnotes
Acknowledgments
The authors thank Kristen Trexler, Matthew Eckard, and Ethan Mick for technical assistance.
Disclosure Statement
The authors declare that no competing financial interests exist.
Funding Information
Grants: Research was supported by the National Institutes of Health (AR066806, DA043571, and GM104942).
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.