
Abstract
Introduction:
Among adolescents and young adults, cannabis use is prevalent. Prior studies characterizing withdrawal effects in this age range have primarily included treatment seeking or comorbid psychiatric samples; these studies have identified several affected domains, especially sleep, mood, and anxiety. The present study compared a community (i.e., nontreatment seeking) sample of cannabis-using and control participants on mood, anxiety, sleep, and withdrawal inventories during the course of a monitored 3-week cannabis abstinence period.
Materials and Methods:
Seventy-nine adolescent and young adult participants (cannabis-using group=37 and control group=42) were recruited from the community to undergo 3 weeks of confirmed abstinence (i.e., urine and sweat patch toxicology) and completion of Cannabis Withdrawal Symptom Criteria, State-Trait Anxiety Inventory, Beck's Depression Inventory, and Pittsburgh Sleep Quality Index across the study period. Repeated measures and cross-sectional regressions were used to examine main effects of group and interactions with time (where appropriate), while accounting for recent alcohol use and cotinine levels.
Results:
Cannabis-using participants reported higher mood (p=0.006), overall withdrawal (p=0.009), and sleep-related withdrawal (p<0.001) symptoms across abstinence compared to controls. Overall withdrawal severity (p=0.04) and sleep-related withdrawal symptoms (p=0.02) demonstrated a quadratic trajectory across the monitored abstinence periods, with an increase from baseline and subsequent decreases in symptom severity. No differences of anxiety scores (p=0.07) or trajectories (p=0.18) were observed. By study completion, groups did not differ among sleep quality components (all p's>.05).
Conclusions:
These findings revealed that nontreatment-seeking cannabis-using adolescents and young adults reported heightened total withdrawal symptoms during a 3-week sustained abstinence period relative to controls. Cannabis-using participants demonstrated an increase in withdrawal symptom trajectory during the first week followed by decreased symptoms from weeks 2 to 3, which contrasts with prior linear decreases observed in cannabis-using adolescent and young adults. More mood symptoms were observed in the cannabis-using group even while excluding for comorbid psychopathologies—along with significantly more sleep problems during the abstinence period. Implications include the necessity to provide psychoeducation for recreational, nontreatment-seeking cannabis-using individuals about cannabis withdrawal, mood symptoms, and sleep quality difficulties when cannabis cessation is attempted, to improve likelihood of long-term sustained abstinence.
Introduction
Within the United States, cannabis is the second most commonly used substance among adolescents and young adults. 1 Approximately 30.6% of adolescents 2 and 52.4% of young adults 3 have used cannabis within their lifetime. Adolescents and young adults are increasingly perceiving cannabis to not be harmful,2,4 which can correspond with an increased likelihood of using. 5 Despite perceptions, regular cannabis use in adolescence is associated with lower educational attainment, other substance use, and increased psychopathology. 6 Yet sustained abstinence (i.e., 3 or more months) has been shown to increase functional outcomes in this age range, 7 but is first associated with a period of cannabis withdrawal that can interfere with maintaining abstinence. 8
Cannabis withdrawal was initially studied in heavy and chronically using adults and several affected domains were identified, including but not limited to, craving, irritability, sleep difficulties, decreased appetite, and restlessness.9,10 These seminal findings led to the categorization of cannabis withdrawal syndrome in the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-5)11–13 ; however, studies have yet to fully characterize if these symptoms differ during sustained abstinence in adolescents and young adults. Furthermore, due to increased potency in cannabis products overtime,14,15 ongoing investigation of cannabis withdrawal and its impact on function is especially important for this age range.
While actively using cannabis, severity or frequency of use is related to increased reporting of depressed mood, anxious feelings, and sleep disturbances.16–19 Among adolescents and young adults, examinations of cannabis withdrawal course have been largely limited to treatment-seeking samples20–25 and samples with psychopathological comorbidities.26,27 These studies have generally found that withdrawal symptoms persisted for at least 2 weeks, 21 are more prolonged for those with psychopathological comorbidities (i.e., 1 week longer compared to those without comorbidities), 27 and are associated with increased affective lability 28 and anxiety. 29 In noncomorbid samples, measures of objective sleep quality in cannabis-using young adults observed declines in sleep duration, efficiency, and amount of rapid eye movement 30 with little change in subjective self-reporting across abstinence, 30 and no association between sleep patterns and use history after 28 days of abstinence among adolescents. 31 Despite these findings, few studies have examined these domains in nontreatment-seeking cannabis-using adolescent and young adult samples without current psychopathological comorbidities.
Thus, the aim of this study is to examine self-report measures of cannabis withdrawal, anxiety, mood, and sleep among nontreatment-seeking cannabis-using adolescents and young adults over 3 weeks of monitored abstinence, relative to controls—a population that is currently understudied yet, given the prevalence of use in this age group, may be more impacted by even cannabis withdrawal syndrome. It is hypothesized that cannabis-using participants will exhibit increased withdrawal severity with a quadratic trajectory across abstinence (i.e., initial increase in symptoms, followed by a reduction in weeks 2–3). In addition, the cannabis-using group will display increased reporting in mood, anxiety, and sleep disturbances at week 1 with significant improvements by week 3.
Methods
Participants
Seventy-nine participants (cannabis-using group=37 and control group=42) were recruited through advertisements in the university and local community. Participants were between the 16 and 26 years of age (M=21.2, SD=2.5) and were gender balanced (45.6% female), and racial identities consisted of predominantly: white (65.8%), Asian American (11.4%), multiracial (10.1%), and black (7.6%) (Table 1).
Demographics and Substance Use Variables
Mean (standard deviation) or %.
p<0.05.
Active tobacco use is defined as level of cotinine ≥3 measured at any week (i.e., 100+ng/mL; www.accutest.net/products/pdf/ds47ny150.pdf).
Notably, this sample consisted of primarily cannabis flower smoking and n=2 reported concentrate usage that was calculated into total past-year grams.
Calculated from date of baseline session and date of last use from TLFB.
Mean is calculated from n=4 controls who used in the past year.
DSM-IV Diagnosis of Cannabis Abuse or Dependence from CDDR.
Mean is calculated from n=12, who met >0.4 ng threshold for reporting quantifiable THCCOOH levels.
Not applicable; n=0 controls met >0.4 ng threshold for reporting quantifiable THCCOOH levels.
Mean is calculated from n=5, who met >0.4 ng threshold for reporting quantifiable THCCOOH levels.
Mean is calculated from n=2, who met >0.4 ng threshold for reporting quantifiable THCCOOH levels.
DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition; TLFB, Timeline Follow-Back.
Participants were included if they spoke English and were willing to abstain from substance use over a 3-week period. Exclusion criteria included an independent Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (Text Revision) (DSM-IV-TR) Axis I (attention, mood, anxiety, or psychotic) disorder, current psychoactive medication use, major medical or neurological disorders, loss of consciousness >2 min, history of learning or intellectual disability, prenatal medical issues or premature birth (gestation <35 weeks), magnetic resonance imaging (MRI) contraindications (pregnancy, claustrophobia, and metal in body), reported significant prenatal alcohol or nicotine exposure or any prenatal drug exposure, or excessive other illicit drug use (>20 times of lifetime use for each drug category). Cannabis-using group used cannabis ≥44 times in the last year (i.e., nearly weekly) and had ≥100 lifetime uses. Control group used cannabis ≤5 times in the past year and ≤20 times in their lifetime.
Procedures
Data for this post-hoc analysis were used from a larger parent study examining the neurocognitive effects of cannabis use in young adults (R01 DA030354; Principal Investigator: Lisdahl); all aspects of the protocol were approved by University of Wisconsin-Milwaukee IRB. Potential participants were asked for demographic information (including age, gender, race, ethnicity, and educational attainment) and screened through an initial semistructured interview for independent lifetime and past-year Axis I Disorders other than substance use disorder over the phone.32,33 If determined eligible, study staff obtained written consent from participants (18 years of age or older). All minors below 18 years of age provided written assent after parent consent was obtained.
Eligible participants attended four study sessions over 3 weeks. The four sessions (herein referred as baseline, week 1, week 2, and week 3) occurred 1 week apart and consisted of urinary drug analysis, drug sweat patch administration, and behavioral measures. During the study period, participants were asked to remain abstinent from alcohol, cannabis, and other substances (other than tobacco), which was confirmed through breath, urine, and sweat toxicology screening. If positive for other drug use, showed an increase in THCCOOH (a metabolite of THC) levels, or had a breath alcohol concentration greater than 0.000 at the start of any subsequent week after baseline, participants were asked to conduct the session after a week of abstinence (n=0 for participants in this study).
Measures
Lifetime substance use
To determine lifetime patterns of drug and alcohol use and determine diagnosis of Cannabis Abuse or Dependence based on DSM-IV-TR, participants were given the Customary Drinking and Drug Use Record (CDDR) 34 at baseline.
Past-year substance use
A modified version of the Timeline Follow-Back (TLFB) interviews was administered at baseline to measure substance use patterns on a weekly basis for the past year.35,36 Substances were measured by standard units (alcohol [standard drinks], nicotine [number of cigarettes; occasions for chew/pipe/cigar/hookah], cannabis [smoked/vaped flower, concentrates, and edibles were measured and dosing was converted to joints based grams], ecstasy [tablets], sedatives [pills], stimulants [mg], hallucinogens [hits], heroin/opium [hits], and inhalants [hits]).
Verifying drug abstinence
As participants were expected to remain abstinent from all alcohol and drugs (other than nicotine) throughout the course of the study, abstinence was evaluated each week with the following: urine samples were tested using the ACCUTEST SplitCup 10 Panel drug test and NicAlert to test cotinine level—a metabolite of nicotine; participants also wore PharmChek Drugs of Abuse Patches, which continuously monitored sweat toxicology and gave quantified values of THCCOOH; and participants underwent breathalyzer screens to test for alcohol use each week.
Cannabis Withdrawal Symptom Criteria
The Cannabis Withdrawal Symptom Criteria (CWSC) was administered across all sessions. The CWSC presents participants with a list of 17 common symptoms associated with cannabis withdrawal to rate based on a 0–10 scale, asking to what extent symptoms were experienced within the past 24 h. Two of these symptoms include “sleep problems” and “strange (unusual) dreams,” which were averaged to assess sleep disturbances across the period of sustained abstinence. 37
State-Trait Anxiety Inventory
The State-Trait Anxiety Inventory (STAI) was administered at baseline and week 3 of the study protocol. The first 20 questions of the STAI ask participants to rate a statement's correspondence with their current internal state on a 4-point Likert scale. 38
Beck's Depression Inventory
The Beck's Depression Inventory-II (BDI) was administered at baseline and week 3 of the study protocol. The BDI provides participants with 21 grouped statements, and respondents pick one statement that describes their mood or feelings during the past 2 weeks. 39
Pittsburgh Sleep Quality Index
The Pittsburgh Sleep Quality Index (PSQI) was administered at week 3. The PSQI presents questions assessing typical sleep qualities and frequencies of sleep disturbances across a number of domains. Seven independent components are calculated and Global PSQI score sums all component scores. 40
Statistical analysis
Analyses were completed in R, version 4.0. 41 Differences in demographic variables were examined using analysis of variance (ANOVA) and Pearson's Chi-square tests. Linear mixed-effects models were run to account for random intercepts of participants across repeated measurements 42 (i.e., STAI, BDI, and CWSC). Single-session measurements (i.e., PSQI) were fitted using generalized linear models. Only complete cases at each session were used due to minimal item-level missingness (2.2%). All analyses controlled for past-year alcohol use and cotinine level at the specified session(s). Main effect of group and interaction (i.e., group*week) effects were ascertained using ANOVA Type-II,43,44 which calculates Wald's Chi-square for effect size.45,46 Due to previous withdrawal characterizations, 47 CWSC analyses were fit with a quadratic parameter of time (i.e., week) and tested against a reduced model with a linear parameter, which resulted in superior fit of the quadratic model (p=0.02); thus, the model with the quadratic time parameter is reported. Decisions about statistical significance were made at p<0.05 for all analyses.
Results
Demographic data
There were no significant differences between cannabis-using and control groups for age (p=0.22), sex (p=0.13), race (p=0.49), ethnicity (p=0.22), and educational attainment (p=0.69). There was a significant difference between groups for past-year alcohol use (p<0.001), past-year nicotine use (p=0.01), cotinine average across weeks (p<0.001), past year (p<0.001), and lifetime (p<0.001) cannabis use (Table 1).
Primary analyses
Withdrawal symptoms
For CWSC total scores, there was a significant effect of group (Wald χ 2 =6.84, p=0.009); on average, cannabis-using group (M=23.20, SD=15.04) reported significantly greater withdrawal symptoms compared to controls (M=16.15, SD=13.52). Furthermore, a quadratic effect of week*group was observed for CWSC scores (Wald χ 2 =4.12, p=0.04); cannabis-using group reported greater withdrawal scores and their trajectory differed from controls in a quadratic trend across the abstinence window, with increases seen at week 1 and subsequent decreases observed for weeks 2 and 3 (Fig. 1; Table 2).
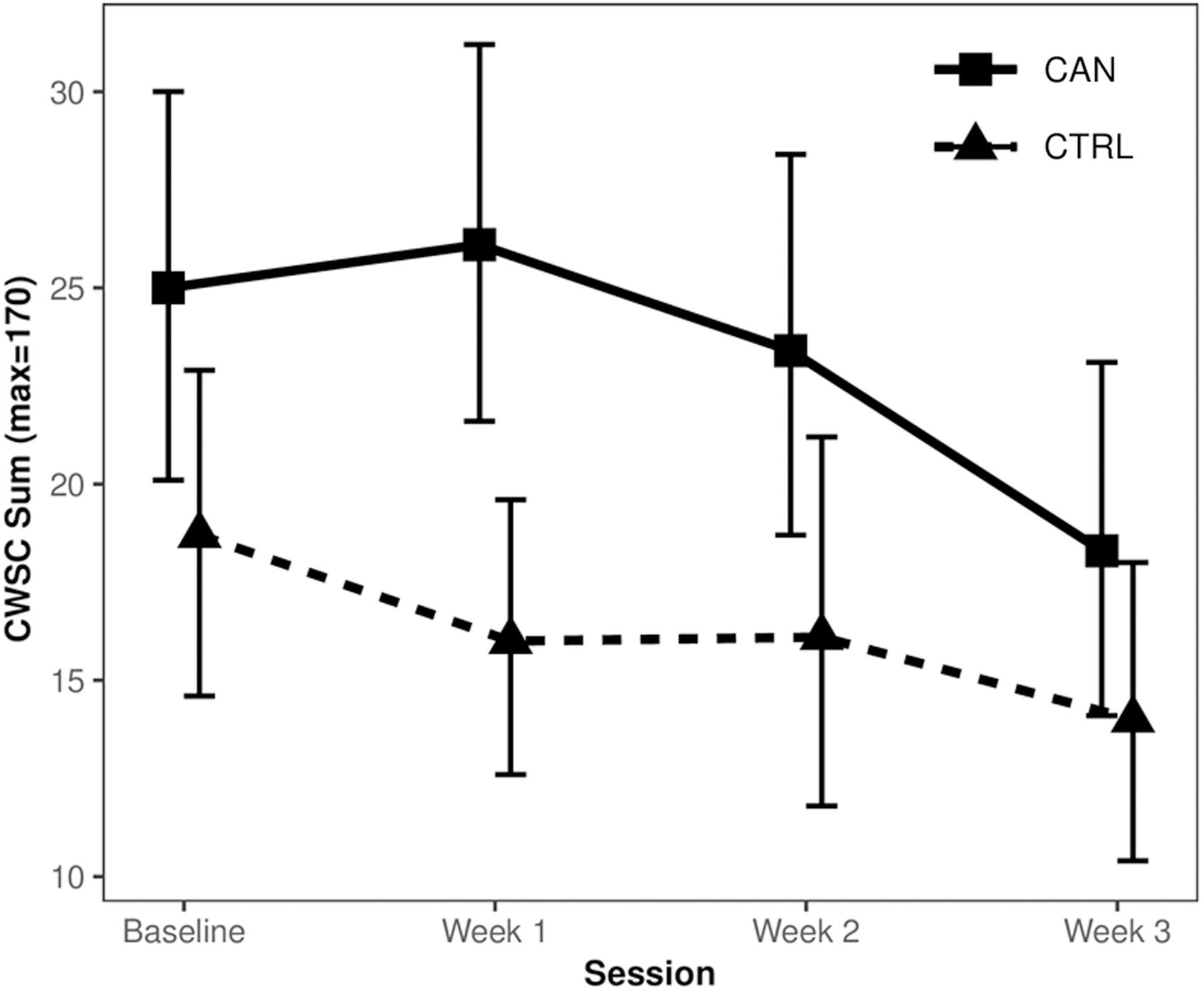
CWSC trajectory across weeks. This figure depicts trajectory of CWSC scores across the abstinence period. Cannabis-using participants (CAN) are depicted with a solid line and nonusing controls (CTRL) with a dashed line. The point represents mean score for the group with 95% confidence intervals as the brackets around the mean. CWSC, Cannabis Withdrawal Symptom Criteria.
Behavioral Index Scores Across Abstinence Period
Mean (standard deviation).
BDI, Beck's Depression Inventory; CWSC, Cannabis Withdrawal Symptom Criteria; STAI, State-Trait Anxiety Inventory; PSQI, Pittsburgh Sleep Quality Index.
Anxiety
On the STAI, there was a marginally significant effect of week—regardless of group—observed (Wald χ 2 =3.29, p=0.07), wherein anxiety reporting decreased at follow-up. Cannabis group (p=0.18) and group*week (p=0.30) effects were nonsignificant (Table 2).
Mood
On the BDI, a significant effect of group was observed (Wald χ 2 =7.56, p=0.006). Cannabis users (M=5.04; SD=4.25) reported greater mood symptoms compared to controls (M=3.04; SD=3.48). A marginal group*week effect was additionally observed (Wald χ 2 =3.67, p=0.055) (Fig. 2; Table 2).

BDI across weeks. This figure depicts trajectory of BDI scores across the abstinence period. Note that BDI was only administered at baseline and session three. Cannabis-using participants (CAN) are depicted with a solid line and nonusing controls (CTRL) with a dashed line. The point represents mean score for the group with 95% confidence intervals as the brackets around the mean. BDI, Beck's Depression Inventory.
Sleep
There was a main effect of group observed on sleep-related CWSC scores (Wald χ 2 =25.89, p<0.001); Cannabis-using group (M=2.17, SD=2.02) reported greater sleep-related withdrawal symptoms across the follow-up period (Control group: M=0.81, SD=1.30). There was a quadratic effect of week*group observed for sleep-related CWSC scores (Wald χ 2 =5.32, p=0.02), wherein cannabis-using participants displayed a quadratic trajectory across the abstinence period compared to controls (Fig. 3).

Sleep-related CWSC across weeks. This figure depicts trajectory of averaged sleep-related CWSC scores across the abstinence period. Cannabis-using participants (CAN) are depicted with a solid line and nonusing controls (CTRL) with a dashed line. The point represents mean score for the group with 95% confidence intervals as the brackets around the mean.
There was no significant effect for any PSQI scores (only available at week 3) (subjective sleep quality: p=0.35; sleep latency: p=0.18; sleep duration: p=0.48; sleep efficiency: p=0.42; sleep disturbance: p=0.14; sleep medication: p=0.65; daytime dysfunction: p=0.15; and Global PSQI Score: p=0.53). Increased sleep duration was linked with decreased cotinine level (Wald χ 2 =5.90, p=0.015; Table 2).
Discussion
In the United States, cannabis is one of the most common recreationally used substances among adolescents and young adults,2,4 with approximately half of adolescents and young adults with cannabis use disorder never fully remitting. 48 Withdrawal syndrome from regular and repeated cannabis use is predictive of sooner relapse 49 and associated with other substance use to mitigate withdrawal 50 ; yet, youth increasingly perceive cannabis use as harmless.2,4 Thus, identifying the impact of withdrawal course in this population provides a novel addition to the literature, informing psychoeducation and clinical recommendations. In this study of nontreatment-seeking and physically healthy adolescents and young adults with no psychiatric comorbidities, regular cannabis-using participants reported significantly elevated withdrawal symptoms and peaking trajectories across 3 weeks of monitored abstinence compared to control participants. Moreover, cannabis-using participants reported more mood symptoms across the study period compared to controls, yet scores do not meet clinical thresholds. Cannabis-using group reported significantly elevated sleep-related withdrawal problems across abstinence, but by week-3 did not differ in overall sleep quality or duration compared to controls. Finally, cannabis-using participants did not differ on anxiety symptoms relative to control participants.
As expected, cannabis-using participants reported more cannabis withdrawal symptoms compared to controls. This corresponds with previous research on cannabis withdrawal reporting in adolescent and young adult treatment-seeking20,51,52 and comorbid 27 samples. Notably, these findings demonstrate heightened withdrawal severity, despite community sample recruitment (i.e., nontreatment seeking). Furthermore, it is well understood treatment-seeking cannabis-using samples experience significant impacts on psychological distress when experiencing withdrawal symptoms, 53 yet, these results suggest nontreatment-seeking samples also undergo a period of withdrawal that may prevent successful abstinence and/or impact daily function, 54 although we are observing a smaller magnitude of differences in this sample relative to heavier cannabis-using samples. Thus, future studies encapsulating both populations are needed as insight into problematic use can moderate the relationship between cannabis withdrawal syndrome and sustained abstinence. 51
More specifically, cannabis-using participants reported significantly elevated withdrawal symptoms from baseline to week 1 follow-up and demonstrated recovery in these symptoms into 2- and 3-week follow-up (Supplementary Fig. S1). In contrast, previous research has reported linear decreases of withdrawal symptoms in cannabis-using adolescents and young adults across assessments of 10 days 24 to 4 weeks21,27—despite robust research showcasing nonlinear trajectories in adults generally over shorter periods of withdrawal.9,16,37,47,54,55 This initial increase in symptom severity followed by decline was observed previously among nontreatment-receiving young adult comparison groups in studies assessing effectiveness of treatments for cannabis withdrawal,25,27 suggesting younger and otherwise healthy cannabis users may demonstrate quick escalation in mild to moderate withdrawal symptoms followed by a relatively quick recovery. However, differences in these findings may be due to varying sample characteristics, including cannabis use severity, concurrent treatment,25,27 and/or utilization of outpatient21,25 and inpatient 24 populations. Furthermore, some participants (21.6%) initiated abstinence before baseline, which limits direct comparisons to studies in more controlled inpatient settings. Future examinations of cannabis withdrawal should assess symptoms more frequently, potentially utilizing ecological momentary assessment56,57 (EMA), throughout a period of monitored abstinence to identify specific and rapid fluctuations in withdrawal severity, as these trajectories—particularly in this age range—are contested. 16
Cannabis-using participants also reported more mood-related symptoms, relative to control participants. This finding aligns with previous research showcasing increased mood reporting among actively cannabis-using adolescents and young adults16,18,20; yet differs from other analyses showcasing decreases in depressive symptomology across abstinence in adolescents and young adults.9,24 However, our participants did not indicate clinically significant mood symptoms, despite observed group differences, which may be due to exclusionary criteria (i.e., DSM-IV Axis I Disorders). Surprisingly, no differences were seen between groups for reported anxiety, which could be due to relatively quick recovery of anxiety and anxiety-related physiological symptoms associated with withdrawal,9,24 potentially attributable to this study procedure or the aforementioned variability in starting abstinence periods before study outset. Moreover, a lack of large effects for mood and anxiety inventories may be a result of recruitment criteria (i.e., nontreatment seeking and Axis-I diagnosis exclusion) as comorbid mood or anxiety disorders are often observed with cannabis use.58,59 Additional large-scale longitudinal studies examining cannabis withdrawal and mood symptoms are needed.
As it pertains to sleep quality and problems, differences were observed in overall reported sleep-related withdrawal symptoms (i.e., sleep problems and strange dreams), in addition to initial increases and subsequent recovery across abstinence. At week 3, groups did not differ in overall sleep quality components, suggesting recovery of acute sleep problems with sustained abstinence. Significant reporting of sleep difficulties across the abstinence period aligns with previous findings demonstrating frequent reporting of sleep-related problems associated with immediate cannabis withdrawal.10,37,60 Trajectories of sleep problems correspond with fluctuations in these symptoms across withdrawal9,56 with eventual decline in subjective reporting, 24 despite persistent sleep architecture aberrations.30,31 Interestingly, cotinine levels were associated with shorter sleep duration, which coincides with pre-existing literature demonstrating sleep quality disturbances associated with tobacco use.61–63 These findings suggest both cannabis and acute nicotine use can disrupt sleep, although cannabis effects recover by the third week of abstinence. This information can be used to provide feedback and psychoeducation to regular cannabis users with intentions to quit.
Subtle deficits from cannabis use can be observed in relation to brain structural,64–68 functional,69,70 and neurocognitive71–75 domains throughout ∼1 month of monitored abstinence. This is important for all health care providers working with emerging adult cannabis users. It is recommended that health care providers (e.g., primary care, mental health counselors, etc.) communicate, even to nontreatment-seeking patients, that mild to moderate cannabis use (i.e., past-year cannabis use for this sample, M=424.7, SD=435.5, Range=44–2306) can be associated with a period of withdrawal, which may affect sustained abstinence. For example, research characterizing the chronic effects of cannabis highlights the importance of considering abstinence when assessing current cognitive function71,75–79 and understanding how prominent withdrawal symptoms can affect cognitive profiles.80–82 Based on these results and prior literature, it is recommended neuropsychologists advise cannabis-using clients partake in at least 2 weeks21,83–85 of abstinence to accurately assess function without the influence of acute or withdrawal symptoms. However, it is notable that subtle mood-related symptoms and sleep withdrawal symptoms may persist past 3 weeks; thus, it is recommended that neuropsychologists assess for sleep and mood symptoms at the time of evaluation. Notwithstanding, exact windows for each outcome in this age range are still under investigation and future studies examining monitored abstinence trajectories should utilize mood/withdrawal inventories, neurocognitive batteries, and MRI at baseline (i.e., closest to the last day of use) with measures repeated appropriately across the abstinence period (e.g., daily mood/withdrawal inventories, weekly neurocognitive assessment, and monthly MRI), and recruitment of both treatment-seeking and nontreatment-seeking populations.
There are a few factors that limit the conclusions of this study. First, direct causality regarding mood and sleep outcomes cannot be determined due to cannabis initiation before study protocols. Prospective longitudinal studies such as the ABCD Study® can investigate early substance patterns and their impact on psychological functioning.86,87 Second, the parent study excluded for independent DSM-IV Axis I disorders and comprised nontreatment-seeking participants, which is noted in contrast to published samples that typically consist of more severe cannabis-using populations experiencing psychological complaint related to their use,20,24,26–28,52 limiting direct comparison, yet provides findings from a more novel sample, which is perhaps more similar to typical young adult users. Based on the parent study protocols, the sample was balanced for aerobic fitness and excluded individuals who could not undergo acute aerobic fitness measurements 72 ; this decreases generalizability to adolescent and young adult populations more broadly, along with sedentary cannabis-using populations. this study aimed to investigate overall differences in withdrawal syndrome; future studies examining individual trajectories and factors that influence severity would be beneficial. Finally, only complete cases for each week were utilized in this analysis, which reduces statistical power, but was low enough to not consider data imputation techniques (2.2% missingness).
Conclusions
This study found that cannabis-using participants reported more mood symptoms and cannabis withdrawal severity across a 3-week period of monitored abstinence. More notably, a nonlinear trend of cannabis withdrawal symptoms was observed with peak severity after 1 week of abstinence and a subsequent decrease in symptoms as abstinence duration increased. Furthermore, although cannabis-using group reported significant sleep-related withdrawal symptoms in the first 3 weeks of cannabis withdrawal, by week 3, they did not significantly differ in their overall sleep quality. These findings represent a novel characterization of affect, overall withdrawal, and sleep-related inventories within a 3-week period of monitored abstinence among nontreatment-seeking cannabis-using adolescents and young adults. Future studies should assess these symptoms through longer, prospective, monitored abstinence windows, while utilizing more frequent assessments (e.g., EMA) coupled with neuropsychological, neuroimaging, mood, and sleep inventories to identify peak severity of symptoms and targets for relapse prevention among cannabis-using populations undergoing withdrawal. These findings have direct implications for assessment and clinical contexts insofar as cannabis-using clients should undergo at least 2 weeks of abstinence—that is, recovery from general withdrawal symptoms—to accurately assess cognitive profiles. In addition, results indicate healthy cannabis-using adolescents and young adults experience fairly quick recovery of withdrawal symptoms after initial abstinence—relative to chronically using adults—which can be interpreted as motivation toward prolonged and maintained abstinence.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the National Institute on Drug Abuse to K.M.L. (R01 DA030354; U01 DAO41025; and R21 DA049109) and the National Institute of Health to N.E.W. (T32 AA013525; P.I.: Riley/Tapert to Wade).
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.