
Abstract
Background:
Severe acute respiratory syndrome coronavirus 2 SARS-CoV-2 has caused >211 million infections and >5.5 million deaths within 24 months globally (WHO). Internationally, a debate emerged about potential benefits of cannabidiol (CBD) as treatment of corona virus disease-19 (COVID-19).
Objective:
To assess the effects of CBD in the treatment of COVID-19–related inflammatory symptoms from the literature.
Methods:
We searched Cochrane COVID-19 study register, CENTRAL (PubMed, Embase, CINAHL, ClinicalTrials.gov, and the WHO's International Clinical Trials Registry Platform), for studies testing CBD as inflammation intervention. All types of studies and populations were considered. All pre-clinical, clinical, and pharmacological outcomes were of interest.
Results:
Of 18 articles found, 9 were included: 5 in vivo animal studies, 3 in vitro human tissue studies and, 1 randomized clinical trial. Outcomes in four in vivo animal studies and three human tissue studies were immune response markers, which decreased. One in vivo study showed enhancement of monocytes. One human study did not show group differences in COVID-19 evolution. There was no information on adverse effects or drug interaction.
Conclusion:
There is not enough evidence to support or refute CBD as a repurpose drug to treat inflammation and other symptoms of COVID-19. Clinical trials are needed to test its efficacy and adverse effects.
Introduction
Corona virus disease-19 (COVID-19) is an emerging rapidly evolving situation. Within 24 months, >326 million confirmed cases of COVID-19, including >5.5 million deaths, have been reported. 1 Main symptoms of COVID-19 are fever and cough, other clinical manifestations are acute respiratory distress syndrome (ARDS), fatigue, muscle soreness, headache, sore throat, or diarrhea. 2 Pathophysiology can be mild to severe, 3 or asymptomatic. 4
In severe cases, COVID-19 may progress to pneumonia, ARDS, and multiorgan dysfunction. 5 Acute lung injury is characterized by the release of proinflammatory cytokine storms. 6 This intense immune response may be caused by excessive production of interleukin (IL)-6 and IL-1b, IL-18, and immune cells. 7 Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-induced inflammation also affects other organ tissues 8 and has an impact on the central nervous system. The case fatality rate is estimated to range from 0.6% to 1%. 9
Owing to the heterogeneity of presentations of the disease and varying vulnerability of the patients, COVID-19 is difficult to treat.10,11 Amid the development of vaccines, anti-inflammatory medications can help reducing severe respiratory symptoms in patients with COVID-19. Approaches to treat COVID-19 include corticosteroids such as dexamethasone (anti-inflammatory, immune suppressive, immune modulatory), remdesivir (antiviral), hydrochloroqine, convalescent plasma therapy, and monoclonal antibodies. 12
Dexamethasone and remdesivir have shown improvements in patient outcomes in hospitalized individuals, 13 but dexamethasone has not been tested in early onset of COVID-19 symptoms, and remdesivir is not suitable for ambulatory use but used in patients hospitalized for SARS-CoV-2 infection and must be applied daily for up to 10 days. 13 Immune modulators can cause severe side effects (e.g., organ damage). Potential investigational therapies (such as viral antibody therapies) are approved by the FDA (FDA news release November 9, 2020) for people diagnosed with COVID-19 and who are at high risk for progressing to severe COVID-19 and/or hospitalization.
Only very few medications, for example, remdesivir, dexamethasone, and viral antibody therapies, have been approved as an experimental drug for severely affected patients. 11 Two recent emergency use authorizations (EUAs), Paxlovid (Pfizer) 14 and molnupiravir (Merck) 15 have been released to treat patients with positive results of SARS-CoV-2 testing who are at risk for progression to severe COVID-19. The duration of treatment is restricted to symptoms onset and no longer than 5 days and only for individuals with no initiation of treatment of severe or critical COVID-19 condition. Currently, there are no suitable approaches available and more effective and safe interventions are needed.
In 2018, cannabidiol (CBD) was approved by the FDA and the EU as orphan medicine for a rare form of severe pediatric and adult epilepsy. 16 Its immunosuppressive and anti-inflammatory properties 17 are now discussed as potentially beneficial in the treatment of COVID-19–related lung inflammation. 18 Since the discovery of the endocannabinoid system as part of the human physiology, delta-9-tetrahydrocannabidiol (THC) and CBD as principal components of the hemp plant Cannabis sativa have been tested for medicinal purposes more systematically. 19 Very recently, a controversial debate about the potential of CBD as a repurposed treatment for COVID-19 has emerged. 20
The pharmacological basis of this hypothesis is that the endocannabinoid system, especially the endocannabinoid receptors 1 (CB1) and 2 (CB2), may be involved in anti-inflammatory processes. CB1 and CB2 receptors are found in the nervous system and other tissues throughout the body. 21 CB2 receptors are expressed in immune tissues such as the gastrointestinal tract, in the lungs, liver, and immune-relevant systems, being distributed throughout the body. 22 Their receptor activation is anti-inflammatory, resulting in decrease of proinflammatory cytokines. 22
CB1 and CB2 receptors, and adenosine A2A receptors are involved in anti-inflammatory effects of CBD in induced lung injury models in murine 17 and could be a target for immune suppression. 23 Other studies suggest cytokines and chemokines as well as effector T cells and microglia cells as critical targets of immune suppression. 24 In several models of inflammatory diseases, CBD was able to block IL-6. 19 A well-accepted entry site for SARS-CoV-2 in the human host, causing COVID-19 symptoms, is the angiotensin-converting enzyme 2 (ACE-2) that is expressed in lung tissue and other mucous membranes of the mouth, nasal, and gastrointestinal tissues. 25
Cannabis-derived derivate CBD is generally considered as safe medication, 26 but low doses of CBD enhance the intoxicating effects of THC, whereas high doses of CBD reduced these effects of THC. 27 Although its counterpart THC has abuse-related effects, CBD was comparable with placebo. 28 Human studies have not shown potential effects of dependence 26 and abuse of CBD. 28
Previous trials on rare forms of epilepsy, 16 drug–drug interaction, 29 and mental disorders 30 suggest that CBD has possible side effects (e.g., pyrexia, somnolence, decreased appetite, sedation, vomiting, ataxia, and abnormal behavior dry mouth, change in appetite and weight, fatigue, diarrhea, and feeling high), depending on its purity or interactions with other substances or medications. Most studies on side effects were conducted pre-clinical in vitro and in vivo and more studies. Researching CBD side effects after real chronic administration on human needs to be conducted. 31
Objective
To critically search the literature for studies that are investigating the beneficial and adverse effects of pure CBD in acute coronavirus disease-related inflammatory and acute respiratory symptoms.
Methods
From September to December 2020, we searched Cochrane COVID-19 study register, Cochrane Central Register of Controlled Trials (CENTRAL), a highly concentrated source of published and unpublished reports of randomized and quasi-randomized controlled trials (including PubMed, Embase, CINAHL, ClinicalTrials.gov and the WHO's International Clinical Trials Registry Platform). We used a combination of terms relating to CBD (e.g., “cannabidiol” OR “cannabidiolic”) and Covid-19 [e.g., (“severe acute respiratory syndrome coronavirus 2” OR “severe acute respiratory syndrome coronavirus 2” OR “ncov”)].
We included all types of studies, in any population and setting, that examined coronavirus disease-related symptoms or outcomes after administration of CBD (any formulation and dose) compared with any other medication (e.g., antipyretics, or untreated control group, independent from publication state. We included studies independently from their publication status. They also had to report on clinical and pre-clinical research and be written in English or German (as these are the languages spoken by the current authors).
All pre-clinical, clinical, and pharmacological outcome measures were of interest, for example, viral load, inflammatory parameters (cytokines), fever, clinical and emotional symptoms (e.g., mood, anxiety, and sleep), severity of COVID-19 and hospitalization, and adverse effects of CBD. Two researchers independently screened the titles and abstracts of all the studies identifies. Any potentially eligible studies were obtained as full articles and screened for inclusion. Data were selected and assessed independently by the two researchers.
Results
The initial search yielded 18 records, of which 9 were included in this review (Fig. 1). Of these, five are in vivo animal studies17,18,33–35 and three are in vitro studies on human tissues.36–38 No COVID-19 animal model was used to study the efficacy of CBD. One human randomized clinical trial (RCT) testing CBD as a treatment for clinical outcomes has been published. 39 Study characteristics of trials are given in Table 1. Excluded studies did not assess inflammation or lung damage as principal outcome (n=4), did not present data (n=4), or were duplicates (n=1).
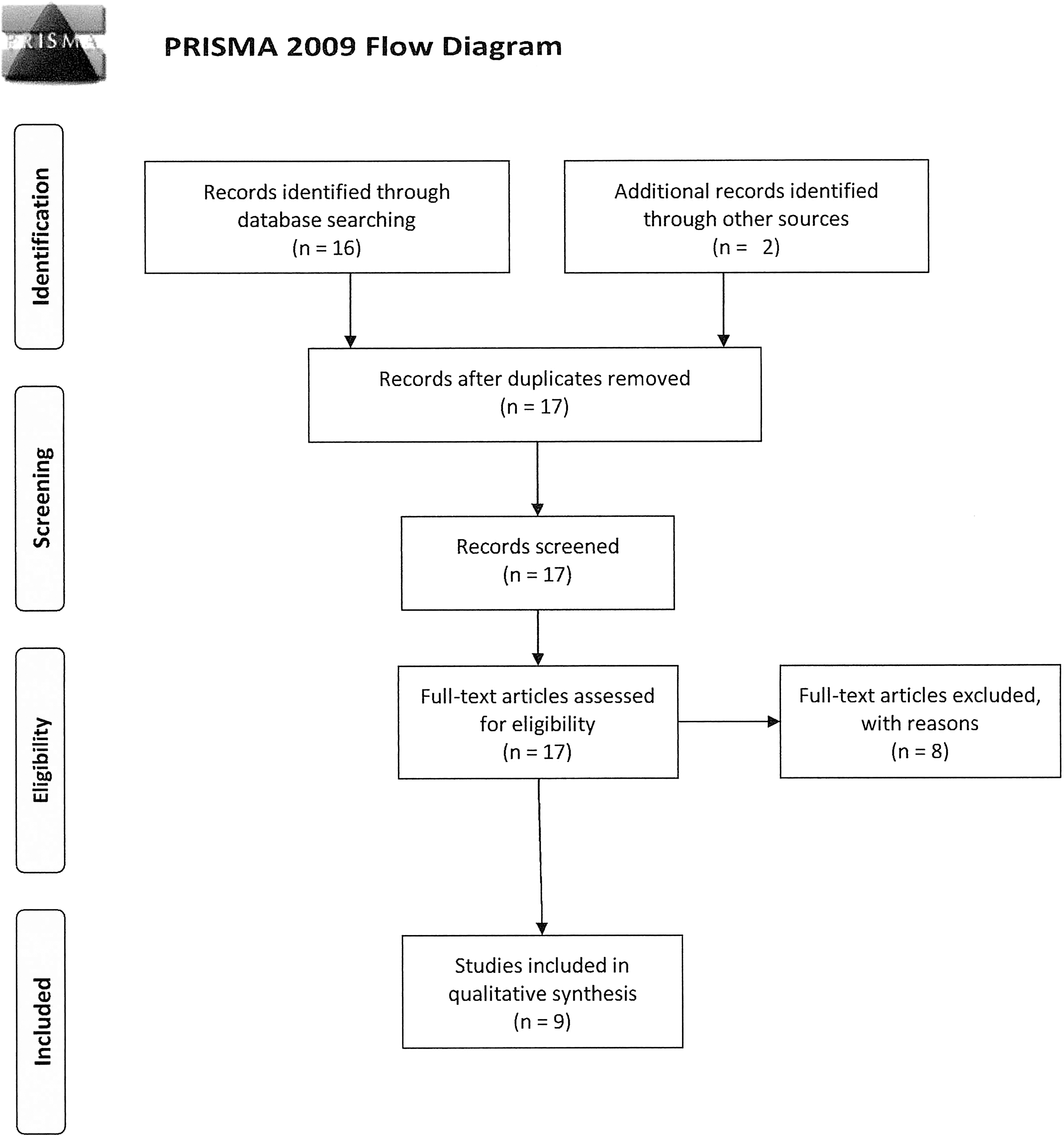
PRISMA 2009 flow diagram. 32
Pre-Clinical and Clinical Trials Using Cannabidiol on Inflammation (N=7)
ACE-2, angiotensin-converting enzyme 2; ARDS, acute respiratory distress syndrome; CBD, cannabidiol; COVID-19, corona virus disease-19; IL, interleukin; LPS, lipopolysaccharide; RCT, randomized clinical trial; RT-PCR, real time polymerase chain reaction; THC, delta-9-tetrahydrocannabidiol.
Studies of inflammatory indications examined a large variety of measures for inflammation and lung disease. Two in vivo studies on animal tissues using a comparison tested the regulation of inflammatory cytokines by CBD versus vehicle and ovalbumin and vehicle 34 and CBD versus sham control 18 with IL-4, IL-5, IL-13, IL-6, IL-10, 34 proinflammatory cytokines, and ARDS 18 as outcomes, resulting in decrease in serum levels of all analyzed cytokines except for IL-10 levels 34 and reduced level of proinflammatory cytokines and ameliorated clinical symptoms of Poly I:C-induced ARDS. 18
Three in vivo studies on animal tissues compared the effect of CBD with a vehicle17,33,35 and tested for leukocyte, albumin and myeloperoxidase concentration in the airways, extracellular adenosine and signaling through A2 receptors, 17 inflammatory cells, 33 and airway resistance and lung elastance, airway collagen fiber content, alveolar septa, and CB1 and CB2 expression. 35 CBD decreased leukocyte migration into the lungs, albumin concentration in the bronchoalveolar lavage fluid, myeloperoxidase activity in the lung tissue, production of proinflammatory cytokines (TNF and IL-6) and chemokines (MCP-1 and MIP-2), and reduced ZM241385 (4-(2-[7-amino-2-(2-furyl)[1,2,4]triazolo[2,3-a][1,3,5]triazin-5-ylamino]ethyl)phenol) due to anti-inflammatory effects of A2A receptors. 17
Although in one study CBD enhanced the presence of monocytes at 6 and 24 h postlipopolysaccharide (LPS)-induced pulmonary inflammation, 32 inflammation was reduced in asthma models accompanied by reduced collagen fiber in airways and alveolar septa, and static lung elastance was reduced with high doses with a significant inverse correlation between CB1 and lung function. 35
Of the four human-related studies included in our review, three were in vitro using tissues of inflammatory colon explant 36 ; airway, oral, and intestine 37 ; and bronchial cells, epithelial cells, macrophages, and fibroblasts. 38 The only human RCT testing pure CBD on patients with mild to moderate SARS-CoV-2 did not show significant differences in the clinical evolution of COVID-19 between groups. 39
Studies on human tissues compared the effects between CBD inflammatory responses of human colon epithelial tissues and Caco-2 cells 36 and CBD with CBD and THC or THC alone on modulation of ACE-2 expression on COVID-19 target tissues 37 and found significant phosphoprotein levels in Caco-2 cultures and colonic explants but not in cultured epithelial cells, 36 and a downregulation of A2A receptors and a decrease of inflammatory in EpiOral, EpiAirway, and EpiIntestinal tissues. 37
Inflammatory responses to CBD treatment in human airway epithelial cells were compared with treatment with dexamethasone 38 and showed that CBD significantly attenuated LPS-induced NF-κB activity and IL-8 and MCP-1 release from macrophages. IL-8, serpin E1, CXCL1, IL-6, MIF, IFN-γ, MCP-1, RANTES, and TNF-α were induced, whereas MCP-1/CCL2, CCL5, eotaxin, IL-1ra, and IL-2 were reduced.
In Brasil, an RCT in humans with mild-to-moderate SARS-CoV-2 infection compared a daily dose of 300 mg CBD (two 150 mg doses; 1 mL of the formulation) with placebo (1 mL medium/coconut chain triglyceride oil — MCT) for 14 days. 39 The outcomes in this study include prevention of severe/critical stages of COVID-19, time to COVID-19 symptoms relief, number of participants with negative clinical COVID-19 symptoms, change in proinflammatory cytokine concentration, parenchymal lung damage induced by COVID-19, adverse events, hospitalization, 28-day mortality, positive-to-negative saliva 2019-n-CoV real time polymerase chain reaction conversion, reduction in viral load, generalized anxiety disorder, depression, odor, and other variables (Table 1).
The study showed no significant difference between study group and placebo group in baseline disease severity and median time to symptom resolution. The study found mostly mild side effects such as somnolence, fatigue, changes in appetite, lethargy, nausea, diarrhea, and fever with no significant difference between treatment groups.
Safety/tolerability/doses
Currently, the appropriate dose of CBD for treatments of inflammation is unspecified since CBD is highly dose dependent.
One randomized open label clinical trial 40 showed reduced symptoms of burnout and emotional exhaustion in COVID-19 frontline workers. Five of 59 participants of the treatment group experienced serious adverse events (4 with elevated liver enzymes and 1 with pharmacodermia). All have fully recovered.
Discussion
Although vaccinations for COVID-19 are available now, it will need years to vaccinate most of the world populations. To treat infected persons, effective and safe drugs are highly needed to avoid severe illness and long-term complications. This review aimed to identify pre-clinical and clinical studies on CBD as a treatment for organ inflammatory symptoms. A recent RCT 39 has tested CBD with a specified dose as a treatment for COVID-19 symptoms. The development of clinical symptoms was not significantly different between groups that could be attributed to a uniform dose of 300 mg/day or that the patients had low inflammation levels.
Only mild side effects were reported, showing that CBD is a relatively mild treatment for COVID-19. Limitations of the study are that it did not include several different doses and the treatment period of this RCT lasted 14 days. A single CT lung scan was performed after 14 days. Since CBD is dose dependent, a study should include different doses to investigate therapeutic effects on COVID-19–related inflammation. Pre- and post-therapy CTs should be considered.
Pre-clinical studies using CBD have shown promising results on inflammatory outcomes of the lungs, of the gastrointestinal tract, and of the cornea. In human model rodents, airway anti-inflammatory effects were achieved by regulation of ACE-2, 37 hyper-responsiveness of the respiratory tract, 35 and expression of IL-6 was reduced 18 by CBD. Inflammatory processes in extracts of human gastrointestinal tissue 36 and corneal tissue of inflammation in rodents were reduced by CBD. A recent study using a human lung epithelia model, which was discovered after our systematic literature search showed a dose-dependent and purity-dependent activity on chemokine and cytokine reduction as well as ACE-2 reduction. 41
Owing to differential results depending on purity or fraction of extracts used in vitro showing proinflammatory or anti-inflammatory effects, the authors recommend to users and health care providers to avoid the use of cannabinoids to treat COVID-19.
Another recent study 42 published after our systematic literature search using CBD in mice and cells suggested that CBD inhibits SARS-CoV-2 replication in part by upregulating stress response in the endoplasmic reticulum in lung and nasal tissues in a dose-dependent manner during early stages of infection. The study also utilized matched human groups data from the National COVID Cohort Collaborative in which 100 mg/mL oral CBD solution had a significant negative association with positive SARS-CoV-2 test results.
Side effects (e.g., pyrexia, somnolence, decreased appetite, sedation, vomiting, ataxia, and dry mouth) in humans were shown only in severe pediatric epilepsy so far. Side effects of CBD as a medication to treat inflammatory diseases in humans have not been examined and need to be assessed in clinical trials. Information of CBD combined with other drugs is missing, too. It is not clear whether these findings can be translated to CBD if used to treat patients with mild COVID-19–related respiratory symptoms. There are no data on an appropriate dose because CBD is dose dependent. The published RCT could not show additional beneficial effect as an add-on to standard care.
Furthermore, a possible drug–drug interaction was brought to attention in the literature, 43 which needs to be examined for corticosteroids (e.g., dexamethasone), antiviral drugs (e.g., remdesivir), hydrochloroqine, convalescent plasma therapy, or monoclonal antibodies. 12 Its anti-inflammatory properties could also be detrimental in suppressing the immune response, which might suppress the ability to fight off infections so that the risk might be higher for viral and respiratory infections. 20 An important message to the clinicians is that that there is insufficient evidence to support or refute the use of CBD in the treatment for COVID-19 symptoms.
Conclusion
CBD has shown some promising anti-inflammatory effects in a few pre-clinical studies, but not in the few human studies. Evidence on beneficial or harmful effects of CBD in the treatment of COVID-19 is missing and should be further investigated.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.