
Abstract
Introduction:
Recent longitudinal studies point toward the existence of a positive relationship between cannabis use and violence in people with severe mental disorders (SMD). However, the existence of a dose–response relationship between the frequency/severity of cannabis use and violence has seldom been investigated. Therefore, this study aims to determine if such a relationship exists in a psychiatric population.
Methods:
To do so, a total of 98 outpatients (81 males and 17 females, all over 18 years of age) with SMD were recruited at the Institut universitaire de santé mentale de Montréal (Montréal, Canada) and included in the analyses. Clinical evaluations were conducted every 3 months for a year. Substance use, violent behaviors, and potential covariables were assessed through self-reported assessments, urinary testing, as well as clinical, criminal, and police records. Using generalized estimating equations, the association between cannabis use frequency (nonusers, occasional, regular, and frequent users) and violence was investigated, as well as the association between the severity of cannabis use and violent behaviors.
Results:
It was found that cannabis use frequency and severity were significant predictors of violent behaviors. After adjustment for time, age, sex, ethnicity, diagnoses, impulsivity, and use of alcohol and stimulants, odds ratios were of 1.91 (p<0.001) between each frequency profile and 1.040 (p<0.001) for each increase of one point of the severity of cannabis use score (ranging from 0 to 79).
Conclusions:
Despite the high attrition rate, these findings may have important implications for clinicians as cannabis use may have serious consequences in psychiatric populations. Nevertheless, the mechanisms underlying this association remain unclear.
Introduction
Individuals with severe mental disorders (SMD), such as schizophrenia, are more likely to be victims than perpetrators of violence. 1 Nevertheless, there is an increased modest risk of violence committed by those with SMD.2–4 The consequences of such acts may be serious for the perpetrator, the victims, their families, and the wider community. 4 It is even more important to recognize the factors responsible for violence for preventative strategies and thus decrease associated stigma. 5 Amid risk factors, literature has documented the overall association between substance misuse and violence, and numerous studies have accordingly reported that substance misuse has a major role in the occurrence of violence among patients with SMD.6–9 Although the association between alcohol use and violence in addition to overall substance use has been far more studied, much less work has been conducted in the association with cannabis alone.
Notably, rates of cannabis use disorders (CUDs) are higher among patients with SMD compared to the general population.10–12 Despite a drop in the perceived harm of cannabis use, as well as its increased acceptability in the last decades, several undesirable health sequelae, including exacerbated psychiatric symptoms (i.e., psychotic symptoms), worse prognosis, increased hospitalization, higher risk of suicidal behaviors, and decreased quality of life, have been linked to cannabis use, mainly its heavy and persistent use.13–32 Notwithstanding advances in knowledge on the association between cannabis use and violence in the general population, limited consideration has been dedicated to those with SMD.33–42 Unlike studies of other substances, the cannabis–violence relationship remains a topic of debate.
Although studies remain heterogeneous (i.e. Norström and Rossow 43 ), there is meta-analytical evidence pointing toward a moderate association between cannabis use and violence in different samples and a potential dose–response relationship with larger effects being observed in more frequent users. 44 Concerning the meta-analysis on SMD samples comprising 12 studies, results showed a moderate association between cannabis use and violence (odds ratio [OR]=3.02, confidence interval [CI]=2.01–4.54). 45 When considering studies having adjusted for confounding factors, the effect was slightly smaller, but significant.
The association was significantly superior for cannabis misuse compared to cannabis use. However, the meta-analysis was characterized by high heterogeneity, which may have been partly due to the studies displaying a variety of definitions for violence and assessment methods, or likewise due to the various geographical contexts, as well as differences in cannabis legalization policies. 46 Moreover, most of the available studies in SMD samples show many methodological limitations that should not be neglected when attempting to examine the cannabis–violence association (e.g., limited data on cannabis exposure patterns, limited control for important confounders such as alcohol and stimulant use, and impulsivity) as they may have under or overestimated the amplitude of the relationship. In addition, most studies have been cross-sectional and retrospective in nature, thereby evidence was limited to infer causality and for concluding on the direction of the association. Likewise, studies have not evaluated a potential dose–response relationship with differing profiles of cannabis users. Therefore, fewer longitudinal studies have been conducted to establish the directionality of the association, as well as the association with different exposure patterns in patients with SMD.
A few longitudinal studies in the general population have indeed been conducted to clarify the directionality of the association (e.g., Norström and Rossow, 43 Pedersen and Skardhamar, 47 Reingle et al, 48 Brook et al, 49 Schoeler et al, 50 Monshouwer et al, 51 Ostrowsky, 52 White et al, 53 Duarte et al, 54 Derzon and Lipsey, 55 Lim and Lui 56 ), with some suggesting a unidirectional association and others a reverse association or even a bidirectional association. Nevertheless, more recent literature has suggested a stronger relationship when examining the effects of persistent cannabis use (as opposed to occasional use) on subsequent violence.48,50,56 Growing literature in SMD samples have likewise reported similar findings.40,42 Longitudinal data from well-known databases have shown that persistent cannabis use predicted subsequent violent behavior, while the reverse relationship was not significant.40,42 Importantly, findings from these studies remained significant after controlling for important confounding factors, including alcohol and stimulant use.
Considering international cannabis policy changes and limited literature on the cannabis–violence association in SMD samples, further longitudinal studies examining such relationship are critically needed. The present study aims to investigate the cannabis–violence relationship in a sample of psychiatric patients, by investigating more particularly profiles of severity and frequency of cannabis use in relation to acts of violence. We hypothesized that a dose–response association between cannabis and violence will be found. Moreover, we believed that continued frequent cannabis use will be a significant predictor for violence perpetration even after controlling for confounding factors.
Methods
Study sample and design
Participants were psychiatric patients at the Institut universitaire en santé mentale de Montréal (Quebec, Canada). Between June 2018 and January 2020, 103 participants were recruited through various sources: 39 were referred from a partnership help with Signature Bank, 57 which recruited consecutive people showing up in the emergency room, 51 were referred by their treating clinical teams, 12 were solicited following their participation to another research project, and 1 was self-referred (by word of mouth). Inclusion criteria were the following: being 18 years of age or older, having a DSM-5 diagnosis of SMD, having used cannabis at least once in their lifetime, and finally living in the community setting or being soon-to-be discharged from the hospital (the baseline visit was scheduled at maximum 2 weeks before the discharge date as estimated by their treating clinical teams). For follow-up reasons, participants without a fixed address were excluded.
The following diagnoses were defined as SMD: schizophrenia, schizoaffective disorder, nonspecified or substance-induced psychosis, delusional disorder, bipolar disorder (type 1, type 2, substance induced, or unspecified), and major depressive disorder. As violent acts were expected to be relatively rare, only past or current cannabis users (as opposed to cannabis naive individuals) were included to increase statistical power.
This longitudinal observational study began in June 2018 and was prematurely stopped due to the coronavirus disease 2019 (COVID-19) pandemic in March 2020. Following the baseline evaluation, participants were interviewed every 3 months for a total of 4 follow-up visits over a year.
After a complete description of study, all participants provided their written informed consent. The study was approved by the Ehics Committee of the CIUSSS de l'Est-de-l'Île-de-Montréal.
Assessments
Various measures were collected using tools and questionnaires that were administered either by a research nurse or by a trained evaluator. Medical, police, and criminal records were used to complement the obtained information when possible. All interviews were conducted in French. When no French version of a questionnaire was available, it was translated and then back-translated by two members of our team.
Primary diagnoses
Primary diagnoses were established by consulting participants' medical records, and these were confirmed by a research nurse using the Structured Clinical Interview for DSM-5 (SCID-5), a widely used clinical tool based on the DSM-5 with excellent sensitivity and specificity. 58 If the diagnosis was not consistent with the medical records, the case was then discussed with a psychiatrist (A.D.) to reach a final primary diagnosis.
Substance use
Cannabis use and dependence were assessed during each interview visit using the Cannabis Use Problems Identification Test (CUPIT). This tool is a brief questionnaire that was found to be valid and acceptable across diverse community settings. Moreover, it has excellent reliability (test-retest ranging between 0.89 and 0.99) and internal consistency (Cronbach's alphas ranging from 0.79 to 0.92). 59 The severity of cannabis use was measured using the standardized total score.
Moreover, the severity of CUD was also measured using the SCID-5; however, it was only performed during the baseline interview, which often had to be split in half due to its long duration. To increase participant retention, follow-up interviews were kept as short as possible. Of note, the CUPIT score strongly correlates with the number of DSM symptoms, and its cutoff scores are highly sensitive and specific. 59 All participants who did not use cannabis in the preceding time period (12 months for baseline and 3 months for each follow-up visit) were rated as zero. With that score, the following categories could be determined: 0–8=no cannabis use problems; 9–16=at risk of dependency; 17–79=CUD. 59
The frequency of cannabis use was assessed using the second and third items of the CUPIT: “On how many days have you used cannabis over the past 3 months (90 days)?” and “How many times would you use cannabis on a typical day when you were using?” Participants were categorized into four groups based on frequency of cannabis use: nonusers, occasional users (less than once a week), regular users (once a week to once a day), and frequent users (more than once a day). These profiles are in accordance with the ones that were used in the Quebec Cannabis Survey. 60
Patients were also asked about their use of other drugs and alcohol during the past week using the Timeline Follow-back (TLFB) questionnaire, a standardized tool with an excellent reliability (intraclass correlation coefficient ranging from 0.70 to 0.94) and validity (high correlations with urine assay). 61 Since alcohol and stimulant (cocaine, amphetamine, 3,4-methylenedioxy-methamphetamine use are known to be associated with cannabis use and violence and that the use of other drugs (i.e., opiates, benzodiazepines, hallucinogens) was rare and negligible, only alcohol and stimulants were included as covariate in statistical analyses.
At each visit, patients underwent a urinary test (QuickCheck Drug Screen Test Cup with Creatinine 62 ), which tested for the presence of tetrahydrocannabinol (THC), cocaine, opioids, amphetamines, and methamphetamines. When patients reported not having used any drugs, the absence of such drug use was also confirmed through urinary testing. In contrast, a negative test on a participant that reported using drugs was not considered in the analyses due to the presence of false negatives. 62 If the patient tested positive to stimulants even though they said they did not consume any, they were classified as users. However, since we were interested in the severity of cannabis use, cannabis users that were not consistent regarding their status were excluded from the project and from the analyses.
Violence
Violent behaviors were primarily self-reported during each visit using the MacArthur Abbreviated Community Violence Instrument (MACVI), a tool with excellent reliability and validity which was initially developed for the MacArthur Violence Risk Assessment Study. 63 This questionnaire assessed aggressive behaviors within the last 12 months preceding the completion of the baseline visit and within 3 months preceding each of the follow-up visits. Such behaviors included violence toward others (e.g., hitting, slapping, or pushing someone) and threats of serious violence (e.g., with a lethal weapon). For the last item of the MACVI, “Have you done anything else that might be considered violent?,” as well as for each act obtained through criminal, medical, or police records, the Cormier-Lang Criminal History Score definition of violent behavior (i.e. Quinsey et al 64 ) was used to characterize violent acts. For example, an assault and a treat with weapons were considered as violent acts, whereas mischief to public property was not.
Data on violent acts were collected during the preceding year and following the recruitment period for all 103 participants through their criminal, police (Index general module d'information policière database), and medical records, when available.
Impulsivity
Impulsivity, which is an important covariate when studying violence, was measured during the baseline interview using the French short version of the Impulsive Behavior Scale (UPPS-P). This scale has shown good internal consistency and test-retest stability (i.e. Billieux et al 65 ), even within individuals with a substance use disorder (i.e., Cronbach's alphas=0.63 to 0.85 66 ).
Statistical analyses
The effects of the severity of cannabis use (standardized CUPIT total score) on violence (dichotomic) were examined using generalized estimating equations (GEE) with a binary logistic model and an exchangeable working correlation matrix. Since the collected data were time dynamic, the models were adjusted for timepoints. The same was also done for the effects of the frequency of cannabis use (1=nonusers; 2=occasional users; 3=regular users; 4=frequent users) on violence (dichotomic). Multivariate analyses were then performed using the same approach, adjusting for potential covariates: time, age, sex, ethnicity, impulsivity, alcohol use, stimulant use, and primary diagnosis. In addition, to evaluate the presence or absence of attrition bias, associations between the number of completed visits and potential predictors (violence, substance use, etc.) were calculated using Pearson's correlations.
All statistical analyses were performed using SPSS for Windows version 25. The threshold for statistical significance was set at p-value <0.05.
Results
Sample characteristics
From the 103 recruited participants, 56 were reassessed after 3 months, 52 after 6 months, 40 after 9 months, and 28 were interviewed at the 12-month follow-up visit. However, seven participants (7%) were excluded from the study during their follow-up for various reasons, notably inconsistency in their answers or the impossibility to extract information from them (e.g., the presence of severe negative symptoms). The evaluations that were completed before the exclusion were nevertheless included in the analysis. Due to these exclusions and some missing data, analyses could only be performed on 98 participants, totalizing 267 visits, for an average of 3 visits per participant. From this sample, only 21 participants (21%) completed all 5 interviews. However, it is worth acknowledging that the follow-up of 33 participants (34%) was interrupted in March 2020 due to the COVID-19 pandemic. Details about the course of the study are presented in Figure 1.
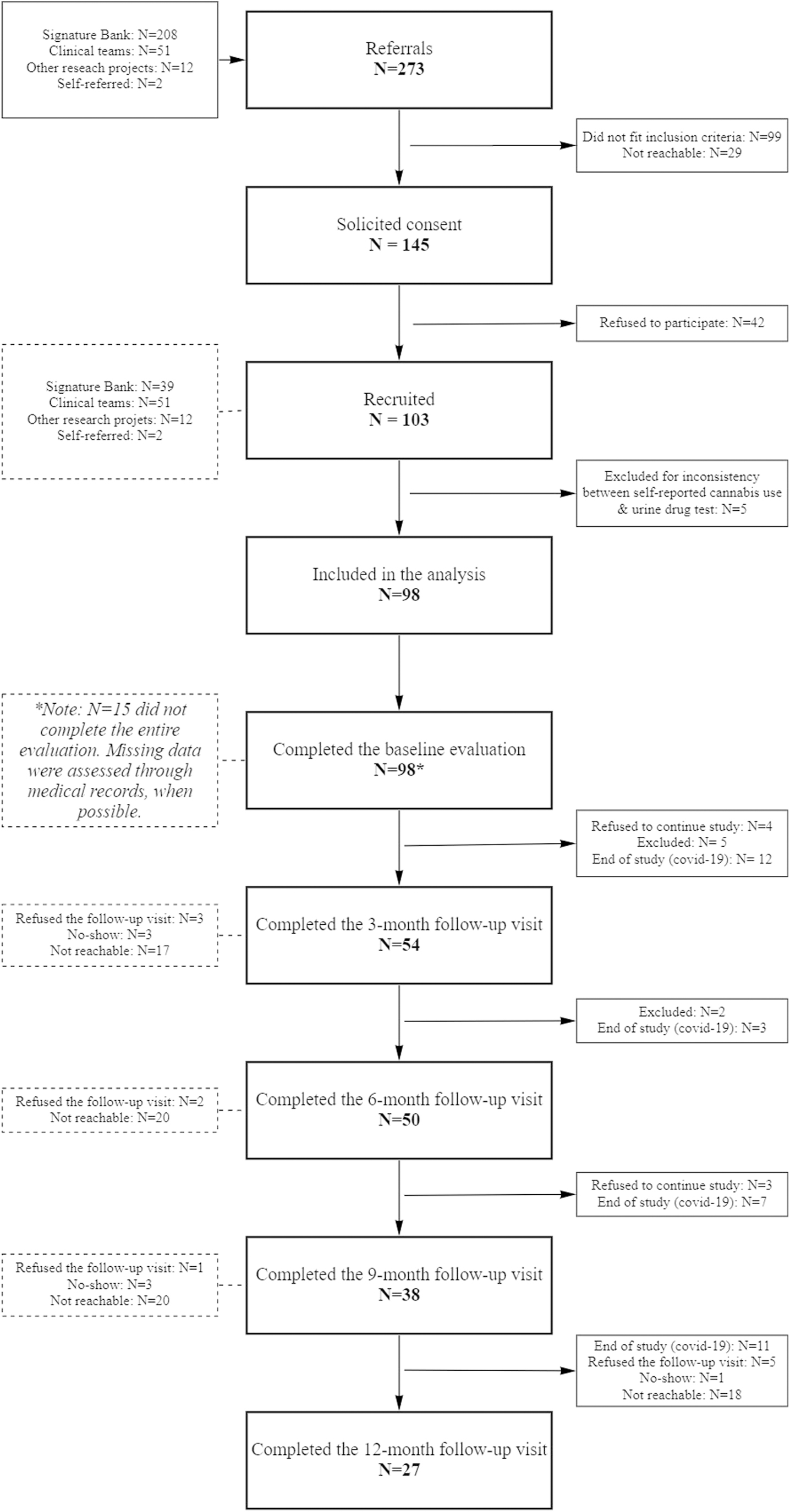
Study profile of participants who underwent a 1-year follow-up. From 273 referrals, the consent of 145 was solicited and 103 of them were finally recruited.
The mean age was of 39.5 years (standard deviation=12.9; range=19–69). The majority were unmarried Caucasian men with a diagnosis of a psychotic disorder. Over a quarter of the sample (28%) also had a comorbid personality disorder. Detailed sample characteristics are presented in Table 1.
Detailed Sample Characteristics N=98
SD, standard deviation; UPPS-P, French short version of the Impulsive Behavior Scale.
Drug and alcohol use decreased drastically after the baseline visit and then remained relatively stable. A similar pattern was observed for violent behavior. However, it should be noted that the baseline visit covered the whole year before the evaluation, whereas each follow-up visit covered solely a 3-month time lapse. On one hand, Pearson's correlations showed negative associations between the number of completed visits and baseline violence (R=−0.357, p<0.001), borderline personality disorder (R=−0.226, p=0.035), and the period of follow-up evaluation being conducted during the COVID-19 pandemic (R=−0.359, p<0.001). On the other hand, losses to follow-up were not significantly correlated with drug and alcohol use at baseline.
Frequency of cannabis use as a predictor of violence
As shown in Table 2a, unadjusted GEE results revealed that consuming cannabis more frequently increased the likelihood of committing acts of violence (OR=1.35; 95% CI=1.06–1.72; p=0.014). The same analysis was also conducted with adjustment for potential covariates: timepoint, sex, age, ethnicity, diagnoses, impulsivity, alcohol use, and stimulant use (Table 2b). In doing so, the association between the frequency of cannabis use and violence remained significant (OR=1.91; 95% CI=1.33–2.74; p<0.001). These results are illustrated in Figure 2.

Estimated means with standard errors for violence associated with frequency of cannabis use across each timepoint. N=87. For each increase of one profile: OR=1.91; 95% CI=1.33–2.74; p<0.001. Nonusers=No cannabis use, Occasional users=less than once a week, Regular users=once a week to once a day, Frequent users=more than once a day. Results are adjusted for the effects of the timepoint, sex, age, ethnicity (Caucasian vs. others), primary diagnosis (schizophrenia spectrum disorders and affective disorders; presence/absence), personality disorders (presence/absence), impulsivity (UPPS), alcohol use (presence/absence), and stimulant use (presence/absence). 95% CI, 95% confidence interval; OR, odds ratio.
Unadjusted (a) and Adjusted (b) Generalized Estimating Equations with a Binary Logistic Model and an Exchangeable Working Correlation Matrix Estimating the Effects of the Frequency of Cannabis Use on Violence Occurring at the Same Timepoint
Ordinal variable: 1=No cannabis use (nonusers); 2=Less than once a week (occasional users); 3=Once a week to once a day (regular users); 4=More than once a day (frequent users).
Adjusted for the effects of the timepoint.
Adjusted for the effects of the timepoint, sex, age, ethnicity (Caucasian vs. others), primary diagnosis (schizophrenia spectrum disorders and affective disorders; presence/absence), personality disorders (presence/absence), impulsivity (UPPS), alcohol use (presence/absence), and stimulant use (presence/absence).
95% CI, 95% confidence interval; GEE, generalized estimating equations; OR, odds ratio; UPPS-P, French short version of the Impulsive Behavior Scale.
Severity of cannabis use as a predictor of violence
The impact of cannabis use on participants was quantified using the standardized CUPIT score. Unadjusted GEE has shown a strong association between cannabis use severity and violence with each unit increase resulting in 1.040 times more risk of being violent (95% CI=1.022–1.058; p<0.001). After adjustments for potential covariates, this association remained stable (OR=1.040; 95% CI=1.016–1.064; p<0.001). As shown in Figure 3, the dose–response relationship between cannabis use severity and violence was mostly observed for those with a CUD, that is, with an adjusted CUPIT score of over 17.

Estimated means with standard error for violence associated with the severity of cannabis use across each timepoint. N=88. For each increase of one unit: OR=1.040, 95% CI=1.016–1.064, p<0.001. The CUPIT total score was adjusted (score – 3) to bring the minimum score to 0. The nonusers were rated 0. Two cutoff points are illustrated: 9=at risk of CUD, 17=diagnosis of CUD. Results are adjusted for the effects of the timepoint, sex, age, ethnicity (Caucasians vs. others), primary diagnosis (schizophrenia spectrum disorders and affective disorders; presence/absence), personality disorders (presence/absence), impulsivity (UPPS), alcohol use (presence/absence), and stimulant use (presence/absence). CUD, cannabis use disorder.
Discussion
This study aimed to investigate the relationship between cannabis use and violent behaviors in people with SMD. More precisely, the possibility of a dose–response relationship between frequency, as well as severity of cannabis use, and violence was explored. Using GEE, significant dose–response associations were observed. These associations remained stable after adjustment for potential covariates.
First, it was found that more frequent cannabis use was associated with a higher risk of violent behaviors. Indeed, being a frequent cannabis user was associated with a risk of committing violent acts 2.5 times higher than individuals in the nonusers group. This result is consistent with previous literature showing the existence of an association between persistent cannabis use and violence in people with SMD.40,42 Indeed, in a sample of individuals with SMD, it was observed that the cumulative use of cannabis was associated with a higher risk of violence. 40 These results were subsequently replicated in another large sample of patients with schizophrenia. 42 The current study further investigated the causality of this association by exploring the existence of a dose–response relationship. Results showed that the association remained stable after controlling for confounding factors (time, gender, age, ethnicity, primary diagnosis, impulsivity, alcohol use, and stimulant use).
Therefore, this association was not mediated by the concomitant use of other substances. Second, a robust association was observed between the severity of cannabis use (standardized CUPIT score) and violent behaviors. Even after adjustments for potential covariates, the association remained strongly significant. Therefore, these results suggest that the more problematic cannabis use was (i.e., cannabis use interfering with ability to perform usual activities, feeling that consumption is needed or that it is difficult to go through the day without it, and so on), the more likely participants were to commit acts of hetero-aggression. This result follows existing literature suggesting that cannabis abuse and associated consequences are more strongly associated with violence than nonproblematic cannabis use in a SMD sample. 45
However, because the number of violent behaviors at follow-up was insufficient to evaluate the impact of cannabis use on future violence, it remains unclear whether the observed relationship is bidirectional or not. Previous studies have shown unidirectional relationships between cannabis use and subsequent violence in adults with SMD. Although a tendency could generally be observed in prior studies on similar samples of adults with SMD, the reverse relationship was not significant, possibly due to a lack of statistical power.40,41 It remains to be noted, however, that there is evidence of a higher risk of cannabis use in youth with externalizing behaviors, such as impulsivity, which may be associated with violent behaviors later on in life as well.67,68 Future longitudinal studies are needed to clarify the direction of the association throughout individuals' lifetime.
Several hypotheses can be put forward to explain the association between cannabis use and violence. First, cannabis might lead to violent acts through the exacerbation of psychotic symptoms. Notably, a dose–response relationship between cannabis use and the risk of developing psychosis was repeatedly observed, and it subsequently seems to be associated with exacerbated symptoms as well after the first episode of psychosis. 69 It is indeed commonly noted that patients with exacerbated psychotic symptoms may present with aggressive or violent behaviors. Moreover, a recent study using the medical records from 1089 individuals under Section 136 of the UK Mental Health Act showed that the use of cannabinoids seemed to increase the risk of violence associated with psychotic symptoms (i.e. Kalk et al 70 ), which is in line with the hypothesis.
Another mechanism stated in literature is that cannabis use could be associated with a sudden increase in impulsivity, which could subsequently lead to violence. However, in the present study, the impulsivity score did not seem to have a role on the cannabis–violence relationship, although impulsivity was only measured at baseline as such a trait generally remains stable over time. 71 Nevertheless, transient increases in impulsivity could have occurred while intoxicated and these cannot be detected with periodic evaluations. 72
The association between cannabis use and violence could also be explained by social and cultural factors that are commonly associated with both drug use and violence, such as coming from a high-criminality environment or having a history of abuse.73,74 In such a case, the relationship would likely be bidirectional.
Finally, cannabis withdrawal could also be in play, especially since it was shown to be linked with anxiety, irritability, and violence.75,76 It is possible that part of our sample sporadically experiences cannabis withdrawal periods, for example, due to financial reasons or difficulties of access. Moreover, frequent cannabis use was previously shown to be associated with an increased likelihood of withdrawal symptoms. 77 Although several distinct mechanisms have been suggested in literature, it is possible and even likely that several of these elements are combined.
Limitations
This innovative study investigated a possible dose–response relationship between cannabis use frequency/severity and violent behaviors in patients with SMD. Although these results represent a significant contribution to the field and address many previously named limitations, notably by following participants prospectively and using objective measures, a few limitations must be acknowledged.
First, the low prevalence of violence at follow-ups; it was not possible to consider the interaction between time and substance consumption, thereby accessing the direction of the association. A solution to address this problem in future studies could be to recruit individuals at higher risk of violence, for example, people who committed such acts in the past.
Second, most measurements were self-reported, thereby introducing potential recall and social desirability biases. However, several steps were undertaken to minimize these biases, especially for the primary outcomes. For drug use, urinary testing was included. Violent behaviors were also assessed through medical, police, and criminal records.
Third, the attrition rate was high, and the study was ceased prematurely due to the COVID-19 pandemic. Consequently, only a minority of participants completed all follow-up evaluations, and results should therefore be interpreted with caution. Factors that could be associated with attrition (i.e., introducing an attrition bias) were measured, and it has been determined that violence was associated with attrition, while cannabis use was not. However, there is no reason to believe that this could explain the presented results; on the contrary, the fact that individuals pursuing violence were less likely to be followed could have reduced the statistical power of our analyses, and therefore, the strength of the associations might have been underestimated.
Finally, cannabis use frequency was assessed regardless of the amount of the type of cannabis consumed. Unfortunately, this information is generally unavailable when patients recreationally consume street drugs. Nevertheless, the amount of THC and cannabidiol (CBD) might greatly influence the effects of cannabis. Notably, the use of CBD might be beneficial for individuals with mental illnesses, notably in reducing anxiety symptoms78,79 or treating individuals with a dual diagnosis of psychotic and THC-related CUD. 80 In Quebec, illegal cannabis contains around 20.5% THC and 1.7% CBD, whereas legal cannabis is composed from a mean of 15.5% THC and 2.0% CBD. 81 In the era in which cannabis is now legal, the exact properties of the cannabis consumed should be assessed more easily in future studies, which will clarify the role of each component in these associations.
Conclusion
In conclusion, a relationship was observed between cannabis use and violence in individuals with SMD. The severity of cannabis use was strongly associated with violent behaviors as well, suggesting that the problematic aspects of cannabis consumption (e.g., being dependent) could be the factors that mediate the relationship between frequency of use and violence. Although a growing body of evidence points toward the existence of that relationship, more studies will now be needed to elucidate why and how cannabis consumption could lead individuals with SMD to aggression. If replicated, these findings could be highly relevant for clinical practice as cannabis might not be as inoffensive as it might appear, and therefore, CUDs should be tackled seriously and treated appropriately. In light of these observations, the authors recommend that violence should be considered when documenting the impacts of cannabis legalization policies.
Footnotes
Acknowledgment
Authors would like to thank the participants and students that contributed to the projects, as well as the evaluators and research nurses who completed the clinical evaluations.
Authors' Contributions
The study was designed by A.D., S.P., C.E.G., and M.B. Statistical analyses were performed by M.B., C.E.G., and S.G. The article was written by M.B., L.D., S.G., and A.D. All the authors have made substantial contributions and have revised, edited, and approved the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research project was funded by the Fondation Jean-Louis Lévesque, which is a non-profit organization supporting academic research in many innovative areas.