
Abstract
Background:
Cannabis consumption for recreational and medical use is increasing worldwide. However, the long-term effects on kidney health and disease are largely unknown.
Materials and Methods:
Post hoc analysis of cannabis use as a risk factor for kidney disease was performed using data from the Assessment, Serial Evaluation, and Subsequent Sequelae of Acute Kidney Injury (ASSESS-AKI) study that enrolled hospitalized adults with and without acute kidney injury from four U.S. centers during 2009–2015. Associations between self-reported cannabis consumption and the categorical and continuous outcomes were determined using multivariable Cox regression and linear mixed models, respectively.
Results:
Over a mean follow-up of 4.5±1.8 years, 94 participants without chronic kidney disease (CKD) (estimated glomerular filtration rate [eGFR] >60 mL/min/1.73 m2) who consumed cannabis had similar rates of annual eGFR decline versus 889 nonconsumers (mean difference=−0.02 mL/min/1.73 m2/year, p=0.9) and incident CKD (≥25% reduction in eGFR compared with the 3-month post-hospitalization measured eGFR and achieving CKD stage 3 or higher) (adjusted hazard ratio [aHR]=1.2; 95% confidence interval [CI]=0.7–2.0). Nineteen participants with CKD (eGFR <60 mL/min/1.73 m2) who consumed cannabis had more rapid eGFR decline versus 597 nonconsumers (mean difference=−1.3 mL/min/1.73 m2/year; p=0.02) that was not independently associated with an increased risk of CKD progression (≥50% reduction in eGFR compared with the 3-month post-hospitalization eGFR, reaching CKD stage 5, or receiving kidney replacement therapy) (aHR=1.6; 95% CI=0.7–3.5). Cannabis consumption was not associated with the rate of change in urine albumin to creatinine ratio (UACR) over time among those with (p=0.7) or without CKD (p=0.4).
Conclusions:
Cannabis consumption did not adversely affect the kidney function of participants without CKD but was associated with a faster annual eGFR decline among participants with CKD. Cannabis consumption was not associated with changes in UACR over time, incident CKD, or progressive CKD regardless of baseline kidney function. Additional research is needed to investigate the kidney endocannabinoid system and the impact of cannabis use on kidney disease outcomes.
Introduction
Cannabis consumption has increased considerably over the past decade in the United States and worldwide, particularly among people older than 50 years,1–3 an age group enriched with chronic illness including chronic kidney disease (CKD). 4 In fact, adults with chronic medical conditions are more likely to consume cannabis than healthy individuals. 5 However, the long-term health effects of cannabis on some of these conditions are currently unknown.
Nevertheless, the perceived risk associated with cannabis consumption among older adults with chronic medical conditions has decreased the greatest among those living with CKD. 6 Nephrologists broadly support the study and consumption of cannabinoids for symptoms associated with CKD and end-stage kidney disease (ESKD),7,8 while people living with these conditions also express interest and some people do in fact consume it. 9 With increasing availability and consumption of cannabis, there is growing importance to understand the clinical impact on people living with CKD and ESKD and those at risk of developing CKD.10,11
Cannabis naturally contains many phytocannabinoids, including the most abundant and well-described Δ 9 -tetrahydrocannabinol and cannabidiol. Cannabinoids have differing activities and affinities for the ubiquitously expressed G-protein coupled cannabinoid receptors type 1 (CB1R) and type 2 (CB2R). In the rodent kidney, these receptors influence kidney blood flow, glomerular filtration rate (GFR), fibrosis, proteinuria, and various tubular functions.12–16 In pre-clinical animal models, activation of CB1R worsens kidney disease17–19 while conflicting data suggest that activation of CB2R could be harmful20,21 or protective.22–25 Additionally, some cannabinoid isolates are protective in rodent models of acute kidney injury (AKI).23,26–28 Whether these effects apply to human cannabis consumption remains to be determined.
Knowledge regarding cannabis consumption on native kidney outcomes is limited to a few studies that evaluated generally healthy people29,30 or people living with CKD.31,32 We hypothesized that cannabis consumption may adversely impact the kidney function of people living with kidney disease. Therefore, we sought to evaluate the association between chronic cannabis consumption and long-term kidney outcomes of individuals with kidney disease or those who were at high-risk for kidney disease.
Materials and Methods
Study design and population
Post hoc analysis of cannabis use as a risk factor for kidney disease was performed using data from the Assessment, Serial Evaluation, and Subsequent Sequelae of Acute Kidney Injury (ASSESS-AKI) study, which was a parallel matched cohort study that enrolled individually matched hospitalized adults with and without AKI, many of whom had pre-existing CKD,33–35 designed to characterize the short-term and long-term natural history of AKI including important renal and cardiovascular outcomes. Participants were enrolled from four clinical centers (Kaiser Permanente Northern California, Vanderbilt University, University of Washington, and Yale University/Western University) between December 2009 and February 2015.
The institutional review boards of the participating institutions approved the study, and informed consent was obtained from all participants enrolled in ASSESS-AKI. A total of 1,599 study participants had an outpatient research study visit 3 months after index hospitalization discharge, during which clinical data and biosamples were systematically collected. This visit was considered the baseline study visit, and the follow-up in-person study visits were conducted annually thereafter. Medical history, study events, and use of medications were updated at each in-person visit and estimated glomerular filtration rate (eGFR) requantified.
Exposure measures
Participant lifestyle characteristics were collected from questionnaires administered at the 3-month post-hospitalization and subsequent annual study visits. Past year cannabis consumption was determined at each study visit by self-report and defined as responding “yes” to, “Since your last study visit, have you used marijuana?” Cannabis nonconsumers were defined as always responding “no” at every post-hospitalization study visit. Chronic cannabis consumption was defined as responding “yes” to the follow-up question, “Have you used marijuana within the past 30 days?” at every post-hospitalization study visit. Participants with any cannabis consumption and chronic cannabis consumption were combined to define the exposure. Tobacco, alcohol, and other drug consumption were determined by self-report at the 3-month post-hospitalization visit regarding the type, quantity, and frequency of usage.
Outcome measures
All participants had serum creatinine (SCr) concentration measured, and eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration equation 36 at the 3-month post-hospitalization study visit and subsequent annual visits. Random urine albumin to creatinine ratio (UACR) was quantified concurrently. Serum and urine creatinine concentration was measured using the Roche enzymatic method (Roche Diagnostics) on a Roche ModP Chemistry Analyzer before January 2014 and Cobas 6000 Chemistry Analyzer afterward. The method was calibrated, and checked semiannually, using the National Institute of Standards and Technology standard traceable to reference material SRM 909b (Isotope Dilution Mass Spectroscopy).
Urine albumin concentration was quantified using a nephelometric method on the Siemens ProSpec Analyzer (Siemens GmbH). Kidney function decline was defined by the parent study protocol, where incident CKD among participants without pre-existing CKD (eGFR ≥60 mL/min/1.73 m2) before the index hospitalization was defined as a≥25% reduction in eGFR compared with the 3-month post-hospitalization measured eGFR and achieving CKD stage 3 or higher. Progression of CKD among participants with pre-existing CKD at the index hospitalization (preadmission eGFR <60 mL/min/1.73 m2) was defined as a≥50% reduction in eGFR compared with the 3-month post-hospitalization eGFR, reaching CKD stage 5, or receiving kidney replacement therapy (long-term dialysis or kidney transplant). 35
Covariates
Demographic characteristics included age, sex, self-reported race/ethnicity, employment status, education level, and annual income. Self-reported prior cardiovascular disease (heart failure, myocardial infarction, stroke, or peripheral artery disease) was recorded. Hypertension was based on self-report combined with taking antihypertensive agents, or having a study visit systolic blood pressure (SBP) >140 mm Hg and/or a diastolic blood pressure (DBP) >90 mm Hg. Diabetes (types 1 and 2) was based on self-report, taking prescription antidiabetic agents, or having a glycosylated hemoglobin level of ≥6.5%. Sepsis was based on suspected infection plus the presence of at least two criteria of systemic inflammatory response syndrome. Shock was defined by physician diagnosis. There were no missing data in any of the primary exposures of interest, other key covariates, or outcomes examined.
Statistical analyses
Multivariable Cox regression models were used to assess the association between cannabis consumption and time until incident and progressive CKD after adjustment for covariates including: AKI status at the index hospitalization, sex, Black race, Hispanic ethnicity, former smoker, current smoker, diabetes, sepsis, body mass index (BMI), parathyroid hormone, phosphorus, and C-reactive protein. Linear mixed models were used to assess the independent association of cannabis consumption with change in eGFR and UACR over time after adjusting for the within-subject variance of the participant intercept as a random effect.
Key covariates were used as additional fixed effects in the regression models, which included: AKI status at the index hospitalization, demographic characteristics (age, sex, race), lifestyle characteristics (tobacco use, alcohol use, other illicit drug use); comorbid conditions (diabetes mellitus, hypertension, cardiovascular disease, cancer, chronic obstructive pulmonary disease); SBP, DBP, BMI, laboratory variables (LDL and HDL cholesterol), and medications (renin–angiotensin–aldosterone system [RAAS] antagonists, diuretics). For all analyses, a two-tailed t-test value of p<0.05 was taken as evidence of statistical significance. All statistical analyses were performed with SAS Version 9.4.
Results
Participant baseline characteristics
Of 1,599 study participants, 1,486 did not consume cannabis (93%), whereas 113 consumed cannabis within the past year (8%), of whom 96 consumed cannabis chronically (85% of all cannabis consumers), having consumed cannabis within the 30 days preceding every post-hospitalization study visit (Table 1). At baseline, cannabis consumers had a mean age of 54±12 years while nonconsumers had a mean age of 65±12 years, were 78% White and 18% Black compared with nonconsumers who were 82% White and 12% Black, were 78% male while nonconsumers were 61% male, and were enrolled from the University of Washington site (60%) while nonconsumers were more evenly distributed across the four study centers.
Baseline Characteristics of Cannabis Consumers and Nonconsumers
Demographics were determined from the index hospitalization. Data are presented either as total number and percentage or mean ± SD.
SD, standard deviation.
From the 1,599 total study participants, 616 had CKD, of whom 19 (3%) consumed cannabis and 597 (97%) did not (Table 2). Of the remaining 983 participants who did not have CKD, 94 (10%) of them consumed cannabis while 889 (90%) did not. Baseline comorbidities were similar among the groups except for chronic liver disease being more prevalent among participants without CKD who consumed cannabis compared with nonconsumer counterparts (11% vs. 3%).
Baseline Characteristics of Cannabis Consumers and Nonconsumers Stratified by Chronic Kidney Disease Status
Demographics and comorbidities were determined from the index hospitalization, whereas lifestyle habits, vitals, and laboratory variables were determined from the 3 month post-hospitalization study visit. Data are presented either as total number and percentage or as mean±SD.
BMI, body mass index; CKD, chronic kidney disease; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; SBP, systolic blood pressure; SCr, serum creatinine; UACR, urine albumin to creatinine ratio.
Participants with CKD who consumed cannabis were younger than nonconsumers with CKD (mean 57.7±6.7 vs. 70.2±10.3 years), had a higher baseline SCr (1.9±0.8 vs. 1.5±0.7 mg/dL), UACR (130.0±77.1 vs. 91.8±65.3 mg/g), DBP (81.7±12.1 vs. 68.4±13.9 mm Hg), and BMI (36.0±9.9 vs. 31.1±7.4 kg/m2) but had a similar eGFR (45.2±20.3 vs. 47.9±16.3 mL/min/1.73 m2) and SBP (135.3±22.7 vs. 128.0±21.1 mm Hg; Table 2). Additionally, of the 19 participants with CKD who consumed cannabis, 10 (53%) were permanently disabled, 9 (47%) had an annual income less than $20,000, and 8 (42%) did not receive education past high school (Table 3).
Baseline Socioeconomic Characteristics of Cannabis Consumers and Nonconsumers Determined from the Index Hospitalization and Stratified by Baseline Chronic Kidney Disease Status
Data are presented as total number and percentage.
Participants without CKD who consumed cannabis were younger than nonconsumers (mean 53.7±13.5 vs. 61.8±13.0 years) and had a higher eGFR (95.1±22.1 vs. 82.9±20.4 mL/min/1.73 m2) but had a similar baseline SCr (0.9±0.4 vs. 0.9±0.4 mg/dL), UACR (114.0±81.6 vs. 103.2±75.4 mg/g), SBP (124.3±18.5 vs. 126.8±20.5 mm Hg), DBP (74.1±12.5 vs. 73.0±13.5 mm Hg), and BMI (29.5±7.7 vs. 30.9±7.8 kg/m2; Table 2).
Regular heavy tobacco smoking was reported most frequently from participants without CKD who consumed cannabis compared with cannabis nonconsumers without CKD (29% vs. 9%). Rates of tobacco smoking among participants with CKD were similar between cannabis consumers and nonconsumers (11% vs. 6%; Table 2). Additionally, participants without CKD who consumed cannabis reported frequent heavy alcohol drinking more commonly compared with cannabis nonconsumers (32% vs. 21%), whereas participants with CKD had similar rates of alcohol drinking regardless of cannabis consumption (16% vs. 17%). Finally, of the 113 total cannabis consumers, 6 also used methamphetamine, cocaine, heroin, or other drugs, none of whom had CKD.
Kidney outcomes by cannabis consumption
Over a mean follow-up of 4.5±1.8 years, participants with CKD who consumed cannabis had a faster rate of annual eGFR decline compared with nonconsumers (−2.69±0.98 vs. −1.41±0.21 mL/min/1.73 m2/year; p=0.02; Fig. 1), whereas participants without CKD demonstrated similar rates of annual eGFR decline between cannabis consumers and nonconsumers (−1.64±0.52 vs. −1.61±0.15 mL/min/1.73 m2/year; p=0.92). Cannabis consumption was not associated with differences in annual change in UACR compared with nonconsumers regardless of whether participants had CKD (0.14±0.22 vs. 0.17±0.04 mg/g/year; p=0.75) or not (0.16±0.11 vs. 0.11±0.03 mg/g/year; p=0.40).
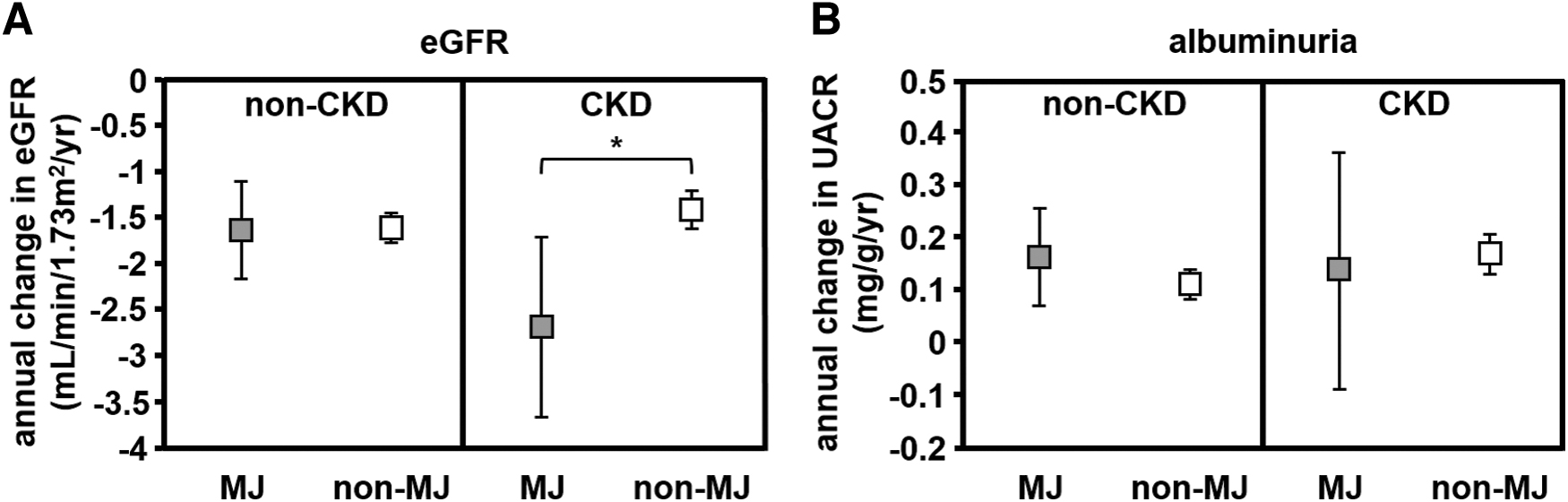
Change in
Cannabis consumption among participants without CKD was not associated with the development of CKD (incidence rate of 19/82 [23.2%] consumers vs. 185/898 [20.6%] nonconsumers; adjusted hazard ratio [aHR]=1.22; 95% confidence interval [CI]=0.74–2.01; p=0.43), nor was there an independent association with increased risk of CKD progression among those already with CKD (incidence rate of 7/31 [22.6%] consumers vs. 90/588 nonconsumers [15.3%]; adjusted HR=1.59; 95% CI=0.71–3.54; p=0.26; Figs. 2 and 3).

Adjusted HR for incident or progressive CKD in cannabis consumers vs. nonconsumers. Cannabis consumption among participants without CKD was not associated with the development of CKD (p=0.43), nor was there an independent association with increased risk of CKD progression among participants with CKD (p=0.26). aHR, adjusted hazard ratio.
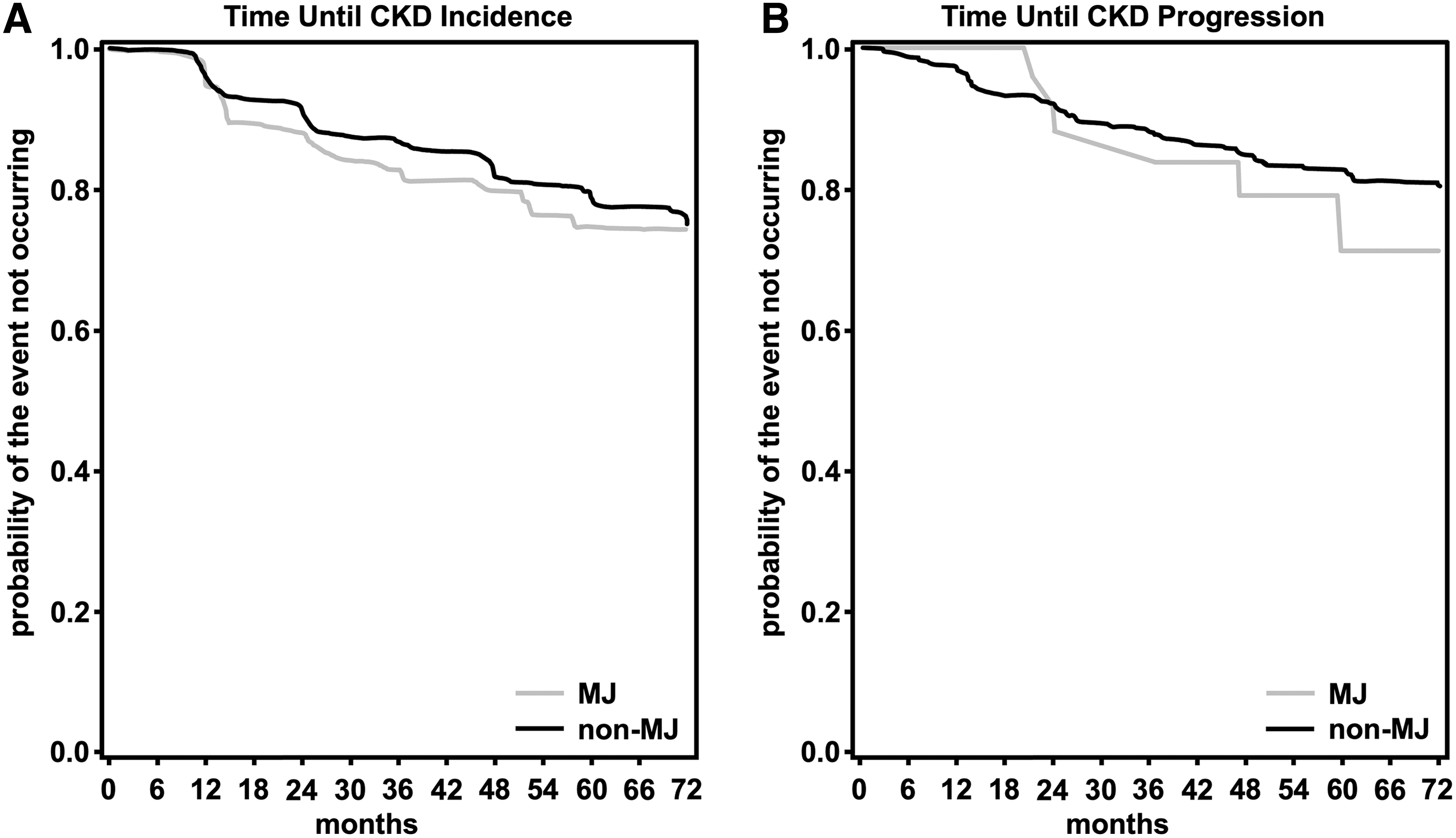
Kaplan–Meier estimates of time to CKD
Discussion
Retrospective analysis of the multicenter ASSESS-AKI study revealed that self-reported cannabis consumption did not adversely affect the kidney function of participants without CKD, but that cannabis consumption was associated with a faster annual eGFR decline among participants with CKD. Additionally, cannabis consumption was not associated with changes in UACR over time, incident CKD, or progression of CKD regardless of baseline kidney function.
Findings from this study add to a growing body of evidence that cannabis consumption among an older population with normal kidney function does not seem to adversely affect kidney function. Our results from participants without CKD regarding eGFR and albuminuria are consistent with previously reported retrospective analyses of the Coronary Artery Risk Development in Young Adults (CARDIA) study, 29 which did not demonstrate a longitudinal association between cannabis consumption and eGFR change, rapid eGFR decline, or prevalent albuminuria, and the nationally representative National Health and Nutrition Examination Survey (NHANES), 30 which did not find a clinically significant effect of self-reported past or current cannabis consumption on SCr, eGFR, UACR, or odds of having stage 2 or higher CKD.
Both of these respective cohorts were larger (3,765 and 13,995 participants), had longer follow-up (15 and 7 years), and their participants were younger (mean 35 years, but mean age was not reported in the NHANES study, although 86% of the cohort was <50 years), and had higher baseline eGFR than our study (111 and 99 mL/min/1.73 m2).
A recent retrospective analysis examined the association between chronic heavy cannabis consumption on baseline kidney function at inpatient admission for 42 treatment-seeking cannabis-dependent adults. 37 Participants did not have any other concomitant substance abuse or dependence, were primarily White Europeans who were younger (mean age=29 years), and had higher baseline eGFR (104 mL/min) than participants from our cohort. Despite near-daily cannabis consumption for a mean of 55±60 months and notably, one participant for 360 months, no participant had significant kidney dysfunction. Five participants had stage 2 CKD, but those individuals smoked on average more cigarettes per day and two of these participants had a comorbid medical condition. 37
Although the number of participants in our study with CKD who consumed cannabis was low, the faster annual eGFR decline that we observed differs from prior research. Retrospective analysis of the Chronic Renal Insufficiency Cohort (CRIC) study did not reveal an association between cannabis consumption and CKD progression defined as incident ESKD or halving of eGFR. 31 Participants were similar in age and had a similar baseline eGFR to our study, but their cohort was larger (3,939 participants) with slightly longer follow-up (5.5 years). However, the 1,293 cannabis consumers included those with any lifetime or past year consumption limiting the ability to make conclusions about current consumption.
Recently, a retrospective analysis of U.S. veterans with advanced CKD who were transitioning to dialysis found that 66 participants with cannabis-only positive urine toxicology screens and 168 participants with positivity for cannabis and other drugs had similar rates of AKI within the week after the positive urine test compared with veterans who tested negative. 32 The cohort was almost all men who were similar in age to our cohort (mean=57 years) but had lower baseline kidney function (mean eGFR=30 mL/min/1.73 m2), higher mean blood pressure (150/83 mm Hg), and more cigarette smokers (76% of cannabis-only participants). 32
Strengths of our study include an adequate length of follow-up (mean=4.5 years) to predict long-term renal outcomes, the use of a study cohort enriched with participants who had CKD at risk for progression, regular follow-up and prospective data collection that reduced ascertainment bias, and the assessment of cannabis use within the past 30 days to better identify chronic consumption. Of note, the prevalence of past month (∼6%) and past year (∼8%) cannabis consumption in the ASSESS-AKI cohort is similar to nationally reported estimates for U.S. adults. 38
Across the study recruitment centers, three of the four are located in states with legal medical cannabis programs and one of these had legal recreational cannabis at some point during the study period (December 2009–February 2015). Washington legalized medical cannabis in 1998 and recreational cannabis in 2012 with sales beginning in 2014; California legalized medical cannabis in 1998 and legalized recreational cannabis in 2016; Connecticut legalized medical cannabis in 2012; and cannabis remains illegal in Tennessee. Accordingly, 80% of the cannabis consumers in this cohort were recruited from the University of Washington and Kaiser Permanente Northern California.
The present study has several limitations, the greatest one being the number of participants with CKD who consumed cannabis was low and the results lack adequate power to draw definitive conclusions from. In addition, there were few cannabis consumers and therefore only a few events of CKD progression, which also limited statistical power. Despite the more rapid annual eGFR decline among people with CKD who consumed cannabis, the lack of association with CKD progression could be due to a relatively small absolute annual change in eGFR. Compared to nonconsumers with CKD, participants with CKD who consumed cannabis had a higher baseline SCr, UACR, BMI, and DBP in addition to having a lower annual income, and an increased likelihood of being permanently disabled, all of which are established risk factors for, or are clinical markers associated with kidney disease, and we cannot exclude residual confounding effects that contributed to the faster annual eGFR decline.
Additionally, the retrospective nature of this study is hypothesis generating but is unable to demonstrate causality. Alternatively, we cannot exclude reverse causality in which sicker participants with progressive CKD at baseline may have been more inclined to consume cannabis medicinally for symptom management. Cannabis consumption was determined by self-report on a questionnaire, and the reliability of questionnaire data assessing for federally illegal behavior may have limited honest study participation, leading to reporting and selection bias with the magnitude of such effects differing by state and changing over time.
Furthermore, self-report is subject to recall bias and may underestimate true consumption of cannabis and other illicit substances. Also, the outcome measures of cannabis consumption within the past 30 days or within the last year since the last study visit do not capture the true frequency or intensity of consumption, or other aspects such as simultaneous alcohol or other drug consumption, which may be relevant to kidney or cannabis-related harms. Finally, we were unable to assess the recreational or medical motivations and reasons for cannabis consumption.
Despite these limitations, there is biologic plausibility that cannabis consumption could accelerate eGFR decline among people living with CKD, although this remains to be tested clinically in humans. CKD is typically associated with overactivation of the RAAS leading to a compensatory increase in glomerular hyperfiltration, which is characterized by a reduction in afferent arteriole resistance and increase in efferent arteriole resistance to increase single nephron GFR. CB1R activation by anandamide in rat kidney vasodilates both the afferent arteriole39,40 and the efferent arteriole, but the latter to a greater extent, causing GFR to decrease and renal blood flow to increase. 39 In the context of CKD, CB1R activation would theoretically cause excess efferent vasodilation and would be detrimental to the preservation of GFR.41,42
Kidney diseases are associated with increased kidney CB1R expression in people with CKD from diabetic nephropathy,43,44 IgA nephropathy, 43 interstitial nephritis, 43 focal segmental glomerulosclerosis, 44 obesity-related glomerulopathy, 44 and kidney allograft fibrosis. 45 In animals, CB1R expression and/or activity are increased in diabetic nephropathy,17,19,46,47 ureteral obstruction, 43 chronic intermittent hypoxia-induced kidney injury, 48 and nephrectomy models of CKD,49,50 whereas CB1R inhibition prevents the development of kidney fibrosis 43 and reduces proteinuria19,51 associated with these conditions. Accordingly, several CB1R antagonists are currently in pre-clinical development for the treatment of various kidney diseases. Also, combustion by-products found in smoke could cause oxidative stress to blood vessels,52,53 leading to impaired kidney function.
Although these hypotheses could be possible in humans, the exact clinical impact of cannabis consumption among people living with CKD and ESKD is uncertain. The ratio and degree of CB1R versus CB2R activation from cannabis-based phytocannabinoids are unknown, and the net effect is unpredictable. Similarly, complicated and nuanced pharmacokinetics, 54 and synergy among the numerous phytocannabinoids in cannabis, known as the “entourage effect,” 55 makes the cumulative physiological and pathophysiological effects difficult to predict.
With increasing acceptance of both medical and recreational cannabis use in the United States and worldwide, risk factors for kidney disease including negative social determinants of health and medical comorbidities should be addressed, particularly among those who consume cannabis and even more so among those already living with CKD. Additional research is needed to investigate the kidney endocannabinoid system, and ultimately, a large prospective study of people with and without CKD is needed to properly assess the impact of cannabis consumption on kidney health and disease. The federal illegality of cannabis in the United States severely impairs the ability to conduct well-designed clinical trials to properly inform health care providers and the public.
Footnotes
Acknowledgments
The authors would like to thank all the ASSESS-AKI study participants, research coordinators, and support staff for making this study possible. Parts of this research were presented as a poster at the American Society of Nephrology Kidney Week 2018 in San Diego, California, and as an oral presentation at the International Cannabinoid Research Society Annual Symposium on the Cannabinoids 2019 in Bethesda, Maryland.
Authors' Contributions
J.L.R.: Conceptualization, methodology, validation, writing—original draft, and writing—review and editing. H.Z.: Methodology and formal analysis. G.B.F.: Methodology, data curation, resources, and project administration. K.C.: Methodology and visualization. E.D.S.: Writing—review and editing, and investigation. M.M.W., A.X.G., and T.C.T.: Investigation and supervision. J.S.K.: Writing—review and editing, investigation, and supervision. V.M.C.: Methodology, validation, formal analysis, investigation, resources, data curation, writing—original draft, writing—review and editing, visualization, supervision, and project administration. S.G.C.: Conceptualization, methodology, validation, formal analysis, investigation, writing—original draft, writing—review and editing, and supervision.
Disclaimer
The views expressed in this article are those of the authors and do not reflect the views or policy of the Department of Veterans Affairs or the U.S. government.
Author Disclosure Statement
J.L.R., H.Z., G.B.F., K.C., and T.C.T. have nothing to disclose. E.D.S. reports consultancy agreements with Akebia Therapeutics; honorarium for an invited educational talk on AKI epidemiology at the DaVita Annual Physician Leadership Conference; editorial board for CJASN; and author for UpToDate (royalties). M.M.W. reports consultancy agreements with Roche Diagnostics; research funding with Roche; and honoraria with Roche Diagnostics. A.X.G. reports research funding with Astellas and Baxter; editorial board for American Journal of Kidney Diseases and Kidney International; serving on the Data Safety and Monitoring Board for an anemia trial program funded by GlaxoSmithKline, as the medical lead role to improve access to kidney transplantation and living kidney donation for the Ontario Renal Network (government funded agency located within Ontario Health).
J.S.K. reports consultancy agreements with National Institutes of Health and National Kidney Foundation; ownership interest with Amgen; associate editor for American Journal of Kidney Disease; and steering committee chair for ASSESS-AKI, National Institute of Diabetes and Digestive and Kidney Disease (NIDDK). V.M.C. reports scientific advisor or membership with Allergan, AstraZeneca, Biohaven, Janssen, Regeneron, and Sanofi. S.G.C. reports personal fees from Bayer, Boehringer Ingelheim, CHF Solutions, Quark, Relypsa, and Takeda; personal fees and other from ProKidney and pulseData; grants, personal fees, and other from RenalytixAI; consultancy agreements with 3ive, Axon, Reprieve Cardiovascular, and Vifor; ownership interest with pulseData and Renalytix; research funding with ProKidney, RRI, and XORTX; patents and inventions with Renalytix; scientific advisor or membership with Renalytix and Reprieve Cardiovascular; associate editor for Kidney360; editorial board for Kidney International, CJASN, and JASN.
Funding Information
J.L.R. was supported by the National Institutes of Health (NIH) National Institute of Diabetes and Digestive and Kidney Disease (NIDDK) grant T32DK007757. The ASSESS-AKI Study Consortium was supported by the supplemental American Recovery and Reinvestment Act funds and research grants U01DK082223, U01DK082185, U01DK082192, U01DK082183, U01DK084012, and R01DK098233 from the NIDDK of the NIH, U.S. Department of Health and Human Services. This publication was also supported by the National Center for Research Resources and the National Center for Advancing Translational Sciences, NIH, through University of California, San Francisco–Clinical and Translational Science Institute grant UL1RR024131. S.G.C. was also supported by grants R01DK106085 and U01DK106962. A.X.G. was also supported by the Dr. Adam Linton Chair in Kidney Health Analytics, and a Clinician Investigator Award from the Canadian Institutes of Health Research. E.D.S. was also supported by the Vanderbilt O'Brien Kidney Center P30-DK114809 clinical and translational core.