
Abstract
Objective:
To determine whether prenatal cannabis use alone increases the likelihood of fetal and neonatal morbidity and mortality.
Study Design:
We searched bibliographic databases, such as PubMed, Embase, Scopus, Cochrane reviews, PsycInfo, MEDLINE, Clinicaltrials.gov, and Google Scholar from inception through February 14, 2022. Cohort or case–control studies with prespecified fetal or neonatal outcomes in pregnancies with prenatal cannabis use. Primary outcomes were preterm birth (PTB; <37 weeks of gestation), small-for-gestational-age (SGA), birthweight (grams), and perinatal mortality. Two independent reviewers screened studies. Studies were extracted by one reviewer and confirmed by a second using a predefined template. Risk of bias assessment of studies, using the Newcastle–Ottawa Quality Assessment Scale, and Grading of Recommendations Assessment, Development, and Evaluation for evaluating the certainty of evidence for select outcomes were performed by two independent reviewers with disagreements resolved by a third. Random effects meta-analyses were conducted, using adjusted and unadjusted effect estimates, to compare groups according to prenatal exposure to cannabis use status.
Results:
Fifty-three studies were included. Except for birthweight, unadjusted and adjusted meta-analyses had similar results. We found very-low- to low-certainty evidence that cannabis use during pregnancy was significantly associated with greater odds of PTB (adjusted odds ratio [aOR], 1.42; 95% confidence interval [CI], 1.19 to 1.69; I2, 93%; p=0.0001), SGA (aOR, 1.76; 95% CI, 1.52 to 2.05; I2, 86%; p<0.0001), and perinatal mortality (aOR, 1.5; 95% CI, 1.39 to 1.62; I2, 0%; p<0.0001), but not significantly different for birthweight (mean difference, −40.69 g; 95% CI, −124.22 to 42.83; I2, 85%; p=0.29). Because of substantial heterogeneity, we also conducted a narrative synthesis and found comparable results to meta-analyses.
Conclusion:
Prenatal cannabis use was associated with greater odds of PTB, SGA, and perinatal mortality even after accounting for prenatal tobacco use. However, our confidence in these findings is limited. Limitations of most existing studies was the failure to not include timing or quantity of cannabis use. This review can help guide health care providers with counseling, management, and addressing the limited existing safety data.
Protocol Registration:
PROSPERO CRD42020172343.
Introduction
With increasing legalization, prenatal cannabis use has substantially increased, and cannabis is now the most common federally illegal drug used in pregnancy.1–4 The potency of cannabis also nearly tripled over the last two decades. 5 Approximately half of pregnant individuals who use cannabis continue to use throughout pregnancy, particularly in the first trimester during organogenesis when the fetus is most sensitive to adversity.4,6–10
Although the American College of Obstetricians and Gynecologists has advised pregnant and lactating individuals to abstain from cannabis, most continue to use partly because current safety data are limited.1,11–13 There is concern for detrimental fetal and offspring outcomes14–16 because cannabis' main active component, delta-9-tetrahydrocannabinol, readily crosses the placenta. The limited available evidence suggests that prenatal cannabis exposure is associated with stillbirth, intrauterine growth restriction, and impaired fetal neurodevelopment.15–22
Prior studies examining the association between prenatal cannabis use and adverse outcomes, including the most recently published systematic review and meta-analysis, 23 are largely limited by lack of statistical adjustment for important confounding factors, especially prenatal tobacco use. A prior meta-analysis noted that significant associations between prenatal cannabis use and higher rates of low birthweight (LBW) and preterm delivery dissipated after adjustment for prenatal tobacco use. 24 However, most studies included in that meta-analysis collected data before state-level recreational cannabis legalization. Indeed, patterns of cannabis use have changed in recent years, and the potency of cannabis itself has increased. 5
As cannabis has become more potent and perceived risk has declined, prenatal use has increased.1,2,4,5 The purpose of this systematic review and meta-analysis is to provide a contemporary understanding of the association, after accounting for tobacco use, between prenatal cannabis exposure and fetal and neonatal outcomes.
Methods
We conducted this review using standard systematic review methods and reported our findings using the Meta-analysis of Observational studies in Epidemiology (MOOSE) reporting guidelines. This review was conducted as part of the Systematically Testing the Evidence on Marijuana project, which is funded by the Veterans Health Administration's Office of Rural Health and is intended to help health care providers have evidence-informed discussions about cannabis with patients (www.cannabisevidence.org). As part of this project, we will conduct literature surveillance and update findings for this review at least once yearly.
Information sources and search strategy
We performed systematic searches of MEDLINE (Ovid), CINAHL (EBSCOHost), PsycInfo (Ovid), Global Health (Ovid), and EBM Reviews Cochrane Database of Systematic Reviews (Ovid) from database inception through February 14, 2022, based on a predesigned protocol registered with PROSPERO (CRD42020172343). An experienced research librarian developed the search strategies, which were peer reviewed by a second research librarian using the Peer Review of Search Strategies instrument. 25 Reference lists of included studies and relevant systematic reviews and meta-analyses were reviewed for additional publications of interest. Full search strategies are available in the Supplementary Data. The MOOSE reporting guidelines were followed.
Study selection
Studies were eligible if they (1) were published in a peer-reviewed scientific journal, (2) included pregnant individuals up to 1 year postdelivery; (3) included individuals for whom cannabis was the only illicit substance used during pregnancy; (4) used a cohort or case–control study design; (5) had a comparator group of noncannabis users, or lower dose or frequency users; (6) assessed 1 or more outcomes of interest; and (7) adjusted for prenatal tobacco, alcohol, and polysubstance use in statistical models.
Only English-language studies were included. The definition of cannabis exposure during pregnancy included any amount, duration, or frequency and was defined by self-report, toxicology results, or both depending on the individual study. Although toxicology testing is a more objective and precise method to ascertain prenatal cannabis use, self-report was also included due to the limited number of studies using toxicology alone. Primary outcomes were preterm birth (PTB; <37 weeks of gestation), birthweight, perinatal mortality, and small-for-gestational-age (SGA; weight <10th percentile given gestational age and sex of offspring).
Secondary outcomes were gestational age, LBW (<2500 g), neonatal intensive care unit (NICU) admissions, and Apgar score at 1 and 5 min. These outcomes were selected because they are the most evaluated outcomes in the literature and are most relevant to pregnant individuals and clinicians.
Data extraction
From each study, we abstracted details on study design, setting, duration, ascertainment of cannabis use, comparators, participant characteristics, and outcomes. Data were abstracted by one reviewer and confirmed by a second.
Risk of bias of included studies
Two independent reviewers assessed each trial for inclusion at the title and abstract and full-text levels. Two independent reviewers also assessed the risk of bias (RoB) for included studies using the Newcastle–Ottawa Scale (NOS). 26 The NOS ranges from 1 to 9 stars. For ease in interpretation and because the Cochrane Collaboration advises against use of summary numeric scores for RoB, 27 we categorized the numeric ratings as “low” (7–9), “moderate” (4–6), and “high” (1–3) RoB. Disagreements were resolved by consensus or a third reviewer. Unpublished studies and conference abstracts were included in our search, but excluded from our analysis as it has been shown that their exclusion does not change the precision or accuracy of the results. 28
Certainty of evidence
Two independent raters assigned a summary judgment for the overall certainty of evidence (CoE) for each primary outcome, using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach. 29 Disagreements were resolved by consensus. Because it would be unethical to evaluate cannabis use in pregnancy through randomized trials, observational evidence (e.g., cohort studies) will be the highest quality study design data derived for this topic. As a result, we started all outcomes at high CoE, pulling from recent guidance by the GRADE working group about nonrandomized studies evaluating interventions. 30 We downgraded each outcome one level for internal validity concerns (RoB), such as a lack of randomization and vulnerability to confounding.
Data synthesis
For our data synthesis, we conducted an overall qualitative synthesis of all eligible studies for our four primary outcomes (PTB, birthweight, perinatal mortality, and SGA). Then, for studies that reported sufficient data for quantitative syntheses, we conducted meta-analyses of those studies reporting unadjusted effect size estimates, followed by separate meta-analyses of those reporting adjusted effect sizes for each of our primary outcomes. We conducted both qualitative and quantitative analyses because of variation in how data were reported in eligible studies and statistical heterogeneity we detected in our meta-analyses.
For the meta-analyses of unadjusted effect sizes, we first calculated effect size estimates using study-reported within-group results (e.g., means and standard deviations [SDs] for continuous outcomes and counts of individuals with events for binary outcomes). For birthweight, we calculated mean differences (MDs) and 95% confidence intervals (CIs) between the exposed and unexposed groups. For PTB, perinatal mortality, and SGA, we calculated odds ratios (ORs) and 95% CIs, reflecting the relative odds of a participant experiencing an event between the exposed and unexposed groups.
We additionally conducted meta-analyses using study-reported effect size estimates that had been adjusted for confounding variables (e.g., smoking, alcohol use, race/ethnicity) for outcomes for which three or more studies reported the same type of effect size (e.g., MD, OR). For studies that reported adjusted effect sizes stratified by subgroups of cannabis use frequency, we incorporated each of the subgroups using multilevel models to account for the within-study dependency (e.g., correlated error) introduced by including multiple comparisons within a single study.
We used DerSimonian–Laird random effects models to synthesize effect estimates, and evaluated statistical heterogeneity using prediction intervals and the I2 statistic. 31 All analyses were conducted using the meta package in R, version 4.0.3 (R Project for Statistical Computing). 32
Results
Overall characteristics of studies
The study selection process is depicted in Figure 1. After reviewing 1902 titles and abstracts, we included a total of 53 studies from 127 publications. Table 1 describes the studies' characteristics. We found 1 case–control study 18 and 52 cohort studies; 31 studies were published after 2012, the year cannabis was first legalized for recreational use in Colorado and Washington. Table 2 describes the quality of included studies. We assessed 3 studies33–35 as having a moderate RoB, and 50 studies as low RoB. The included studies largely consisted of pregnant individuals who identified as non-Hispanic Black, Hispanic, or non-Hispanic White, were typically 20 to 30 years of age, had completed high school or less, and had received some form of prenatal care (Supplementary Table S1). Study participants varied in when and how often they used tobacco during pregnancy, with cannabis-using participants being more likely to use tobacco than noncannabis-using participants.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses literature flow diagram.
Included Study Characteristics
APGAR, appearance, pulse, grimace, activity, respiration; CUD, cannabis use disorder; GA, gestational age; LBW, low birthweight; MJ, marijuana; NICU, neonatal intensive care unit; NR, not reported; PTB, preterm birth; RoB, risk of bias; SGA, small-for-gestational-age.
Summary of Findings for Cannabis Use During Pregnancy and Perinatal Outcomes
Note: We started the CoE as high, with downgrading, if compared with a target RCT, as outlined in the Grading of Recommendations Assessment, Development, and Evaluation guidelines. 30
CI, confidence interval; CoE, certainty of evidence; ICD, international classification of diseases; MD, mean difference; OR, odds ratio; RCT, randomized controlled trial.
The included studies varied in how cannabis exposure was defined; some studies included only participants with regular and continued use, while others included individuals with irregular use or who discontinued use during pregnancy. Most studies relied on self-reported exposure to cannabis, while some used toxicology results or both, and few used umbilical cord or meconium testing for confirmation. Five studies35–39 used administrative databases to compare those with cannabis-related disorders to those with no diagnosis codes related to cannabis use. Studies were generally conducted in the United States; publication dates ranged from 1980 to 2022, spanning a period characterized by a significant increase in cannabis potency, emergence of different cannabis strains and routes of administration, and legalization that can influence accuracy of participant self-report.
Primary outcomes
PTB (<37 weeks)
Overall, we identified 41 studies (N=17,943,871) examining the association of prenatal cannabis use and PTB (Supplementary Table S2). Of those 41 studies, 31 studies had sufficient data to conduct a meta-analysis of unadjusted effect sizes and 12 had sufficient data to conduct a meta-analysis of adjusted effect sizes. Generally, studies reported results for any PTB; however, a small number of studies stratified results by spontaneous versus indicated PTBs. Across the 41 studies, we typically observed that cannabis use in pregnancy was associated with an increased likelihood of PTB.
In our unadjusted meta-analysis (31 studies; N=14,297,813), we also found that cannabis use in pregnancy increased the odds of PTB (OR, 1.62; 95% CI, 1.43 to 1.83; Supplementary Fig. S1). There were very similar findings among the 12 studies (N=13,928,094) that reported adjusted data for a meta-analysis (adjusted odds ratio [aOR], 1.42; 95% CI, 1.19 to 1.69; I2, 93%; Fig. 2). We rated the CoE for PTB as low and downgraded it for inconsistency (differences in magnitude of association between studies) and RoB (if compared with a target randomized controlled trial; Table 2).
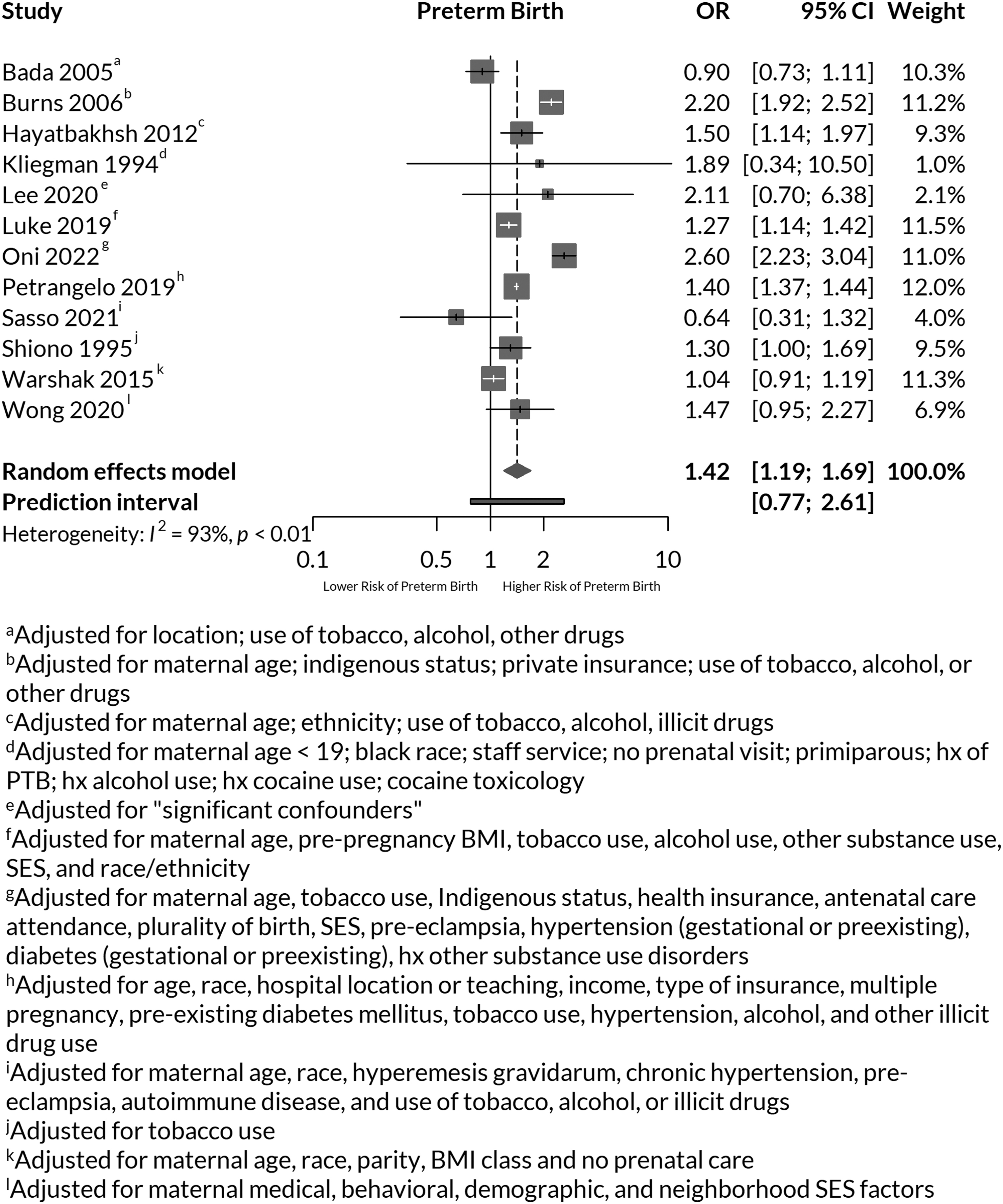
Adjusted meta-analyses of preterm birth after cannabis use during pregnancy. BMI, body mass index; CI, confidence interval; OR, odds ratio; SES, social economic status.
Birthweight
We identified 31 eligible studies (N=282,699) that reported data on birth weight, but across all studies, there was no clear, consistent association of prenatal cannabis use with birthweight (Supplementary Table S2). Of those 31 studies, 22 studies had sufficient data to conduct a meta-analysis of unadjusted effect sizes and 4 had sufficient data to conduct a meta-analysis of adjusted effect sizes. In the few studies in which cannabis use was associated with LBW, the magnitude of difference was relatively small and potentially not clinically important (∼100 to 200 g).
In our unadjusted meta-analysis of 22 studies (N=174,638), we found that cannabis use was associated with lower mean birthweight (MD, -141.62 g; 95% CI, -192.04 to -91.19; Supplementary Fig. S2). However, in our adjusted meta-analysis (4 studies of 8 comparisons; N=33,299), we found no evidence of an association (MD, -40.69 g; 95% CI, -124.22 to 42.83; I2, 85%; Fig. 3). Because of the varied findings across our included studies, we rated our CoE for the association between prenatal cannabis and birthweight as low; downgrading the relationship for inconsistency and RoB (Table 2).

Adjusted meta-analyses of offspring birthweight after cannabis use during pregnancy. MD, mean difference; SEI, socioeconomic index; WIC, Special Supplemental Nutrition Program for Women, Infants, and Children.
Perinatal mortality
We identified 17 eligible studies (N=14,141,101) that analyzed the association between prenatal cannabis use and perinatal mortality (Supplementary Table S3). Of those 17 studies, 12 studies had sufficient data to conduct a meta-analysis of unadjusted effect sizes and 5 had sufficient data to conduct a meta-analysis of adjusted effect sizes. The definition of perinatal mortality varied across studies. Some studies defined it as stillbirth, while others included miscarriage/spontaneous abortion or death before hospital discharge.
The general incidence of perinatal mortality ranged from 1% to 3% of the study samples. In our narrative synthesis of included studies, we found no consistent association as most studies were likely inadequately powered to detect a significant difference between groups. Studies that observed a difference commonly had statistical imprecision (i.e., wide CIs). In our unadjusted meta-analysis (12 studies; N=13,508,621), we observed that prenatal cannabis was significantly associated with increased odds of perinatal mortality (OR, 1.84; 95% CI, 1.47 to 2.29; Supplementary Fig. S3).
Sufficient data were present to include five studies (N=13,206,209) in an adjusted meta-analysis, and our findings remained consistent with increased odds of perinatal mortality among those who used cannabis in pregnancy (OR, 1.50; 95% CI, 1.39 to 1.62; I2, 0%; Fig. 4). One study, 38 with a weight of 95.2% in the meta-analysis, found that mothers reporting cannabis dependence or abuse, identified by international classification of diseases (ICD)-9 codes, were more likely to have an intrauterine fetal demise (OR 1.50; 95% CI 1.39 to 1.62). The overall incidence of perinatal mortality was 1.4%. The ICD-9 codes chosen were likely to be assigned only to individuals with moderate-to-heavy cannabis use during pregnancy, but not to occasional users. Ultimately, we have very low CoE that prenatal cannabis use increases the odds of perinatal mortality. We downgraded this evidence for RoB concerns and an additional two levels for indirectness, as the adjusted analysis was based primarily on the study using ICD-9 codes 38 (Table 2).
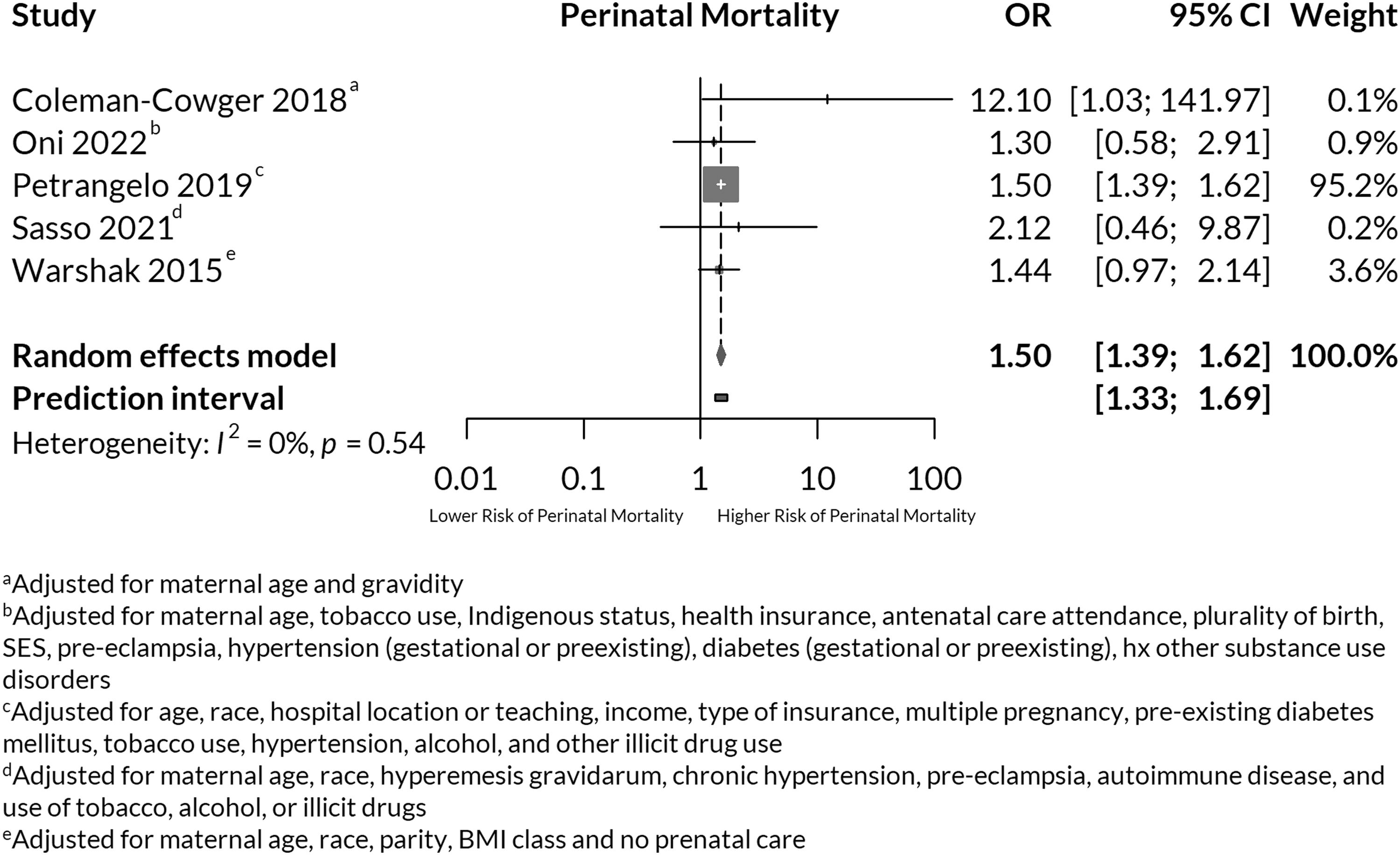
Adjusted meta-analyses of perinatal mortality after cannabis use during pregnancy.
Small for gestational age
We identified 21 eligible studies (N=4,582,445) that analyzed the association of prenatal cannabis use and SGA (Supplementary Table S3). Of those 21 studies, 18 studies had sufficient data to conduct a meta-analysis of unadjusted effect sizes and 6 had sufficient data to conduct a meta-analysis of adjusted effect sizes. Because SGA is defined as having a birthweight less than the 10th percentile, given sex and gestational age of the offspring, the expected occurrence of SGA is 10%. However, most studies reported higher proportion of events, particularly in the exposure groups. In our narrative synthesis, we observed a trend of prenatal cannabis use significantly increasing the likelihood of SGA.
Similarly, in our unadjusted (18 studies; N=1,774,485) and adjusted (6 studies; 686,336) meta-analyses, prenatal cannabis use significantly increased the odds of SGA (unadjusted OR, 2.06; 95% CI, 1.76 to 2.41; aOR, 1.76; 95% CI, 1.52 to 2.05; I2, 86%; Supplementary Fig. S4 and Fig. 5, respectively). We rated the CoE as low for increased odds of SGA with prenatal cannabis use and downgraded the evidence for inconsistency and RoB (Table 2).
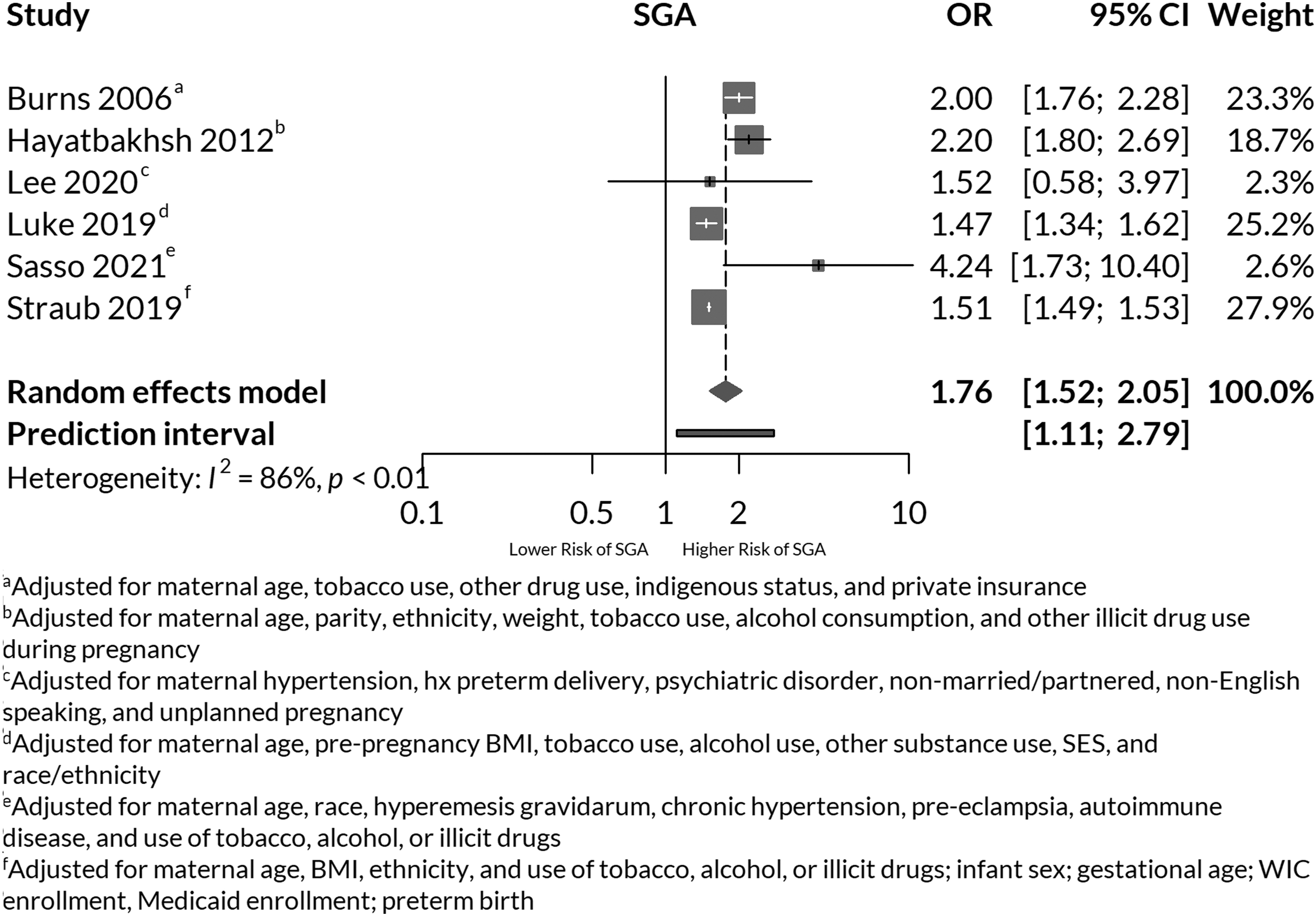
Adjusted meta-analyses of SGA offspring after cannabis use during pregnancy. SGA, small-for-gestational-age.
Secondary outcomes
We did not meta-analyze or assign a CoE rating for secondary outcomes, which included gestational age at birth (in weeks), LBW (<2500 g), NICU admissions, and Apgar scores at 1 and 5 min. Across these secondary outcomes, unadjusted or adjusted associations or both were reported (Supplementary Tables S4 and S5). Gestational age at birth was reported in 27 studies with 8 reporting adjusted measures of association. Most studies showed that prenatal cannabis use significantly reduced gestational age at birth.
Our finding for this association is comparable to our meta-analysis result for PTB. Twenty-three studies reported data on LBW with 19 studies reporting adjusted measures of association. A majority of the adjusted estimates were not significantly different between groups. This finding is also consistent in direction of association with our meta-analysis result of mean birthweight. NICU admissions were reported in 19 studies with 15 reporting adjusted measures of association. Most studies found prenatal cannabis use was associated with a significantly higher likelihood of NICU admissions (Supplementary Table S4).
Nine studies reported data on Apgar scores at 1 min with 5 studies reporting adjusted estimates, and 20 studies reported data at 5 min with 10 studies reporting adjusted estimates. Some studies reported Apgar scores as binary with cutoffs, while the majority reported means. The majority of studies found that Apgar scores at 1 and 5 min were not significantly different between groups (Supplementary Table S5).
Discussion
In this review, we found 53 studies evaluating prenatal cannabis use and relevant fetal and neonatal outcomes. Of our primary outcomes, after adjusting for confounding factors, we found low CoE that prenatal cannabis use remained an independent risk factor for PTB and SGA, and very low CoE for an increased likelihood of perinatal mortality. We found low CoE for no association with prenatal cannabis exposure and mean birthweight. Among secondary outcomes, we found that prenatal cannabis use was associated with decreased gestational age at birth, which is congruent with our observed association of prenatal cannabis use and PTB. Furthermore, we found that prenatal cannabis use was generally not significantly related to LBW, which was also consistent with our analysis of cannabis and mean birthweight. Finally, we observed that prenatal cannabis use was, in most studies, significantly associated with an increased likelihood of NICU admissions, but no consistent relationship was detected with Apgar scores.
It has been well demonstrated that PTB and SGA are strongly associated with increased offspring morbidity and mortality. 40 PTB is relatively common and affects 1 in 10 infants born in the United States. 41 SGA infants are five times more likely to die in the neonatal period and first years of life. 42 Thus, it is important to address modifiable risk factors for PTB and SGA, such as cannabis use, during the preconception or pregnancy period, which might help prevent these complications.
Compared with prior reviews focused on prenatal cannabis use, our review offers important strengths. Our review is current and comprehensive; many studies focused on examining cannabis use in pregnancy have emerged since the most recently published large systematic reviews.24,43,44 Also, similar to Conner et al, 24 our review used adjusted effect sizes in our meta-analyses accounting for confounders that were not addressed in other recent large reviews.40,41 Our review also assessed many clinically relevant prenatal and neonatal outcomes similar to three recent reviews,23,24,43 including perinatal mortality, which was not evaluated in the most recently published review. 23
Marchand et al reviewed the associations of prenatal cannabis use on neonatal outcomes through August 2021. 23 Among 16 studies, they found significant increases in 7 adverse neonatal outcomes among women who used cannabis during pregnancy, including LBW, SGA, PTB, NICU admission, decreased mean birthweight, Apgar score at 1 min, and infant head circumference. 23 However, the authors did not adjust for confounding factors in their meta-analyses (e.g., tobacco, alcohol use), which might lead to biased associations, particularly with observational data. Although our review did not meta-analyze NICU admissions, in comparison we included more studies in our analysis; excluded for polysubstance use, including tobacco and alcohol; and did not find an association between prenatal cannabis exposure and birthweight.
Conner et al searched through August 2015, and similar to us, their pooled unadjusted data demonstrated an association between prenatal cannabis use and increased risk of PTB and LBW that, unlike our review, was no longer statistically significant after adjusting for tobacco use and other confounding factors. 24 While our review also did not show a difference in mean birthweight, we did demonstrate a greater risk of SGA with prenatal cannabis use. Their review also found that prenatal cannabis use is not an independent risk factor for adverse neonatal outcomes.
Gunn et al reviewed the associations of prenatal cannabis use on fetal outcomes through April 2014 and found that infants exposed to cannabis in utero had a higher risk of LBW and NICU admission. 43 Because the authors did not account for tobacco and alcohol use, the results were likely confounded. In contrast, our review did not meta-analyze NICU admissions, but most included studies found an association between in utero cannabis exposure and increased NICU admissions while adjusting for confounders.
Our review was based on an extensive literature search, but we had strict exclusion criteria to improve the quality of eligible studies, which likely reduced the number of included studies. Additionally, the existing literature for our review was limited by observational study designs and most studies included in our review determined cannabis use by participant self-report, which can underestimate the prevalence of cannabis use in pregnancy.44,45
Pregnant individuals also underreport their cannabis use by up to 60–70% of their actual use and there is no biological validation for self-reported dosing.11,46,47 Even when use is reported accurately, it is hard to quantify and compare reported usage due to the lack of standardized dosing and routes of cannabis administration. Toxicological testing is preferred in lieu of, or in conjunction with, self-report. While more accurate than self-report, toxicology screening can also be limited by cross-reactivity with other substances, lack of sensitivity to detect intermittent use, overestimation of ongoing use, and an inability to determine timing and quantity of use.
Also, given the heterogeneity of the literature and limited overlapping measures between studies assessed, we were unable to ascertain the association of timing, frequency, quantity, concentration, or duration of prenatal cannabis use on fetal and neonatal outcomes. In addition, a majority of the included studies did not differentiate the mode of cannabis administration. Because smoked cannabis is the most common form of use in pregnancy, 48 it is possible that our observed detrimental associations of cannabis on neonatal outcomes could be, in part, explained by the adverse prenatal effects of smoke inhalation. Comparative studies of different modes of cannabis administration are needed to better understand the effect of cannabis on pregnancy and neonatal outcomes.
Existing studies have also described an adverse association on offspring neurological development from maternal cannabis use in pregnancy, including an increased incidence of autism spectrum disorder.43,46,49 Although our review included neonatal outcomes, we excluded studies that reported long-term offspring neurodevelopmental outcomes after prenatal cannabis exposure.
Conclusions and Implications
The results of our systematic review and meta-analysis suggest that prenatal cannabis exposure was independently associated with an increased risk for PTB, SGA, and perinatal mortality. However, our confidence in these findings was very low or low meaning that additional studies could meaningfully change our conclusions. Future research in this area should focus on the timing, frequency, route of administration, and potency of cannabis use, which is not well addressed in the existing literature.
Additionally, it is important for studies seeking to determine the association of cannabis use in pregnancy to ascertain cannabis use through screening methods with greater accuracy than participant self-report alone, and to adjust for important confounding factors, such as polysubstance, tobacco or alcohol use, or to use propensity scores or matching techniques to reduce selection biases. As prenatal cannabis use is becoming more common and cannabis potency is increasing, health care providers should discuss the uncertainty regarding the potential benefits and harms of cannabis use during pregnancy with individuals who are pregnant or trying to conceive.
Footnotes
Acknowledgments
The authors would like to acknowledge Robin Paynter, MLIS, for conducting the searches for this review, and Travis Lovejoy, PhD for assisting with study design and initial data collection.
Authors' Contributions
J.O.L.: Conceptualization, methodology, investigation, data curation, writing–original draft, and visualization. B.S.: Investigation, formal analysis, data curation, writing–review and editing, and visualization. S.R.: Investigation, formal analysis, data curation, writing–review and editing, and visualization. C.K.A.: Investigation, formal analysis, data curation, writing–review and editing, visualization, and project administration. S.D.: Investigation, formal analysis, data curation, writing–review and editing, and visualization. A.O.: Investigation, data curation. D.K.: Conceptualization, methodology, writing–review and editing, and funding acquisition. C.S.H.: Conceptualization, methodology, investigation, data curation, writing–original draft, visualization, formal analysis, and supervision.
Role of Funder/Sponsor
The funder/sponsor did not participate in the work. The findings and conclusions in this document are those of the authors who are responsible for its contents; the findings and conclusions do not necessarily represent the views of the Department of Veterans Affairs or the United States government.
Author Disclosure Statement
Authors have no conflicts of interest to disclose.
Funding Information
This research was funded by the Office of Rural Health, Department of Veterans Affairs, Veterans Health Administration, Health Services Research, and Development.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.