
Abstract
Early studies suggest medical cannabis (MC) has the potential to benefit people who suffer from chronic pain by offering a less addictive alternative to opioids; however, most investigators agree more research is indicated. Today, in 2023, cannabis remains a Schedule I drug and is an illegal substance in the United States under the Controlled Substances Act of 1970. Despite this designation, as of February 2022, 37 states, three territories, and the District of Columbia allowed using cannabis products to treat certain painful medical conditions. The contradictory status of federal and state legislation regarding cannabis use has resulted in delays and restrictions on relevant research. As a result, an inadequate foundation of knowledge exists needed to inform policy, program, and practice decisions concerning MC to treat pain. Implementing and controlling access to MC is influenced by overlapping individual, interpersonal, community, and organizational influences that all fall under the umbrella of federal and state policies. Increasingly, the legalization and expanded access to MC necessitates the integration of evidence, policy, and social–ecological reality. To adequately delineate these complex factors to anticipate and plan future interventions at multiple levels, we propose a social–ecological framework (SEF) for using MC to treat pain. This SEF assumes the transactional relationship between the individual and the environment and that no single factor can predict behavior or health outcomes. Our framework illustrates five dynamic levels of analysis that interact between dimensions. Key elements and intersections are discussed at the intrapersonal, interpersonal, institutional, community, and policy levels.
Background/Framework
In 2023, cannabis remains a Schedule I drug and is an illegal substance in the United States under the Controlled Substances Act of 1970. A Schedule I drug, by definition, is a drug “with no currently accepted medical use and a high potential for abuse.” 1 This definition means that possession of cannabis is a crime under federal law and that cannabis has no legal or recognized medical purpose. Nonetheless, according to the National Conference of State Legislatures, in February 2022, 37 states, three territories, and the District of Columbia allowed the use of cannabis products to treat certain painful medical conditions. 2 Unfortunately, the conflict between state and federal law regarding cannabis use has resulted in delays and restrictions on relevant research. As a result, there is an inadequate foundation of knowledge needed to inform policy, program, and practice decisions regarding medical cannabis (MC) to treat pain.
A recent report from the National Institute on Drug Abuse (NIDA) National Advisory Council on Drug Abuse concludes, “There is a great need for research on cannabis that informs policy and regulation of the drug, as regulators have to make many decisions about cannabis, and, by their testimony, they are currently ‘winging it’” (p. 31). 3 Following that report, in December 2022, HR 8454, Medical Marijuana and Cannabidiol Research Expansion Act, was passed by the U.S. House and Senate and signed into law by the president. 4
Studies conducted about the potential of cannabis to treat pain suggest that it can be an effective medication. Still, researchers acknowledge the limitations of their research and the need for additional studies.5–8 Relief of chronic pain is the most cited reason for using MC. 9 One study of 2897 patients utilizing MC found that more than one-third of respondents reported that cannabis provided relief equivalent to the relief they received from other medications, and almost all reported a reduction in their use of opioids and that using cannabis was more effective in treating their pain than opioids. 7 However, they concluded that more research is needed to better understand the value of cannabis “as a viable substitute for pain treatment.”
Similarly, other researchers found evidence that using cannabis can reduce the need for prescription opioids for the treatment of pain.7,10–14 However, one early Australian study found no reduction in pain or opioid reduction in a sample of 1514 participants with chronic pain who used cannabis in a 4-year prospective cohort study. 15 Similarly, studies with patients with chronic abominable pain or pain from rheumatoid conditions reported cannabis was not effective for pain management. 16
In 2017, the National Academy of Sciences published a comprehensive report on the health effects of cannabis and cannabinoids, producing almost 100 research conclusions. After reviewing the evidence, including a comprehensive systematic review of the literature on cannabis and chronic pain by Whiting et al., 17 they concluded there is substantial evidence that cannabis is an effective treatment for chronic pain in adults (p. 90). 18 In another systematic review, cannabis was found to be particularly effective for neuropathic pain 19 and has been included in clinical treatment guidelines for chronic neuropathic pain.20,21 The opioid sparing effect of cannabis has been described in basic science publications, further supporting the potential of cannabinoids to reduce opioid use for chronic pain.22–24
Cannabis has been used for its healing effects for thousands of years. Originating in China and central Asia, cannabis was used to treat ailments such as arthritis, depression, inflammation, and pain. 25 There have been more recent advancements in cannabis and cannabinoid research; for example, the use of cannabidiol (CBD), which is one active ingredient in the cannabis plant that does not cause impairment and is not addictive. In 2018, the drug Epidiolex, a CBD-based medication, was approved by the U.S. Food and Drug Administration (FDA) to treat seizure disorders. 26 Three synthetic cannabis-related medications, Marinol, Syndros, and Cesamet, have also been approved by the FDA and are available by prescription. Numerous over-the-counter CBD products are available to consumers to treat conditions such as anxiety, depression, and pain. MC's commercial and economic potential to benefit communities is vast, and growing cannabis is big business agriculture.
However, on their website, the FDA note to date that “the F.D.A. has not approved a marketing application for cannabis for the treatment of any disease or condition,” and other than the medications listed above, no other cannabis products have been approved by the FDA. 27
Access to MC, pharmacology, and cultivation of cannabis is highly regulated and controlled by many state and federal government regulatory bodies that oversee the industry. Growing cannabis is agriculture, and growing crops can influence the environment. However, environmental impact is not necessarily net negative; however, negative impacts may be given as a reason to limit cannabis cultivation. 28 For example, one could say growing cannabis is water intensive. Diverting water to cannabis farming can lead to increased pollution in growing locations that damage the environment. Indoor growing facilities use significant energy to heat, ventilate, and run the facility, and the plants emit chemicals that can impact air quality. 29 These examples may be no less harmful than growing other resource-intensive crops. The intersection of financial opportunity, ecological considerations, and abuse liability need to be balanced along with the potential benefits of MC to improve the lives of people living with chronic painful conditions.
Pending the appropriate cannabis research,30–32 it appears that MC can provide benefit to people who suffer from chronic pain by offering a less addictive alternative to opioids. 33 However, the intricacy of implementing and sustaining access to MC use will make it even more challenging. Implementing drug policy, especially with controlled substances, has had mixed results, and the mismatch between evidence, policy, and social–ecological reality can cause significant harm. 34
For example, an examination of restrictive opioid-prescribing laws in West Virginia indicates less availability of prescription opioids 35 ; however, after implementation, opioid overdoses and deaths increased, 36 perhaps because of an influx of lethal, illicit synthetic opioids. The restrictive prescribing law had downstream effects, such as provider fear of prescribing any opioids at all, 37 and led to gaps in patient care, especially for those on chronic opioid therapy. 38 There is evidence to believe when states enact MC laws, prescription opioid use decreases39–41 and opioid overdose mortality declines. 42
However, Shover et al., challenged this causal finding in an extended study replicating Bachhuber's earlier work and found opioid overdose mortality had increased, not decreased over time. 43 The opioid epidemic is a case study of why we must proactively delineate complex factors to adequately anticipate and plan future interventions and studies at multiple levels. In response, we present a social–ecological framework (SEF) for the medical use of cannabis for pain, illustrated in Figure 1. This integrative framework can guide research that will in turn inform and proactively integrate policy, program, and practice decisions regarding using MC for pain.
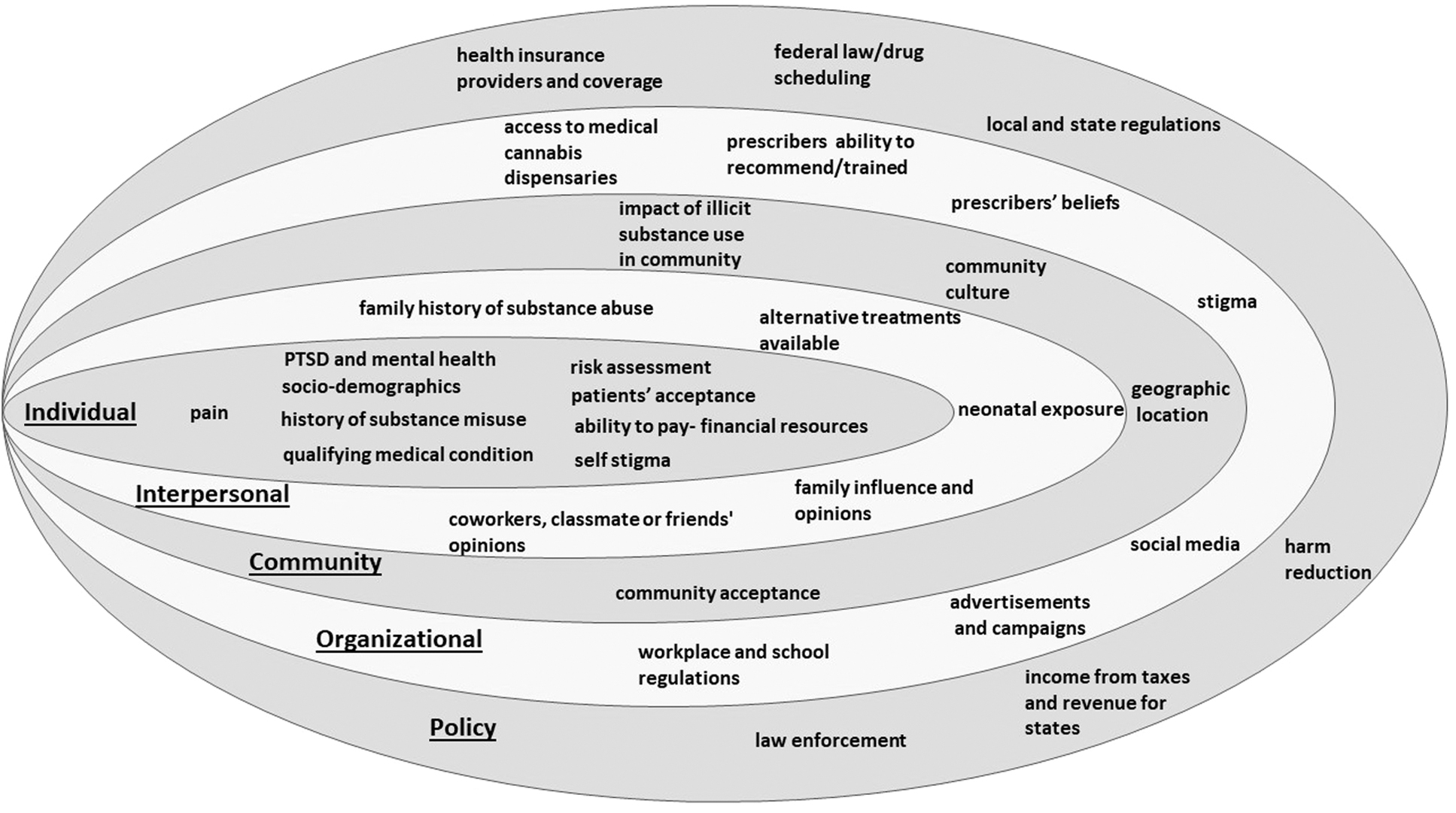
Social–ecological framework of medical use of cannabis for pain.
The SEF has been adapted and widely applied as a conceptual framework to examine the relationship among people, the environment, and health.44–46 In a SEF, health outcomes and behavior are influenced by the broader social environment. For analysis, McLeroy et al., proposed five factors that can affect health behavior: intrapersonal, interpersonal, institutional, community, and policy. 47 The SEF model assumes the transactional relationship between the individual and the environment and that no single factor can predict behavior or health outcomes.
Bookchin argues that an ecological argument for unity in diversity is “not only the determinant of an ecosystem's stability,” but also “the source of an ecosystem's fecundity, of its innovativeness, of its evolutionary potential newer, still more complex life-forms and biotic relationships” (p. 67). 48 Applying this perspective to social environments, others have argued that social–ecological systems are dynamic systems that “coevolve through interactions between actors, institutions, and resources constrained and shaped by a given social–ecological setting.” (p. 36).49–51
In recent years, the social–ecological perspective has brought attention to the dynamic relationship between various social as well as physiological determinants of health and how they are relevant for addressing both personal and public health.52–55 Acknowledging the value of a social–ecological approach to health, the Agency for Toxic Substances and Disease Registry has argued for a community-engaged approach, 56 recognizing that “community-engaged health promotion, policy making, and research is largely rooted in the recognition that lifestyles, behaviors, and the incidence of illness are all shaped by social and physical environments.” 57
The use of MC is well suited to this model because of the personal, social, and policy implications surrounding the legal use of this Schedule I drug. Our framework illustrates five dynamic levels of analysis that interact between dimensions; however, the model is not meant to be exhaustive. We will discuss key elements in each level below.
Individual Level
At the individual level, personal traits and sociodemographic details such as economic status, age, and beliefs influence behavior. These traits include health, medical conditions, employment status, attitudes toward MC, and other unique characteristics, such as sex and race. Individuals who live in a state that endorses the medical use of cannabis must meet specific health criteria. Primarily they must acquire a physician's recommendation to use MC based on a list of qualifying medical conditions. The list varies by state, but most include chronic painful conditions. MC for chronic pain has been shown to reduce opioid use and improve function58–60 ; however, despite the growing demand for less harmful opioid substitutions, cannabis remains a Schedule I drug. Indication for use may vary by age, as indicated in a study of 217 MC users in San Francisco. Middle-aged adults (31–50) were more likely to use MC for insomnia, whereas older (51–72) users were more likely to use MC for chronic conditions, including chronic pain. 61
Studies on MC, including demographics such as race, have found that most users are White.62,63 Following legalization for adult use, non-Hispanic Whites and Hispanic use went up, but no increase in use was identified in the non-Hispanic Black users. Black cannabis users have faced racialized targeting during prohibitive cannabis legal enforcement. 64 The American Civil Liberties Union in 2020 reported that Black people are 3.65 times more likely than Whites to be arrested for possession of cannabis, and the racial disparity persists even in states that have legalized or decriminalized cannabis use. 64 A history of racially biased prosecution for cannabis possession could make MC less acceptable to people of color and contribute to stigma at the individual level. 65
Although the use and normalization of MC are increasing, a well-entrenched stigma remains associated with using a previously illicit drug. Most people who access MC are not cannabis naive. 66 Prior use, under the threat of prosecution, can influence patients to conceal MC use and perpetuate stigma. Additionally, MC users report internalizing the stigma associated with the recreational use of cannabis. 67 Overcoming the internalized stigma associated with cannabis use is key to the acceptance of MC as a legitimate and useful medication. 68
Bringing the cannabis community into view and highlighting diversity, identifying users within social networks, and challenging perpetrators of deliberate misinformation could improve acceptability and reduce the stigma of MC use for individuals. 69 The acceptability of MC use for an individual encompasses many other factors, including employment and the ability to pay for annual qualifying physical exams and cannabis products. Mental health issues or a history of substance use disorder could be exacerbated by cannabis use and should be considered at the individual level when contemplating MC use for chronic pain.70,71
Interpersonal Level
The interpersonal level includes relationships with others, such as family, friends, and health care providers. These relationships can influence the use or nonuse of MC in various ways. The influence of family and friends can be stronger than medical advice.69,72 Patients whose family and friends are more accepting of MC use are more open to MC use themselves. 69 Established relationships with others can also influence MC use. For example, patients who had a regular provider and completely trusted them were twice as likely to report they would use MC if their provider recommended it. 73 Conversely, people with strong religious connections may be more likely to believe in the harmful effects of cannabis and less likely to consider MC as a treatment option. 74
The increase in recreational and MC use brings associated risks for children. With any medication that is left unsecured and accessible to small children, accidental ingestion is a real possibility. Indeed, poison center calls for cannabis exposure increased from 2017 to 2019, primarily for young children 3–5 years old and involving an “edible,” which can resemble a candy product. 75 The research on neonatal exposure to smoked cannabis indicates it can contribute to low birthweight; however, these findings are consistent with the effects of smoking tobacco during pregnancy. 18 Research is insufficient to support other adverse outcomes for prenatal, perinatal, or neonatal exposures. 18 Other risks to children include secondhand smoke exposure containing tetrahydrocannabinol (THC) and cancerogenic chemicals similar to tobacco. 76
For patients considering MC, the perceived stigma associated with cannabis use can delay access and cause people to conceal their subsequent use from unsupportive family, friends, and health care providers. 77 One Canadian study emphasized the need for health care providers to include family and school faculty in the MC education they provide to improve acceptance and reduce the stigma associated with pediatric use. 78
Patients who disclose their use of MC to their health care provider can face health discrimination. For example, people who are “active substance abusers” are usually removed from transplant lists. Heart surgeons are advised to use caution when considering a patient who uses cannabis for a heart transplant. 79 In a recent review of the literature on cannabinoids and solid organ transplantation, the authors noted few adverse effects on commonly tracked outcomes for organ transplants but urged clinicians to utilize an interprofessional psychosocial care model to assess a patient's candidacy for an organ transplant. 80
Patients will sometimes substitute cannabis for their prescription medication but will not disclose this to their health care provider. 81 These concerns are related to a lack of confidence in their providers' knowledge and ability to integrate MC into their treatment. 81 Additionally, the use of cannabis could be considered a violation of a “pain contract,” meaning patients could be cut off from their other pain medications or even discontinued from treatment. 82
Community Level
Building on the personal and interpersonal level lies the influence of the community. Organizations, networks, and the built environment where people live and work all influence health behaviors. MC use may be less acceptable in some communities. For example, communities recently decimated by the opioid crisis may be less likely to welcome an MC dispensary despite research indicating MC use can possibly decrease prescription opioid use and lower rates of opioid overdose. 8 Similarly, communities with anticannabis political underpinnings may be resistant, despite the legal status in their state.
A history of an illicit cannabis market in the community, or possibly an ongoing local illegal market for cannabis, could influence how local people feel about having a legal dispensary in their community. Local town boards can primarily influence the decision to allow a MC dispensary in a community. Permits for dispensaries are often rejected, citing concerns about increased crime, traffic, and easy access to cannabis by local children, and some communities institute complete bans on dispensaries altogether. 83
However, the acceptance of MC to treat painful conditions is changing. At least one community that previously rejected a dispensary has changed course and now recognizes the economic benefits to their community, 84 and researchers have demonstrated the value of interdisciplinary partnerships to improve acceptance of local dispensaries. 85 Nevertheless, cannabis dispensaries are subject to advertising restrictions, community licensing, zoning, and distance limitations (to schools or public parks) managed by local and state governments. 86
Organizational
There are organizational barriers and facilitators to MC that impact access for people with qualifying painful conditions. For example, variations in provider attitudes surrounding cannabis use may influence intentions to recommend use for cancer or chronic pain. 87 Patients wanting to access MC may have to seek a certified and willing physician if their own provider is not supportive or does not recommend its use. 88 Prescribers have been reluctant to recommend MC to their patients. Currently, because cannabis is still a Schedule I drug, it is illegal for providers to “prescribe” it, and even by recommending it, they risk opening their practice to a Drug Enforcement Administration (DEA) investigation. 89 Again, this is where the state and federal laws are at odds. A proliferation of MC card providers has established an online presence, perhaps to fill the void of reluctant, qualified primary care providers. Moreover, the process of becoming a qualified health care provider to recommend MC varies state to state.
Schools and workplaces can have strict policies regarding MC use. Again, these institutions are placed between conflicting state and federal regulations. To keep federal funding, public schools are bound by Drug-Free Workplace laws meaning employees and students can be prohibited from taking MC at school, even if it is legal in their state. 90 However, the National Association of School Nurses offered some accommodations in a position brief in 2019. Their position states that only FDA-approved cannabis medications (such as Epidiolex) 91 are allowed in the school setting. 92 Institutions implementing drug testing can adopt a zero tolerance for testing positive for cannabis despite legalization and legitimate medical use. It is generally agreed that this is a “gray” area and up to the employer to assess risk. Some states, such as Maine, have included protections for authorized activity (legal MC use) in their statutes to protect MC use in schools by employees and students. 93
Occupations, such as physicians and nurses, are normally subject to a zero-tolerance drug test, even if they are not impaired and have not taken their MC for days. 94 The length of time MC can produce a positive result on a drug test makes using MC prohibitive for most professions subject to testing.
Social media inform many people's attitudes and opinions of health issues, including using MC. For example, messaging using a stigmatized illness produced negative attitudes toward MC use. At the same time, less stigmatized illness was more favorably accepted as appropriate use of MC. 95 Marketing of cannabis on social media sites is also a developing industry as dispensaries navigate the need to reach potential patients despite restrictions on drug and alcohol advertising.
Policy
The use of MC is highly regulated at the state and federal levels. The FDA approves cannabis and cannabis products such as CBD. Any product that violates the Federal Food, Drug, and Cosmetic act is subject to investigation, and action is taken against offenders who unlawfully market their product or endanger the health of the public. 96 The FDA acknowledges the public interest in cannabis products and therapies and states it is working with state, local, tribal, and territorial regulatory officials in an intergovernmental capacity as cannabis regulations develop. 96 Recently, in a FDA statement, the FDA concluded that the existing regulatory framework is not appropriate for CBD, and they will work with Congress to develop a new regulatory framework. 97
The disconnect between state and federal regulation of cannabis creates a myriad of issues for consumers and industry workers. Federal law, as of this writing, classifies cannabis (nonhemp) as a Schedule I drug along with other drugs such as heroin or lysergic acid diethylamide. However, many state legislatures have legalized the medical and recreational use of cannabis. Banks have been reluctant to engage with state-licensed cannabis businesses because it could subject them to criminal and civil liability or sanctions under the Controlled Substances Act. 98 A person holding a federal Department of Transportation certification could lose their certification if they test positive for cannabis, even if it were used legally in another state and they were not impaired. 98 Business lawyers may be hesitant to advise cannabis companies because they may be violating their oath. 98 Cannabis users are also at odds with the Second Amendment of the U.S. Constitution. The gun control act of 1968 prohibits people who use unlawful controlled substances to own or possess a gun.
A letter from the Bureau of Alcohol, Tobacco, Firearms, and Explosives to registered firearm dealers in 2011 reinforced that MC cardholders cannot be sold a firearm, and there are no exceptions. 99 There have been challenges to this rule, and the gun ban for cannabis users has been found to be unconstitutional. 100 Nonetheless, the current legal restrictions mean MC users can use their recommended medication or preserve their right to bear arms, but not both.
The existing federal laws also mean insurance companies will deny coverage for MC, even if it is legal in one's state. This action is supported by an “illegal acts exclusion” in most policies. Travelers are advised to dispose of their MC before traveling out of state. Airports provide “Amnesty Boxes” for people to leave their MC before travel (Fig. 2). Federal law supersedes state law when in direct conflict, and even if you have legally obtained your medication in your own state, transporting it to another state (even if legal there) can be considered a federal crime and classified as drug trafficking. 101

Cannabis amnesty box O'Hare airport Chicago Illinois January 2023.
In the case of MC use, there are parallel laws and overlapping jurisdictions across the United States. In response to this disparity, Congress has temporarily prohibited the Department of Justice from spending any funds to restrict states from developing their own cannabis laws. 102 However, this could change with each fiscal year. People who use MC need to be aware of the laws where they are traveling, as reciprocity laws vary from state to state. In any event, some airlines, such as American Airlines, still outrightly ban any cannabis products on their flights. 103
Additionally, the disconnect between state and federal cannabis regulation stifles research into the safety and effectiveness of cannabis and cannabinoid products. A recent monograph published by the Journal of the National Cancer Institute outlines three regulatory hurdles impeding this research. These are federal regulations, drug sources, and funding. 104 The U.S. federal regulations classifying cannabis as a Schedule I drug severely restrict access to cannabis for research purposes. As such, there are limited sources, including NIDA's Drug Supply Program for researchers to request access to cannabis for investigative purposes, 105 although in 2022, the DEA awarded a seventh cannabis cultivation license to increase the number of growers for research purposes. 31
Researchers who order cannabis for research must submit a request package with multiple requirements, including evidence of DEA Schedule I registration and FDA investigational new drug authorization. 106 The FDA website outlines the lengthy seven-step process to obtain approval to conduct research using cannabis controlled under Schedule I with a 0.3% THC. 27
Funding for cannabis projects is improving; however, a successful proposal must include feasibility. Institutional support, expertise, experience, and a Schedule I license are required if cannabis is the study medication under investigation. 104 Cannabis research to treat pain is arduous and nearly impossible for early-stage or new researchers secondary to these rules and regulations. This lack of research has downstream effects. The development and approval of new pharmaceutical drugs is lengthy and costly. The FDA outlines the five steps required to gain approval from discovery and development to post marketing safety monitoring. 107 While cannabis is a known compound, there is still an immense amount of research to be done in the development phase in the United States. Scientific research into cannabis drug interactions, absorption, gender or race differences, effectiveness studies for various chronic pain conditions along with clinical research are some of the ground work needed for FDA approval.
If cannabis were evaluated and approved for use with this level of regulation, it could alleviate prescribers' hesitancy to recommend. Other countries, such as Canada, which legalized cannabis in 2018 are experiencing a significant growth of research into cannabis use for numerous indications, including acute and chronic pain.
In this article, we illustrate how a social–ecological perspective recognizing the dynamic interaction of the individual, interpersonal, institutional, community, and policy levels can help us to better understand and respond to health outcomes, particularly in terms of the use of MC to treat chronic pain. Above, we discussed the impact at each level. But given the current legal, social, and political status of cannabis and the current state of knowledge about the potential use of cannabis as a medical treatment, the need for a better understanding of the complex interplay of different dimensions of social and environmental experience is evident.
For example, an individual suffering from chronic pain, with their doctor might consider cannabis a potentially suitable treatment, but local legislation may consider such treatment a crime; or perhaps in the community where the individual lives, or even in their family or among their peers, there is a stigma attached to using cannabis for any reason; or maybe they are employed, and their employer would terminate their employment for using cannabis; and of course, there may be concerns even between the individual and their doctor about whether or not there is sufficient knowledge about the use of cannabis to feel confident that it will do more good than harm to the individual.
The point is that the decision about what the individual should do to improve their personal health in this circumstance is not one they can make, even with their doctor.
Conclusion
For cannabis to be accepted and used as treatment, for chronic pain or anything else, there needs to be ongoing research to show that it is an effective and safe treatment; both the individual and the people around them need to accept it without stigma, and social and political institutions need to recognize its use as legitimate. A social–ecological approach allows us to study and address the advantages and disadvantages of using cannabis to treat chronic pain in an integrated and coordinated way so we can be sure to consider all the dimensions of the physical and social environment that can impact on whether it should be acceptable for use.
Footnotes
Authors' Contributions
P.D.: Supervision, investigation, writing original draft, and writing—review and editing. H.B.: Writing original draft and editing, and writing—review and editing. T.H.: Writing original draft and editing, and writing—review and editing. C.L.S.: Conceptualization, investigation, writing original draft, and writing—review and editing. All authors approved the final version of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was institutionally funded.