
Abstract
Introduction:
Minor cannabinoids are increasingly being consumed in oral formulations (i.e., edibles, tinctures) for medical and nonmedical purposes. This study examined the pharmacokinetics (PKs) of cannabinoids tetrahydrocannabivarin (THCV), cannabichromene (CBC), cannabinol (CBN), and delta-8-tetrahydrocannabinol (D8-THC) after the first and last oral dose during a 14-day administration period.
Materials and Methods:
Sprague-Dawley rats (N=6 animals/dose, 50% female) were given an assigned dose of one of four cannabinoids (THCV=3.2–100 mg/kg, CBC=3.2–100 mg/kg, CBN=1–100 mg/kg, or D8-THC=0.32–10 mg/kg) or vehicle (medium-chain triglyceride oil) through oral gavage once daily for 14 days. Blood was collected 45 min and 1.5, 3, and 24 h following the first dose (day 1) and the last dose (day 14) of repeated oral cannabinoid treatment for PK analysis. Outcomes of interest included time to maximum concentration (Tmax), maximum concentration (Cmax), and area under the concentration versus time curve (AUClast). Dose-normalized (DN) Cmax and DN AUClast were also calculated. Brain tissue was collected 24 h post-administration of the first (day 1) and the last (day 14) dose of each cannabinoid to determine concentrations in brain.
Results:
All cannabinoids tested were detectable in plasma after single and 14-day repeated dosing. DN Cmax and DN AUClast were highest for D8-THC, followed by CBC, CBN, and THCV. There was no sex difference observed in cannabinoid kinetics. Accumulation of D8-THC in plasma was observed after 14 days of administration. THCV levels in plasma were lower on day 14 compared to day 1, indicating potential adaptation of metabolic pathways and increased drug elimination. Cannabinoids were detected in brain tissue 24 h post-administration of the first and the last dose of 17–100 mg/kg THCV, 3.2–100 mg/kg CBC, 10–100 mg/kg CBN, and 10 mg/kg D8-THC.
Conclusions:
THCV, CBC, CBN, and D8-THC produced detectable levels in plasma and translocated to brain tissue after the first dose (day 1) and the last dose (day 14) of repeated oral dosing. Examination of PKs of these minor cannabinoids in blood and brain provides a critical step for informing target dose ranges and dosing schedules in future studies that evaluate the potential effects of these compounds.
Introduction
The Cannabis sativa L. plant includes a broad range of varieties ranging from “cannabis” (Indica type, Sativa type, and other hybrids) to hemp (defined as <0.03% of D9-tetrahydrocannabinol [D9-THC] by weight).1,2 Cannabis is often categorized as D9-THC dominant or cannabidiol (CBD) dominant, but it also contains other “minor” cannabinoids with unique pharmacological properties. These phytocannabinoids are often at lower levels than D9-THC and CBD in cannabis whole plant and/or extracts. The majority of states in the United States have enacted laws allowing the use of cannabis for medical or recreational purposes, and in 2018, hemp was removed from the Drug Enforcement Administration controlled substances list. As a result, there is a growing market for minor cannabinoids other than D9-THC. Selective breeding techniques have enabled cannabis varieties enriched for minor cannabinoids,3,4 and minor cannabinoids can be extracted for use as concentrates/isolates.
Cannabinol (CBN), produced from the oxidation of D9-THC, is present in higher quantities in aged cannabis. Further, additional cannabinoids can be artificially synthesized or semisynthesized from more abundant phytocannabinoids; delta-8-tetrahydrocannabinol (D8-THC), for example, is a naturally occurring isomer of D9-THC present in low levels in cannabis, but can be efficiently synthesized from hemp-derived CBD. These minor cannabinoids are often sold in formulations for oral consumption (e.g., “edibles,” tinctures, oils), 5 and promoted for medical use and other health benefits.
Sparse research indicates certain minor cannabinoids may have therapeutic potential for pain relief, improved mood, attention, and focus, reduction of anxiety, appetite and weight control, or alternatively, appetite stimulation and weight maintenance.6–11 However, empirical data on the pharmacological effects of cannabinoids other than D9-THC and CBD are very limited.
Oral cannabinoid formulations that permit accurate dosing and reduce potential harmful effects associated with smoking/vape inhalation are approved by the U.S. Food and Drug Administration (FDA). For example, the FDA has approved oral formulations of synthetic D9-THC (e.g., dronabinol and nabilone, Marinol and Cesamet, respectively), and a pharmaceutical grade, hemp-derived CBD (Epidiolex) for the treatment of specific disorders. With oral routes of administration, absorption is slower, and there is typically a lower and more delayed peak of concentrations in blood. 12 Cannabinoids taken orally also show slower elimination rates and longer duration of effects in comparison to those consumed by smoking or vaping.13,14
Minor cannabinoids tetrahydrocannabivarin (THCV), cannabichromene (CBC), CBN, and D8-THC each have a unique, and often complex, pharmacological profile with activity at the cannabinoid type 1 (CB1R) and/or cannabinoid type 2 receptors (CB2R), as well as other receptors within the central and peripheral nervous systems. 15 THCV is a homolog of D9-THC, with reported dose-dependent pharmacological activity as a CB1R antagonist and a CB2R partial agonist.16–18 CBC is a CB2R-selective agonist, and like D9-THC, also interacts with the transient receptor potential vanilloid 1 receptor. 19 CBN is formed as an oxidation product of THC secondary to light/heat exposure, and is present in highest concentrations in aged cannabis (later harvest). It is a CB1R/CB2R partial agonist with lower efficacy than THC. 20 D8-THC is an isomer of D9-THC and appears to have similar pharmacological properties.21,22
In humans, some minor cannabinoids (e.g., CBN and D8-THC) have reported subjective effects when administered alone,23–25 although data are mixed, 26 while other minor cannabinoids (e.g., THCV, CBC) may not have subjective effects on their own, 27 although they may modulate the effects of other cannabinoids, such as THC.27,28 This study examined the oral pharmacokinetics (PKs) of THCV, CBC, CBN, and D8-THC in rat plasma and brain after 14 days of oral administrations of a range of doses. Evaluation of the oral PKs of these minor cannabinoids is a critical step for informing target dose ranges and dosing schedules in future studies that evaluate their potential effects.
Materials and Methods
Subjects
Sprague-Dawley rats (N=276; 50% female) were 7–13 weeks old (170–370 g) upon study start. Food (Teklad Certified Global Diet 2016; Envigo, Madison, WI) and water were available ad libitum in the home cage. All animal work was conducted in Lovelace Biomedical animal research facilities, which are fully accredited by the Association for Assessment and Accreditation of Laboratory Animal Care. This study (institutional protocol No. FY21–110) complied with all applicable sections of the Final Rules of the Animal Welfare Act regulations and the Guide for the Care and Use of Laboratory Animals. 29
Drugs
THCV, CBC, CBN, and D8-THC isolates were provided by Canopy Growth Corporation. Cannabinoid isolates were in liquid form and were mixed in medium-chain triglyceride (MCT) oil and administered to animals at 1 mL/kg through oral gavage. Purities of compounds were as follows: THCV (25.1% D8-THCV, 77.5% D9-THCV), CBN (99.9%), and D8-THC (98.68%). Total dose of each cannabinoid was adjusted for purity. All cannabinoid formulations were analyzed with gas chromatography–mass spectrometry for stability over 14 days. Briefly, five to six replicates of individual cannabinoid formulations were analyzed at the time of preparation and after 14 days using an Agilent 4890B paired with an Agilent 5977B mass spectrometer.
All formulations were verified to be within ±10% of their initial concentrations on day 14 of stability testing (Supplementary Data S1, Supplementary Table S1). Dose selection for CBC, CBN, and THCV was informed by available CBD data (doses ≤150 mg/kg/day CBD) 30 and previous toxicology work with oral cannabigerol (CBG) (doses ≤140 mg/kg/dose) [submitted to Cannabis and Cannabinoid Research]. 31 Doses chosen for D8-THC were lower, as selection was informed by available D9-THC data, given their similar effects in pre-clinical models and binding activities in vitro. 21 A range of doses were selected to derive a full dose–response curve. Further, we targeted dose ranges encompassing currently marketed over-the-counter hemp (<0.3% D9-THC w/w) products.
Experimental design
Animals were randomized into groups (N=6/dose) and given one of four cannabinoids (THCV, CBC, CBN, or D8-THC) or vehicle (MCT oil) through oral gavage. Each rat received only one dose of THCV (3.2, 10, 17, 22, 32, or 100 mg/kg), CBC (3.2, 10, 17, 22, 32, or 100 mg/kg), CBN (1, 3.2, 10, 17, 32, or 100 mg/kg), or D8-THC (0.32, 1, 3.2, or 10 mg/kg) or vehicle for either one day (single-dose group) or daily for 14 days (repeated-dose group).
Blood collections were performed on day 1, immediately after the first-dose administration, or on day 14, after 14 consecutive daily doses. These animals had nonterminal blood collections from the jugular vein under anesthesia at 45±5, 90±5, and 180±5 min from treatment administration on day 1 or day 14. At scheduled necropsy (24 h post-dosing), animals were euthanized by intraperitoneal injection of an overdose of a barbiturate-based sedative. Terminal blood was then collected through cardiac puncture at 24 h±5 min post-dosing. Brain tissue was also collected at this time.
Blood samples (0.5±0.05 mL for nonterminal samples and 1.0±0.05 mL for terminal samples) were processed with tripotassium ethylenediaminetetraacetic acid (K3EDTA) to plasma by centrifugation (1300 g, 2–8°C, 10 min). Plasma and brain samples were stored at −80°C until analysis. Samples were analyzed for THCV, CBC, CBN, or D8-THC through liquid chromatography–mass spectrometry using methods developed at Lovelace Biomedical as described. 32 Briefly, all plasma and homogenized brain tissue samples from orally dosed animals were analyzed using a Sciex API 4000 paired with a Waters Acquity H-Class Ultra Performance Liquid Chromatography (quantification range=4–2000 ng/mL). Refer to the Supplementary Data S2 and S3 for detailed methods and validation, respectively.
Data analysis
PK data were analyzed using a standard noncompartmental method with validated WinNonlin software (Phoenix; Pharsight Corporation, Mountain View, CA) with a noncompartmental analysis (NCA) consistent with the route of administration (extravascular model) for each subject. NCA was only performed if there were quantifiable concentrations at two consecutive time points. Concentration values that were below the quantification limit (BQL) of 0.250 or 1 ng/mL for plasma and brain, respectively, were recorded, but excluded from calculations of descriptive statistics and PK analysis.
In addition, two blood samples for day 1 (one male, 22 mg/kg THCV at 3 h and one male, 100 mg/kg THCV at 24 h) and three blood samples for day 14 (one male, 1 mg/kg D8-THC at 1.5, 3, and 24 h) could not be analyzed due to insufficient quantity. Blood plasma samples from all (N=3) females from the 14-day repeated dosing of 17 mg/kg THCV group were identified as outliers and removed from further analysis: a majority of these samples (9/12) were BQL and the quantifiable samples were very low (<0.29 ng/mL) compared with males (average of 24.9 ng/mL) at the same time points.
Arithmetic mean and standard deviation of cannabinoid concentrations in plasma were calculated for each sex, drug/dose group, and time point after the first dose of THCV, CBC, CBN, and D8-THC on day 1 and after 14 days of dosing. The area under the concentration-time curve (AUClast) for each subject from time zero (immediately after drug administration) to the time point at which the last quantifiable concentration was observed was calculated with the linear up log down interpolation method.
Parameters were estimated for time of maximum observed concentration (Tmax), dose-normalized (DN) AUClast, the maximum observed concentration (Cmax), and DN Cmax. The terminal elimination phase of each concentration versus time curve was identified using at least the final three observed concentration values. The slope of the terminal elimination phase was determined using log regression with uniform weighting. Parameters derived from the terminal elimination phase were reported if they passed the reporting criteria: the coefficient of determination (R 2 ) was ≥0.8 and the extrapolation of the AUC to infinity was ≤20% of the total area (see Table 1 for all definitions of PK parameters calculated).
Definitions of Pharmacokinetic Parameters
Dose-proportionality analysis was calculated in Phoenix by using a general linear model for each treatment to check for the relationship between the average of DN AUClast and DN Cmax values with numerical dose after the first (day 1) and last (day 14) dose of repeated administration. Parameters were considered to have a dose-proportional relationship across the dose range tested if p>0.05; if p≤0.05, then that parameter was considered to have a less than dose-proportional relationship (if the estimate in the model was <0) or greater than dose-proportional relationship (if the estimate in the model was >0).
To evaluate potential accumulation across the 14-day dosing period, accumulation ratios were calculated by dividing group means of AUClast and Cmax for day 14 by the same parameters for day 1. Male:female ratios were calculated for exploratory purposes by dividing group means of AUClast and Cmax for male animals by the same parameters for female animals.
Results
Single (day 1)-dose pharmacokinetics
PK parameters after oral administration of cannabinoids are summarized in Table 2. All cannabinoids were detectable in plasma at the first time point (45 min) following the first oral dose (Fig. 1; day 1). Time of maximal concentration (Tmax) was between 1.5 and 3 h for each cannabinoid tested. On average, Tmax for D8-THC was longest, followed by CBC and CBN, and was shortest for THCV. Cmax and AUClast were highest for CBC-treated animals. However, D8-THC had higher DN Cmax and DN AUClast compared to any other cannabinoid, followed by CBC, CBN, and THCV.
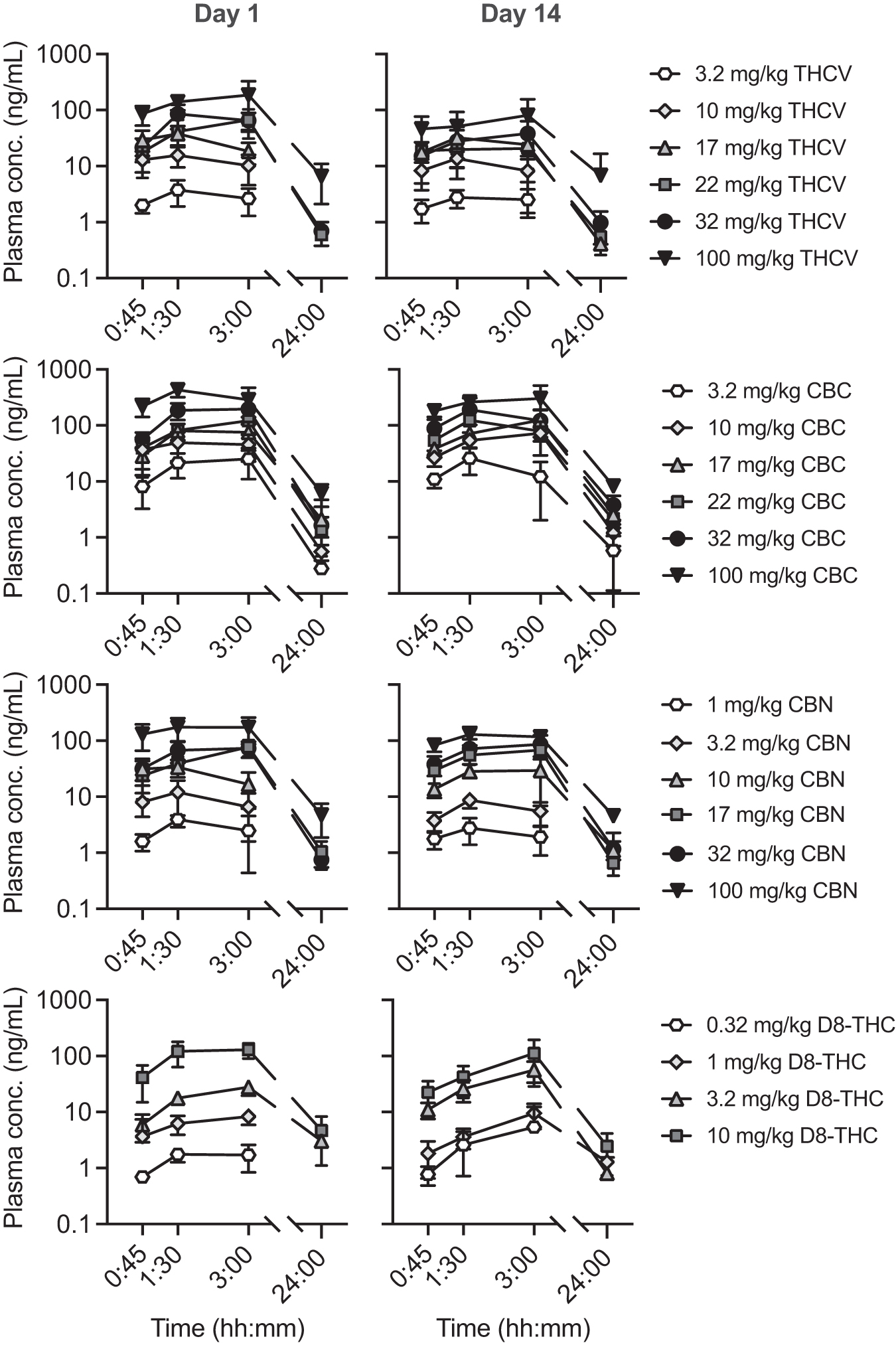
Semilog plot of cannabinoid concentrations in rat plasma following the first dose (day 1) or 14 consecutive daily doses (day 14). Data are mean±standard deviation.
Summary Pharmacokinetic Parameters for Cannabinoids in Rat Plasma After Oral Administration of a Single Dose (Day 1) of Tetrahydrocannabivarin, Cannabichromene, Cannabinol, or Delta-8-Tetrahydrocannabinol
N=6 samples per group.
CBC, cannabichromene; CBN, cannabinol; D8-THC, delta-8-tetrahydrocannabinol; SD, standard deviation; THCV, tetrahydrocannabivarin.
After 24 h, CBC concentrations were still quantifiable for most animals (3.2–100 mg/kg), but THCV, CBN, and D8-THC concentrations were only quantifiable at 24 h in animals in the higher dose groups (22–100 mg/kg for THCV, 17–100 mg/kg for CBN, and 10 mg/kg for D8-THC). On day 1, t1/2 values were able to be estimated and passed reporting criteria for only a few animals dosed with CBC and CBN at higher doses; t1/2 values ranged from 3.34 to 4.52 h.
Dose proportionality was assessed on day 1 by linear regression of numerical dose within each treatment on DN AUClast and DN Cmax ratios (Table 3). Rats treated with THCV had a greater than dose-proportional relationship for DN AUClast (p≤0.05 and estimate >0), but not DN Cmax. Rats treated with CBC and CBN had less than dose-proportional relationship for DN Cmax (p≤0.05 and estimate <0). Rats treated with D8-THC on day 1 had greater than dose-proportional relationship for both DN AUClast and Cmax.
Linear Dose–Response Summary for Dose-Normalized Noncompartmental Analysis Parameters in Rat Plasma Following Oral Administration of a Single Dose (Day 1) or 14 Consecutive Daily Doses (Day 14) of THCV, CBC, CBN, or D8-THC
Dose–response p-value <0.05 and estimate >0, indicating greater than dose-proportional relationship.
Dose–response p-value <0.05 and estimate <0, indicating less than dose-proportional relationship.
For comparisons between sexes, male to female AUClast and Cmax ratios were calculated. Most cannabinoids and dose groups had no notable difference (<2-fold change; Table 4). Exceptions on day 1 (near or greater than twofold change difference) were observed in the 32 mg/kg THCV dose group (DN AUClast and Cmax male:female ratios of 1.98 and 1.95, respectively); the 3.2 mg/kg CBC dose group (DN AUClast male:female ratio of 0.50); the 10 mg/kg CBN dose group (DN AUClast ratio of 1.96); and the D8-THC 3.2 mg/kg dose group (DN AUClast male:female ratio of 3.47). PK data disaggregated by sex are provided in the accompanying Supplementary Data S4 (Supplementary Figs. S1 and S2; Supplementary Tables S2 and S3).
Male to Female Ratios of Dose-Normalized AUClast and Cmax
Repeated (day 14)-dose pharmacokinetics
PK parameters for day 14 of repeated administration of all cannabinoids are summarized in Table 5. Following the last oral dose on day 14, all cannabinoids were detectable in plasma at the first time point (45 min) (Fig. 1; day 14). Tmax was between 1.5 and 3 h for each cannabinoid tested. As on day 1, the Tmax for D8-THC was longer on average, followed by CBN, CBC, and THCV. Similar to day 1, Cmax and AUClast were highest for CBC-treated animals; however, D8-THC had higher DN Cmax and DN AUClast compared to any other treatment, followed by CBC, CBN, and THCV treatments.
Summary Pharmacokinetic Parameters for Cannabinoids in Rat Plasma After Oral Administration of 14 Consecutive Daily Doses of Tetrahydrocannabivarin, Cannabichromene, Cannabinol, or Delta-8-Tetrahydrocannabinol
N=6 samples per group, except for 17 mg/kg THCV, which is N=3 (see “Data analysis” section).
After 24 h, CBC concentrations were still quantifiable for most animals, but THCV and CBN concentrations were only quantifiable at 24 h in animals in the higher dose groups (17–100 mg/kg). D8-THC concentrations were quantifiable 24 h after the last dose of 3.2 and 10 mg/kg. On day 14, t1/2 values were able to be estimated and passed reporting criteria for only a few animals dosed with THCV and CBC at higher doses; t1/2 values ranged from 4.23 to 4.87 h.
Dose proportionality was assessed for day 14 of repeated administration in the same manner as described for day 1. Most treatments showed a similar dose-proportional relationship (i.e., greater or less than dose-proportional) as on day 1 (Table 3). Rats treated with CBC had a less than dose-proportional relationship for DN Cmax and DN AUClast. Rats treated with CBN showed a less than dose-proportional relationship for DN Cmax. THCV and D8-THC showed dose-proportional relationships on day 14.
Accumulation of cannabinoids in plasma across the 14-day repeated-dosing period was determined using ratios of AUClast and Cmax from day 14 compared to day 1 (Table 5). Ratios tended to show a less than twofold change for most cannabinoids and dose groups, indicating no notable accumulation after 14 consecutive daily administrations. However, rats in the THCV-treated dose groups tended to have ratios <1.0 with some <0.5 (greater than twofold decrease) for day 14 compared to day 1, indicating reduced exposure after 14 consecutive daily doses. Rats in the D8-THC-treated dose groups had many ratios >2.0, indicating accumulation after 14 consecutive daily doses.
Male to female AUClast and Cmax ratios for most cannabinoids and dose groups on day 14 had no notable difference (greater than twofold change; Table 4). Exceptions on day 14 (near or greater than twofold change difference) were observed in the 3.2 mg/kg CBC dose group (DN AUClast male:female ratio of 3.90), the 10 and 17 mg/kg CBN dose groups (DN AUClast of 2.09 and 5.39, respectively), and the 0.32 and 1.0 mg/kg D8-THC dose groups (DN AUClast of 2.76 and 4.69, respectively). Ratios could not be calculated for THCV 17 mg/kg dose groups, as all female samples had to be excluded (see “Data analysis” section). PK data disaggregated by sex are provided in the accompanying Supplementary Data S4 (Supplementary Figs. S1 and S2; Supplementary Tables S1 and S2).
There was no quantifiable concentration for any cannabinoid in the vehicle control group on day 1 or day 14. Generally, for cannabinoid dose groups, the only quantifiable concentration was for the cannabinoid that was administered, although there were several nonsystematic exceptions (10 samples in total). In samples from animals dosed with CBC, there were quantifiable concentrations of THCV (two samples); in samples from animals dosed with CBN, there were quantifiable concentrations of THCV (one sample), CBC (one sample), and D8-THC (four samples); and in samples from D8-THC-dosed animals, there were quantifiable concentrations of CBN and THCV (one sample), as well as one sample with all cannabinoids quantifiable. There was no evidence for errors in performance of bioanalytical methods. Contamination of samples, however, cannot be excluded.
Brain
Concentrations of cannabinoids in brain tissue 24 h after the first (day 1) and last (day 14) dose of repeated administration are summarized in Figure 2. THCV was not detectable in brain at doses equal to or below 10 mg/kg. Mean concentrations ranged from 1.9 to 24.1 ng/g 24 h after a single dose of THCV (day 1) for 22–100 mg/kg doses and 1.9–23.6 ng/g 24 h after repeated (14 days) dosing of 17–100 mg/kg THCV. Hence, there was no difference between single and 14-day repeated dosing when measured 24 h after the last dose. CBC produced the highest concentrations in brain: all doses tested (3.2–100 mg/kg) resulted in measurable brain levels 24 h after the first (day 1) and last (day 14) dose of repeated administration dosing.
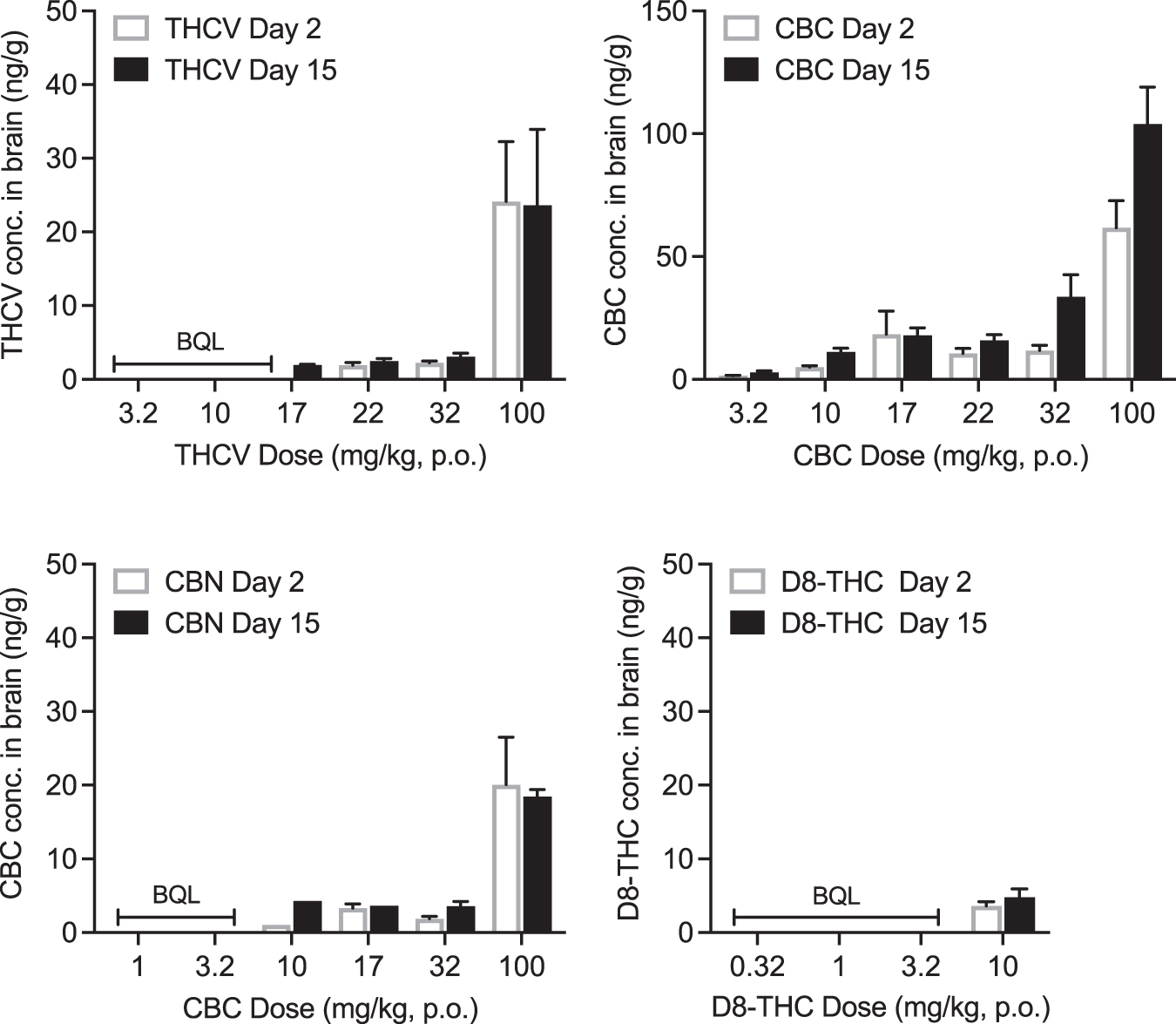
Brain concentrations of cannabinoids 24 h after a single dose (i.e., day 2; white bars) or repeated doses (14 consecutive daily; i.e., day 15; black bars). Data are group mean±standard deviation. BQL, below quantification limits (1 ng/mL).
Mean concentrations ranged from 1.5 to 61.7 ng/g after the first (day 1) CBC dose and from 2.8 to 104.0 ng/g after repeated (14 days) dosing of CBC. Concentrations for several CBC dose groups were significantly higher on day 14 after repeated administrations compared to day 1, suggesting accumulation. CBN was not detectable in brain tissue after administration of 1–3.2 mg/kg doses; CBN resulted in mean brain concentrations between 1.0 and 20.1 ng/g after the first (day 1) dose and 4.3–18.4 ng/g after the last (14 days) dose of 10–100 mg/kg CBN. There was no evidence of accumulation of CBN with repeated dosing. D8-THC was only detectable in brain 24 h after single and repeated dosing at the highest dose (10 mg/kg). Brain concentrations were low with 3.6 ng/g on day 1 and 4.8 ng/g after repeated (14 days) dosing, with no evidence of accumulation.
Discussion
The primary findings from this study were that single and 14-day repeated oral administration of THCV, CBC, CBN, and D8-THC produced dose-related, detectable levels in plasma and brain. For single-dose (day 1) administration, the PKs for THCV, CBC, CBN, and D8-THC were similar. There was also evidence that D8-THC and THCV are absorbed or eliminated differently after repeated administration when compared to CBC and CBN. As expected with oral administration of cannabinoids,33,34 there was a fairly substantial amount of between-subject variability; however, plasma concentrations and AUClast were dose orderly for all cannabinoids tested. We provide details on these key findings below.
THCV, CBC, CBN, and D8-THC were detectable in plasma after the first administration on day 1 for all doses of THCV and CBC (3.2–100 mg/kg), CBN (1–100 mg/kg), and D8-THC (0.32–10 mg/kg). Plasma concentrations of all the minor cannabinoids were detected 45 min after oral administration (1st time point), and maintained for 3 h after oral administration, with maximal concentrations (Tmax) reached between 1.5 and 3 h. THCV, CBC, CBN, and D8-THC were also detected in plasma 24 h post-administration. This is similar to what has been reported for oral administration of other minor cannabinoids (CBD, cannabidivarin, and CBG).32,35,36
There were some notable differences between the minor cannabinoids following the 14-day administration. Specifically, THCV plasma levels decreased after repeated dosing when compared to single dosing, suggesting potential adaptation of metabolic pathways resulting in increased THCV elimination. In contrast, 14-day repeated D8-THC resulted in accumulation in plasma. Importantly, in assessments of formulation stability across 14 days, there was no indication of any cannabinoid degradation in the MCT-oil vehicle as all were within 10% of their initial test concentrations.
CBC and CBN showed similar linear dose responses for DN Cmax and DN AUClast on both days 1 and 14, indicating little change in dose proportionality across the 14-day repeated-dosing period. CBC and CBN showed a less than dose-proportional relationship for DN Cmax, indicating adaptation with increasing doses. THCV and D8-THC showed a greater than dose-proportional relationship for DN AUClast on day 1, but not on day 14.
All cannabinoids tested in this study translocated to brain after single and 14-day repeated dosing. Highest brain concentrations were measured for CBC. CBC was measured in brain 24 h after a single dose in all dose groups (3.2–100 mg/kg), as well as 24 h after the 14-day repeated dosing, with accumulation observed after the 14-day repeated dosing. THCV was detectable in brain at doses >10 mg/kg, CBN was detectable at doses >3.2 mg/kg, and D8-THC was only detectable in brain 24 h post-administration of the highest dose tested (10 mg/kg).
No accumulation was observed in brain for THCV, CBN, or D8-THC. This study was not designed to assess brain concentrations immediately after dosing, rather, by looking at brains 24 h after the first dose (i.e., on day 2) and last dose of the 14-day repeated administrations (i.e., on day 15), this study solely evaluated accumulation in brain. Future studies will be needed to examine the extent and time course of cannabinoid translocation to brain tissue.
To our knowledge, this is one of the first studies to characterize and compare single- and 14-day repeated dosing PKs of a full range of doses of these minor cannabinoid isolates. Prior studies in humans have primarily examined minor cannabinoids' PKs after administration of whole plant cannabis or cannabis products, and report only low levels of these cannabinoids.37,38 To our knowledge, no clinical study to date has investigated PKs after administration of cannabinoid isolates, other than THC and CBD, and the doses received in whole plant cannabis products are not always reflective of those being taken recreationally or medicinally in isolate form.
Nonetheless, our results showing high concentrations of CBC compared with other cannabinoids are in agreement with a recent human laboratory study. Following administration of an oral cannabis product, containing CBC as well as THC and CBD, for 7 days, CBC measured in plasma was proportionally higher than CBD and THC, 39 suggesting preferential absorption or a delayed metabolism/elimination of CBC relative to THC and CBD. An important next step in understanding the PKs of these minor cannabinoids is to administer them in combination, as this reflects many commercially available cannabis products, and PK interactions have been shown between other co-administered cannabinoids (e.g., THC+CBD).40,41
In this study, there was no significant sex difference in cannabinoid kinetics. While this study was not powered to detect sex differences, the male to female ratios suggest there may be differences in exposure between sexes; thus, future studies should examine potential sex differences in PKs for these minor cannabinoids. Studies have indicated potential sex differences in THC metabolism, such that females metabolize THC at a faster rate than males.14,42 This results in higher plasma levels of the active metabolite 11-OH-THC, 42 which may underlie the greater subjective effects often reported in women. 14 This aligns with what was observed with D8-THC in this study, where males tended to have higher D8-THC concentrations than females. Research into D8-THC is still sparse; there is no evidence of any sex difference to its behavioral effects. 43
In summary, this study examined the PKs after a single dose and 14-day repeated oral administration of THCV, CBC, CBN, and D8-THC at a range of doses. These results provide critical information for identification of target dose ranges and dosing schedules in future studies, which will evaluate potential effects of minor cannabinoids.
Footnotes
Authors' Contributions
C.F.M.: Writing – original draft and formal analysis. E.M.W.: Writing – review and editing and formal analysis. J.D.M.: Writing – original draft, project administration, investigation, and formal analysis. W.D.: Writing – review and editing, investigation, and formal analysis. D.S.: Writing – review and editing, investigation, and formal analysis. J.J.: investigation. J.K.: Writing – review and editing, project administration, and conceptualization. T.W.L.: Writing – review and editing, project administration, and conceptualization. M.O.B.-M.: Conceptualization and writing—review and editing.
Author Disclosure Statement
Authors J.K., T.W.L., and M.O.B.-M. were full-time employees of Canopy Growth Corporation, a producer and retailer of cannabis and hemp products, at the time of this project; M.O.B.-M. is a current employee of Charlotte's Web, a producer and retailer of hemp products. Author J.D.M. has received funds from Canopy Growth Corp. for contract pre-clinical research. Authors E.M.W. and C.F.M. have received funds from MyMD Pharmaceuticals, Inc., and MIRA-1 Pharmaceuticals, Inc., for contract pre-clinical research. E.M.W. has received support for clinical research projects from Cultivate Biologics LLC and Canopy Growth Corp. Authors W.D., D.S., and J.J. have nothing to disclose.
Funding Information
This research was funded by Canopy Growth Corporation and conducted under contract with Lovelace Biomedical.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.