
Abstract
Introduction:
Cannabidiol (CBD), a phytocannabinoid isolated from cannabis plants, is an interesting candidate for studying its anti-inflammatory effects, especially in the pre-clinical and animal models. Its anti-inflammatory effects, such as reduction of edema and arthritis, have been demonstrated in animal models. However, topical CBD administration requires further evaluation of CBD dosage and efficacy in animal models and clinical settings.
Methods:
This in vivo study investigated the anti-inflammatory effects of topical CBD administration in an animal model. Scientific experiments, including the formalin test, writhing test, carrageenan-induced edema, histopathological examination, and detection of various proinflammatory mediators, were performed.
Results:
The anti-inflammatory effects in vivo after inflammation induction, represented by decreased times of paw licking, degree of paw edema, and decreased writhing response, showed that 1% of tropical CBD use had significantly comparable or better anti-inflammatory effects when compared with tropical diclofenac, an anti-inflammatory agent. Moreover, the anti-inflammatory effects were significant compared with the placebo. In addition, the histopathological examination showed that topical CBD drastically reduced leukocyte infiltration and the degree of inflammation. This study also showed that the levels of various proinflammatory mediators in the plasma of mice treated with topical CBD did not differ from those treated with diclofenac.
Conclusions:
The topical administration of 1% CBD gel is a potentially effective candidate for an anti-inflammatory agent. Candidate for an anti-inflammatory agent.
Introduction
Cannabidiol (CBD) is a phytocannabinoid extracted from Cannabis sativa (family Cannabaceae). This compound has a low binding affinity for cannabinoid receptors, resulting in fewer or no psychological effects. 1 CBD is widely used as an anti-inflammatory agent in animal models and clinical studies because of its nontoxicity and appropriate therapeutic window.2–4 Its anti-inflammatory effects reduce inflammatory arthritis in animal models.3,5 As a possible mechanism of action, the CBD probably decreases arthritis by regulating intracellular calcium and reducing the production of interleukin-6 (IL-6), IL-8, or matrix metalloproteinase-3 (MMP-3) in synovial fibroblasts. 6
Moreover, the anti-inflammatory mechanism of CBD involves interactions with host molecular molecules, including peroxisome proliferator activated receptor gamma, G protein-coupled receptors 3/6/12/18/55, transient receptor potential vanilloid 1/2 (TRPV1/2), transient receptor potential subfamily A1 (TRPA1), 5-hydroxytryptamine receptor, and mitochondrial proteins.7–10 Moreover, a clinical study evaluating long-term safety and efficacy of “oral CBD” in children and adults demonstrated that it is acceptable. 11 However, the pharmacological efficacy may decrease when used through the oral route because of the high first-pass metabolism of cytochrome P450. Moreover, oral CBD bioavailability is very low (13–19%). 12 The potential explanation for these pharmacokinetics is that the kidney largely excretes CBD metabolites before entering the circulatory system. 13
Oral synthetic CBD failed to relieve pain in patients with hand osteoarthritis and psoriatic arthritis with a randomized control trial. 14 Recently, modified oral lipid formulations of CBD have been developed that display a dose-dependent effect on animal plasma and brain concentrations. In addition, bioavailability was improved by approximately three times compared with lipid-free formulations. 15 However, topical administration routes are likely to overcome insufficient bioavailability and provide potential therapeutic effects for skin disorders. An investigation demonstrated that 1–10% CBD in a gel form was well absorbed and exhibited a linear relationship with dose titration. 16
In addition, this concentration range decreased inflammation in a monoarthritic rat model. 5 Unfortunately, the U.S. Food and Drug Administration currently does not approve any CBD gel form for anti-inflammatory use because of a lack of scientific and pharmacological studies. Only approved oral CBD, such as Epidiolex®, can be used as prescription drugs to treat Lennox-Gastaut and Dravet Syndrome, whereas Sativex® has been studied in the clinical trial process.17,18
A systematic review and meta-analysis demonstrated a potential reduction in pain with a nonoral CBD regimen. 19 However, a recent systematic review released by the International Association for Study of Pain Presidential Task Force on cannabis and cannabinoid analgesia reported a lack of benefits of CBD in pain management; however, no topical CBD regimen was included. 20 Both systematic reviews reported low quality of all trials included in the meta-analysis.19,20
This study provides further information on the use of CBD gels as anti-inflammatory and antinociceptive agents. Regarding the clinical use of CBD, in-house CBD gel forms were formulated and used to evaluate the pharmacological effects in animal models.
Materials and Methods
Animals
The animal protocols were reviewed by the Institutional Animal Care and Use Committee of Thammasat University, Thailand (Approval No. 010/2021). Male ICR mice and Sprague-Dawley rats were obtained from Nomura Siam International (Thailand). Both types of animals were housed in the Laboratory Animal Center of Thammasat University under a proper supply of food and standard conditions (temperature 22±1°C, 30–70% relative humidity, light 130–325 lux, and a 12 h/12 h light–dark cycle) for a week before experiments.
Chemicals and drugs
Lambda-carrageenan, absolute ethanol, hematoxylin and eosin (H&E) staining solution, ethylenediaminetetraacetic acid, and acetic acid were purchased from Sigma-Aldrich, Milano, Italy. CBD powder was purchased from Suranaree University of Technology, Thailand. Diclofenac, levomenthol, carbomer, strong ammonia solution, and formaldehyde were purchased from Tokyo Chemical Industry (Tokyo, Japan). Ten percent formalin solution was prepared from 37% formaldehyde stroke solution.
In-house CBD gel formulation
CBD powder, propylene glycol, ethanol, ammonia solution, and paraben were dissolved in water and mixed with carbomers during the gel-forming process.
Formalin test
The formalin test was performed as previously described.21,22 In briefly, mice were applied with either 0.3 mL of a placebo (control), 1% diclofenac (anti-inflammatory drug), 1% CBD, or 1% CBD combined with 4% levomenthol gel at the right hind paw and restrained in an acrylic restrainer cage for an hour before the experiment. Then, each mouse was injected with 20 μL of a 2.5% formalin solution into the dorsal surface of the right hind paw, using a 30-gauge needle with a Hamilton micro syringe.
After the injection, the mice were placed in a glass cylinder and observed for two phases of time: phase I or early phase (at 0–5 min, early phase) and phase II or late phase (15–30 min) for postformalin injection evaluation. The 45° angle of the mirror under the cylinder was used for paw observation. The time spent licking or biting the mouse paws was counted during phase I (indicating neurogenic pain) and phase II (indicating inflammatory pain) after formalin injection. The time spent licking or biting represents a nociceptive response related to pain-associated behavior in response to formalin injection.
Writhing test
The acetic acid-induced writhing test was performed according to the protocol described by Koster et al.23,24 Mice were applied with either 0.3 mL of a placebo, 1% diclofenac, 1% CBD, or 1% CBD combined with 4% levomenthol gel on the abdominal and restrained in an acrylic restrainer cage for 1 hour before the experiments. Nociception was induced by 0.6% acetic acid (10 mL/kg) intraperitoneal. The mice were then placed in a glass cylinder to observe abdominal stretching and/or pelvic rotation (of at least one hindlimb) as a writhing response. The number of writhing responses was counted every 5 min for a half-hour after induction with acetic acid.
Carrageenan-induced edema
Carrageenan-induced edema was used to evaluate the anti-inflammatory effects of CBD in rats. Rats were treated with either 0.5 mL of a placebo, 1% diclofenac, or 1% CBD gel on the right hind paw and restrained in an acrylic restrainer cage for 1 hour before the carrageenan induction. Initially, 0.1 mL carrageenan (1% w/v in saline) was injected into the plantar of the right hind paw. Paw volume, representing the degree of inflammation, was measured using a plethysmometer (Ugo Basile, Varese, Italy) at baseline and 1, 2, 3, and 4 h after injection.
Histopathology analysis
Six hours postcarrageenan injection, the rats were sacrificed with isoflurane and confirmed by cardiac puncture. The right hind paw of each rat was cut to ∼2 cm and fixed in a mixture of 10% neutral buffered formalin and 10% EDTA for 12 h and processed in Leica tissue processor equipped with Peloris II premium tissue processing system, embedded in a paraffin block, cut into 2 μm thick sections and stained with H&E. A senior pathologist performed the histological analysis using a light microscope.
The degree of inflammation was assessed by selecting the area of maximal infiltration with inflammatory cells in each case and grading the density of inflammatory cells into three tiers: grades 1, 2, and 3. The criteria for grading were as follows: grade 1 was defined as sparse inflammatory cells, grade 3 showed distinctly high cellularity of inflammatory cells, and grade 2 showed that the density of inflammatory cells lies between these two grades. The assessment was blindly performed, without knowing the information regarding each specimen.
Blood samples
Six hours after postcarrageenan injection, the rats were sacrificed using isoflurane, an anesthetic agent. Cardiac puncture of blood samples was performed by a veterinarian. Blood samples of each rat were collected in EDTA K2/gel tubes (BD Vacutainer®; BD Diagnostic, Milan, Italy) through cardiac puncture after the anesthesia. Plasma was separated by centrifugation at 10,000 g for 5 min. Samples were stored at −20°C until use for serotonin and prostaglandin E2 (PGE2) levels.
Cyclooxygenase-1 and cyclooxygenase-2 activity
To quantify the cyclooxygenase (COX) activity, the samples were tested following the protocol of a commercial kit (Abcam, UK; No. ab204699). In brief, tissue samples were mixed with a COX probe and COX factor before celecoxib or SC560 was added to measure COX-1 and COX-2 activities. An arachidonic acid solution was added to each mixture, and fluorescence was immediately measured in kinetic mode (15-sec interval, 30 min). The Bradford protein assay was used to measure the protein concentration of each sample.
The amount of resorufin in each sample was calculated using the standard curve. COX reactivity was calculated from the amount of resorufin per reaction time and the amount of protein in the sample. The degree of COX-1 and COX-2 activity is reported as pmol/min per mg or μU/mg, respectively.
PGE2 level
PGE2 levels represent biological actions, such as anti- and proinflammation, modulation of sleep/wake cycles, and vasodilation. To determine the PGE2 levels, serum samples were tested using a competitive enzyme-linked immunosorbent assay (ELISA) kit (Abcam; No. ab133021). In brief, the samples or standards were mixed well in a microtiter plate with alkaline phosphatase-conjugated PGE2. Next, an antibody specific to PEG2 was added, and the cells were incubated at room temperature (RT) for 2 h.
The ELISA plate was washed three times with washing buffer (provided with the kit). The p-nitrophenyl phosphate disodium salt (pNpp) substrate was added and incubated for 45 min before the stop solution was added. The absorbance was measured at 405 nm using a SpectraMax M5 microplate reader (Molecular Devices). PGE2 levels were calculated using a standard curve.
Serotonin level
Serum serotonin levels were measured in all samples according to the manufacturer's instructions using a competitive ELISA kit (Abcam; No. ab133053). In brief, the samples or standards were mixed with alkaline phosphatase-conjugated serotonin before adding a serotonin-specific antibody to each microtiter plate. The plates were then incubated at RT for 2 h on a shaker. Each well was then washed three times with the washing buffer. The pNpp substrate solution was then added to each well and incubated for 1 h without shaking. After incubation, the stop solution was added and the absorbance was measured at 405 nm using a microplate reader (SpectraMax M5 microplate reader; Molecular Devices). The serotonin levels were calculated using a standard curve.
Statistical analysis
Each group of studies included at least 10 mice and 8 rats. All data are represented as mean±SD or SEM. Variance analysis was performed using one-way ANOVA followed by Tukey's post hoc test for multiple comparisons. The p-value <0.05 was considered statistically significant. GraphPad Prism version 9 (GraphPad Software, San Diego, CA) was carried out for this study.
Results
Formalin and writhing test
To investigate the analgesic efficacy of topical CBD gel in this study, the formalin test and writhing test were performed in mice treated with either topical placebo gel, 1% diclofenac gel, 1% CBD gel, or a combination of 1% and 4% levomenthol gel (Fig. 1). The observations were separated into two parts for the formalin test: early and late phases (0–5 min and 15–30 min after formalin injection, respectively). In the early phase, 1% diclofenac gel, 1% CBD gel, and a combination of 4% levomenthol gel showed significantly reduced paw licking compared with the placebo gel (p<0.0001, p<0.0001, p<0.0001, respectively).
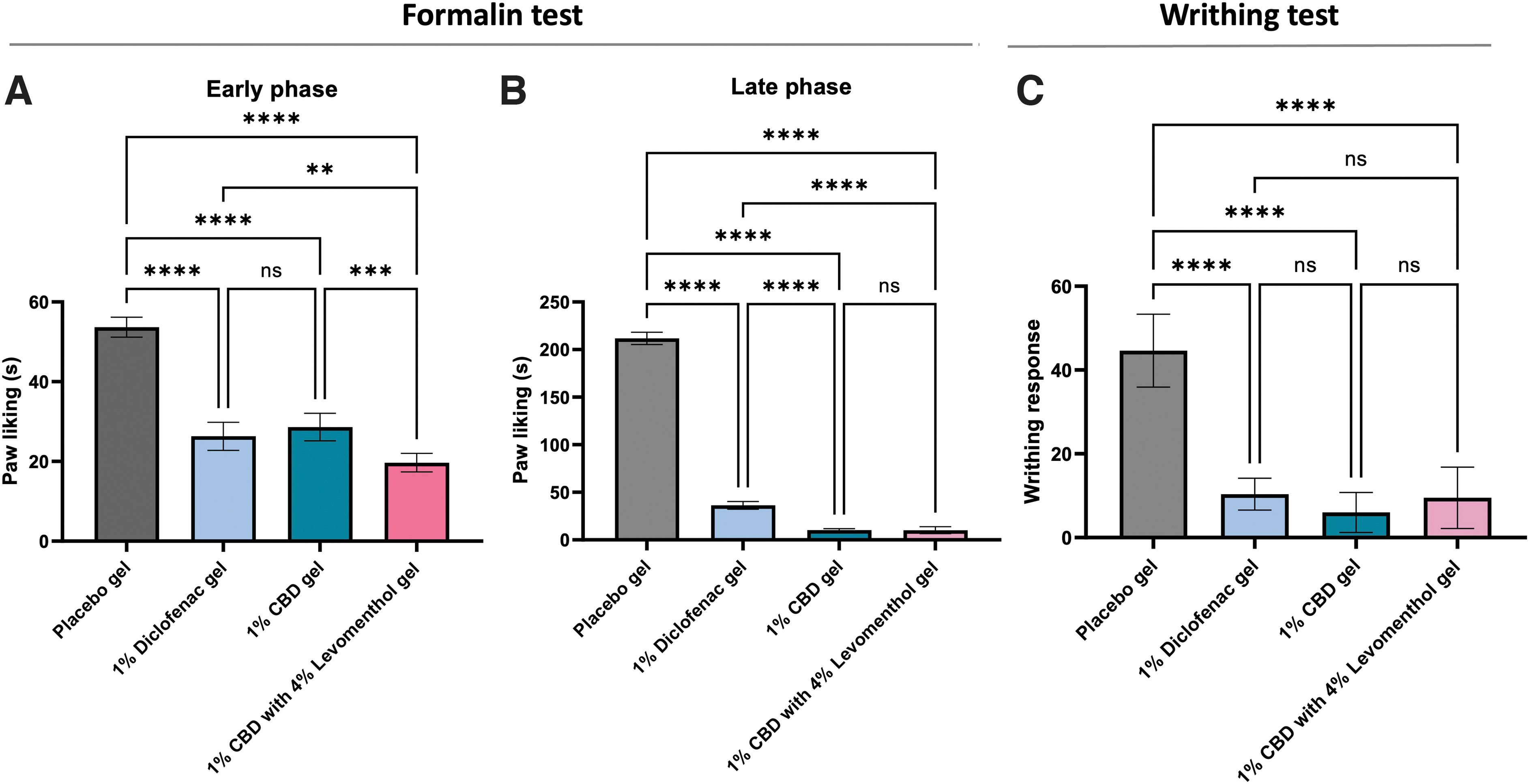
Comparison of the analgesic effect in different treated groups, including placebo gel, 1% diclofenac gel, 1% CBD gel alone, or in combination with 4% levomenthol gel. Paw licking after the 2.5% formalin injected at the dorsal surface of the right hind paw was compared in the early phase
The highest analgesic efficacy was found in the mice treated with the combination of 1% CBD and 4% levomenthol gel, compared with those mice treated with either 1% diclofenac or 1% CBD gel alone (p<0.01, and p<0.001, respectively) (Fig. 1A). In the late phase, paw licking in all treatment groups (1% diclofenac gel, 1% CBD gel, and the combination with 4% levomenthol gel) significantly decreased when compared with the placebo group (p<0.0001, p<0.0001, p<0.0001, respectively).
Interestingly, mice treated with either CBD gel or a combination with 4% levomenthol gel had significantly lower paw licking than the 1% diclofenac group (p<0.0001) (Fig. 1B). For the acetic acid-induced writhing testing, 1% diclofenac, 1% CBD, and the combination with 4% levomenthol have significantly reduced the writhing response compared with placebo gel (p<0.0001, p<0.0001, and p<0.0001, respectively) (Fig. 1C).
Carrageenan-induced edema
The anti-inflammatory effects of tropical CBD were investigated by measuring paw edema (Fig. 2). The percentage of paw edema in rats treated with 1% CBD was significantly lower than placebo and 1% diclofenac gel groups 1 h after the carrageenan administration (p<0.0001 and p<0.0001, respectively). Moreover, the anti-inflammatory effect of 1% CBD gel was observed from 1 to 4 h. In comparison, the anti-inflammatory effect onset of 1% diclofenac gel was observed after 2 h of inducing inflammation (Fig. 2A).
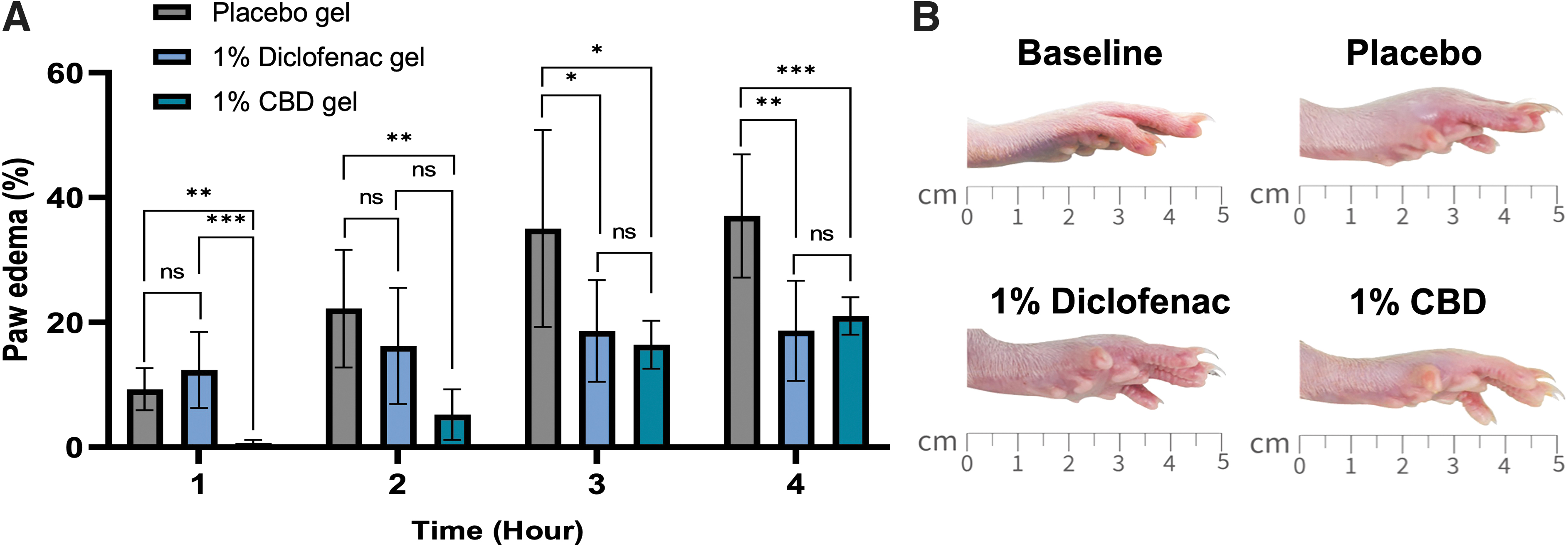
Anti-inflammatory effect of topical CBD on carrageenan-induced paw edema rats. The degree of paw edema in different treated groups (placebo gel, 1% diclofenac gel, and 1% CBD gel) was evaluated at 1, 2, 3, and 4 h after carrageenan-induced paw edema
Moreover, the physical appearance of paw edema at baseline compared with that at 4 h after carrageenan injection in the differently treated mice is shown in Figure 2B. The appearance showed that 1% CBD gel after 4 h of inflammatory induction reduced the severity of paw edema more than 1% diclofenac gel (Fig. 2B). This implied that 1% CBD had greater potential anti-inflammatory efficacy than 1% diclofenac.
Pathohistology analysis
Histological examination was performed to evaluate the site of carrageenan injection after 4 h. The site of carrageenan injection showed congestion of vessels and infiltration of inflammatory cells, such as lymphocytes, macrophages, and neutrophils, into the site of inflammation (Fig. 3A1–A6). The degree of inflammation was graded into three tiers as described in the “Materials and Methods” section. The results demonstrated that the degree of inflammation in paws treated with 1% CBD gel was significantly lower than placebo at 4 h after the carrageenan induction (p<0.05) (Fig. 3B).

Moreover, the highest inflammation was observed in the group treated with placebo gel. In contrast, the lowest inflammation was potentially seen in the group treated with 1% CBD gel, after paw edema result at 4 h after carrageenan injection. However, the degree of inflammation in the placebo and 1% diclofenac gel groups was insignificant in this experimental study.
COX-1 and COX-2 activity, PGE2, and serotonin levels
Inflammatory biomarkers, including COX-1 and COX-2 activity, PGE2, and serotonin levels, were evaluated in different treatment groups (placebo gel, 1% diclofenac gel, and 1% CBD gel) 4 h after inflammatory induction. COX-1 and COX-2 convert arachidonic acid into prostaglandins. In this study, COX-1 and COX-2 activities did not differ between diclofenac gel, CBD, and placebo groups (Fig. 4A, B). Indeed, PGE2 levels also correlated with COX-1 and COX-2 activities (Fig. 4C). However, the serotonin levels in 1% CBD and 1% diclofenac groups were significantly lower than those of the placebo group (p<0.01), whereas serotonin suppressing effects of the CBD and diclofenac groups were not different (Fig. 4D).

COX-1 and COX-2 activity, PGE2, and serotonin levels in the serum of different treated groups (placebo gel, 1% diclofenac gel, and 1% CBD gel) were evaluated at 4 h after the inflammatory induction. COX-1 and COX-2 activities were detected by enzymatic activity method
Discussion
In this study, the antinociceptive effects of topical CBD gels were investigated using formalin and writhing tests in mouse models. Both are robust models of nociception.25,26 The formalin test induced a noxious stimulus with 20 μL of 2.5% formalin in saline under the right hind paw. This study found that 1% CBD gel and 1% diclofenac gel effectively decreased nociceptive behavior in mice. Moreover, the treatment with 1% CBD combined with 4% levomenthol gel decreased nociceptive behavior. It showed high effectiveness when treated with 1% CBD and 1% diclofenac gel in the early phase (neurogenic pain: 0–5 min after induced inflammatory agent injection).
Furthermore, we demonstrated a synergistic antinociceptive response between 4% levomenthol and 1% CBD in the early phase. However, the late phase (inflammatory pain) did not differ with 1% CBD alone. Evaluating the true synergistic response of CBD and levomenthol in alleviating nociceptive behavior in the formalin test requires further analysis. Additional experiments should be conducted to assess the synergistic effect, such as dose–response studies with different combinations of CBD and levomenthol, and to compare the results with the expected additive effects based on individual agent responses.
These experiments clarified whether the combination produced a synergistic effect beyond that expected from the individual components. Levomenthol is an isomer of menthol that provides pain relief through its cooling effect and vasodilation, and may act as a weak sodium channel blocker. 27 The activity depends on neural channels with voltage synchronization, which results in weak and localized anesthetic effects.28,29 The concentration of levomenthol (<1%) depresses cutaneous nociception and may even desensitize nociceptive C-afferent fibers. 30 However, this agent did not exhibit anti-inflammatory activity as observed in the late phase.
Formalin-induced central sensitization is the most crucial aspect of the test for evaluating nociceptive behavior. 31 The subcutaneous injection of formalin produced distinct biphasic nociceptive and response nociceptive behaviors, such as intensive licking and biting of the injected paw. The early phase represents acute pain that immediately occurs (0–5 min) after formalin injection. Nociceptor mediators include substance P, glutamate, and bradykinin, and direct stimulation of the nociceptor occurs through the C fiber.21,31,32
The late phase (inflammatory pain: 20–30 min after injection) stimulates several inflammatory mediators, including prostaglandins, histamine, serotonin, bradykinin, nitric oxide, cytokines (tumor necrosis factor-alpha [TNF-α]), and substance P.33,34 Moreover, late-phase inflammatory mediators stimulate TRPV and TRPA, and probably stimulate downstream signaling pathways.35,36 A systematic review and meta-analysis revealed that various topical CBD treatments have significantly reduced inflammatory and pain models.37–39
The CBD also showed significantly decreased nociceptive behaviors with both results in neuropathic and inflammatory pain models.40,41 Moreover, pre-clinical and clinical studies have suggested that CBD is a promising antinociceptive and inflammatory agent for decreasing neuropathic and inflammatory pain.3,27,42–45
The acetic acid-induced writhing test is widely used to evaluate peripheral analgesic activity and visceral inflammatory pain. This model represents a nociceptive chemical test sensitive to nonsteroidal anti-inflammatory drugs. 46 Intraperitoneal injection of acetic acid increases the levels of inflammatory mediators. Prostaglandin biosynthesis importantly plays a role in the nociceptive mechanism. 47 Acetic acid increases the production of COX-1 and COX-2 (particularly PGE2) and lipoxygenase (LOX) in the peritoneal fluid. 48
Moreover, endogenous mediators, such as bradykinin, serotonin, histamine, and cytokines, are released and stimulated by peripheral nociceptive receptors and nociceptive reactions, which result in physiological effects, such as abdominal constrictions, pelvic rotation, and subsequent stretching of at least one hindlimb.46,47,49 A study in mice models also showed that CBD gel decreased nociceptive behavior and anti-inflammatory effect. Nociceptive behavior in these mice was pathologically similar to that observed in peritonitis. 50
However, not only CBD but also many other drugs (such as muscle relaxants, antihistamines, monoamine oxidase inhibitors, and adrenergic blockers) may inhibit the response to pain, thereby decreasing the writhing response. 50 The impact underlying this decrease in serotonin levels remains unclear. However, a possible explanation is that CBD acts as an agonist of the human serotonin 5-HT1a receptor, which functions through GTP-gamma S binding in the G protein-coupled receptor system. CBD binding resulted in the desensitization of 5-HT1a receptors and decreased levels of serotonin, especially in mice that underwent repeated CBD use. 51 Therefore, a formalin test is required to confirm positive results of the writhing test.
Carrageenan-induced inflammation is a common model for testing anti-inflammatory effects owing to its reliable and highly predictable dosage in inflammatory diseases. This is typically associated with the effective dose in humans. 52 The edema induction mechanically induces various inflammatory mediators, such as prostaglandins, histamine, bradykinin, LOXs, and other COX products (COX-1 and COX-2). 53 Moreover, at the site of inflammation, various cell types, including endothelial cells and leukocytes, produce potent reactive free radicals and nitric oxide products at the sites of inflammation. 43
Owing to carrageenan-induced paw edema, the inflammatory response is time dependent and has biphasic phases with various mediators.54,55 The first phase immediately occurred until 2 h after carrageenan injection, whereas the second phase occurs 3–4 h after carrageenan injection. The response in this first phase is increased vascular permeability and the release of proinflammatory chemical mediators.55–59 The response during the first phase is associated with leukocyte infiltration and the production of inflammatory mediators, such as PGE2, leukotrienes, kinin, platelet-activating factor, proinflammatory cytokines, and free radicals of oxygen derivatives.60–62
This study demonstrated that topical 1% CBD gel could rapidly inhibit paw edema for 1 h. It maintained its inhibitory effect until 4 h, which was concordant with a literature review that summarized the potential analgesic and anti-inflammatory effects of topical CBD in animal models. 63 CBD contributes to various anti-inflammatory mechanisms and stimulates immune cell functions, including the suppression of proinflammatory cytokines, such as TNF-α, growth factors, IL-1 beta (IL-1β), and chemokines, as well as the inhibition of immune cell activation, migration, proliferation, maturation, and antigen presentation.64–66
Although the mechanism of action of topical CBD is not fully understood, it may be an alternative treatment for analgesic and anti-inflammatory conditions.67,68 However, pathohistological assessment of the right hind paw probably supported the hypothesis of the anti-inflammatory effect of 1% CBD gel. This study revealed that 1% CBD gel could help reduce inflammation and infiltration of inflammatory cells, such as macrophages, neutrophils, and lymphocytes into the site of inflammation. Taken together, topical CBD could have analgesic and anti-inflammatory effects in animal models, which this study represents and may play a potential role in the clinical setting.
Conclusion
In summary, the topical administration of 1% CBD gel has the potential for analgesic and anti-inflammatory activities in an animal model. However, the mechanism of action of topical CBD is not completely understood. The topical administration of 1% CBD gel may be an effective candidate for an anti-inflammatory agent. Further safety and efficacy investigations on topical CBD in clinical settings are required.
Footnotes
Acknowledgments
This research could not have been completed without the assistance of many people. The authors thank a senior pathologist Professor Vorachai Sirikulchayanonta, MD, Faculty of Science, Rangsit University, Pathum Thani, Thailand, for his advice and guidance regarding this study.
Author Disclosure Statement
The authors have no conflict of interest to declare.
Funding Information
This study was supported by the Thammasat Postdoctoral Fellowship, Faculty of Medicine, and the Center of Excellence in Stroke, Thammasat University, Thailand (Funding number TUPD2/2564).