
Abstract
To evaluate the anticaries and antigingivitis properties of cannabinoid-containing oral health products. A systematic research strategy was employed. Specific search terms were used, including “Cannabinoids AND dental caries,” “Cannabinoids AND oral health,” “Cannabinoids AND dental plaque,” “Cannabinoids AND gingivitis AND periodontitis,” “Cannabinoids AND S. mutans,” “Cannabidiol AND oral health,” and “Cannabidiol AND oral biofilm.” The search was conducted in PubMed, Cochrane, and EBSCO Host databases. The search yielded a total of 73 articles, out of which 15 articles (20.5%) were relevant to the scope of this systematic review. Among the relevant articles, only eight (10.9%) directly addressed the research question. The findings from these articles suggest that cannabinoids have the potential to reduce the metabolism of cariogenic bacteria, specifically Streptococcus mutans, and decrease the number of bacterial colonies in dental plaque. In vitro studies also demonstrated a significant inhibitory effect of cannabinoids on oral biofilms and create a considerable inhibitory zone of growth when investigated on oral biofilms in vitro. Furthermore, CBD exhibited antibacterial properties against Porphyromonas gingivalis, a primary pathogen associated with periodontal disease. The current review shows insufficient data to conclude on the anticaries and antigingivitis effects of cannabinoids. Despite extensive research on their systemic therapeutic benefits, their oral health impact remains underexplored, lacking clinical trials and primary research.
Introduction
Dental caries and periodontal disease are prevalent yet preventable oral diseases. These conditions significantly impact global health, affecting all age groups. They cause discomfort, lower life quality, strain finances, affect work or school attendance, and induce emotional stress. 1 According to the Global Burden of Disease study, ∼3.5 billion people worldwide suffer from oral diseases, 1 with severe periodontal issues affecting 14% of adults worldwide. 2
Tooth decay or dental caries is a dental biofilm-induced disease that causes mineral loss in teeth, and depends on environmental, behavioral, and dietary factors. Its prevention and treatment are global concerns, multifaceted, requiring interventions. 3
Periodontal disease, a chronic biofilm-driven inflammatory disease, if not prevented or treated leads to progressive destruction of periodontal support around the tooth. Emerging evidence indicates it may also influence other chronic diseases like rheumatoid arthritis and Alzheimer's. 4 More than 1 in 10 adults may be affected by severe periodontitis, making it the 11th most prevalent disease globally, more prevalent than cardiovascular disease. 5
Oral disease prevention strategies vary, from professional treatments like topical application of sodium fluoride and sealants to over-the-counter products like fluoride toothpaste, xylitol gum, or mouthwashes containing essential oils.6–8 Individual compliance with home care and managing risk factors like smoking are also crucial. 7
Cannabis sativa has a complex history and varying medicinal and psychoactive roles. 8 Although the terms, cannabis, hemp, or marijuana, have been used interchangeably, they contain significant pharmacologic differences. The therapeutic effects of cannabinoids are dependent on their bioavailability. For decades, research on CBD has focused on its biochemical, medicinal, and pharmaceutical aspects, including its pharmacokinetics and pharmacodynamics. 9
Discovery of human endocannabinoid system (ECS) has led to interest in the medicinal properties of cannabinoids in recent years. Considering the amount of research on medicinal properties of herbal and natural remedies, in-depth research is lacking in dentistry.
The endogenous cannabinoids, or ECS is a vital neuromodulatory system that plays a crucial role in the development of the central nervous system (CNS) and various other functions related to the nervous system. 10 The ECS includes the endogenous cannabinoids (lipid neurotransmitters), enzymes responsible for production and decomposition of cannabinoids, as well as the cannabinoid receptors. 10
The cannabinoid receptors that are most widely distributed throughout the body include CB1 and CB2 cannabinoid receptors that belong to a bigger family of G-protein-coupled receptors (GPCRs), characterized by seven transmembrane domains and coupled to G-proteins, notably to Gi/Go proteins.9,10 These receptors are known to bind to other receptors such as transient receptor potential (TRP) channels, and peroxisome proliferator-activated receptors (PPARs). 10 Anandamide (AEA) and 2-arachidonoyl glycerol (2-AG) are the most distinguished endocannabinoid, are most effective agonists for cannabinoid receptor type 1 (CB1R), and cannabinoid receptor type 2 (CB2R).9,10 The wide distribution of CB1 and CB2 within the tissue contributes to the psychotropic effects of THC. 10
Endocannabinoids play a key role in regulating homeostatic functions. Increased cellular levels of endogenous ligand binding to CB1R named arachidonoyl ethanol amide (AEA), after periodontal surgery promotes healing by increasing the gingival fibroblast production. 11
The purpose of this review is to investigate whether the use of cannabinoid-containing oral health products has any oral health benefits by reducing risk of dental caries and periodontal disease. In this study, we focused to answer the following questions: How does current research support the anticaries effects of cannabinoids? Is there any evidence supporting the antigingivitis effect of cannabinoids?
Methods
This systematic review seeks to evaluate the scientific evidence on whether cannabinoid-containing oral health products reduce the risk of dental caries and periodontal disease. Our research question was built using the PICO framework. 12 The question was formulated as follows: In patients with dental caries and periodontal disease, does using cannabinoid-containing oral health products compared with conventional oral health products reduce the risk of dental caries? This resulted in a PICOS analysis as follows: Population: Patients with dental caries and periodontal disease; Intervention: Using cannabinoid-containing oral health products; Comparison: Conventional oral health products; Outcome: Reduce the risk of dental caries; Study Design: review.
This review is part of a PhD study approved by the IRB at the West Coast University.
The primary investigator conducted an initial literature search in May 2022 using PubMed, EBSCO, and Cochrane Database, employing various keyword combinations. The search in PubMed included the following terms: (cannabinoids AND “dental plaque” OR “ oral disease”), (Cannabidiol OR dental plaque), (Cannabidiol AND “oral health”) (cannabinoid AND “p. gingivalis”), (cannabinoid AND “ dental plaque” AND “ dental caries”), (cannabinoids AND “gum disease”), (Cannabinoids AND “gingivitis” AND “periodontitis”), (Cannabinoids AND s. mutans), and (Cannabinoids AND “biofilm”).
The eligibility criteria in this search engine were studies that investigate the effects of cannabinoids on dental plaque, oral diseases, dental caries, gum disease, gingivitis, periodontitis, Streptococcus mutans, and biofilm. Pilot studies and clinical trials investigating the anticaries and anti-inflammatory effects of cannabinoids, as well as their oral health benefits, were included. Articles not specifically addressing the oral health benefits of cannabinoids, focusing instead on overall health benefits, in vivo animal studies, or synthetic cannabinoids, were excluded.
The advance search in the EBSCO host was made limited to peer-reviewed publications and keywords (AND Cannabinoids AllFields AND dental plaque AllFields). The eligibility criteria for this search engine included peer-reviewed publications that discuss cannabinoids and dental plaque. For the Cochrane Database of Systematic Reviews, the terms included “Cannabinoids” AND “oral health,” “Cannabinoids” AND “dental plaque.” For this specific database, the eligibility criteria were systematic reviews that cover the topic of cannabinoids and their impact on oral health and dental plaque. These sources (PubMed, EBSCOhost (Dentistry & Oral Sciences Source and the Cochrane Database of Systematic Reviews), were utilized to gather evidence on the effects of cannabinoids on dental plaque, oral diseases, dental caries, gum disease, gingivitis, periodontitis, S. mutans, and biofilm. The eligibility criteria for each database were specified to filter and identify relevant articles.
The search was carried out by a single reviewer (J.T.) who assessed the relevance of the search results based on their titles and abstracts. Following the removal of duplicates, blinded pairs of researchers (J.T. and H.L.) evaluated the abstracts of the selected articles using the Rayyan web application. 13 This web tool aided in screening and data extraction for selected articles, capturing study features, participant details, intervention types, and results. It revealed a limited number of studies focusing on the antigingivitis and anticaries benefits of cannabinoids.
The following search terms and fields search words (cannabinoids AND “oral health”), resulted in the discovery of 25 resources, of which 2 pertained to the premise of this review. The (Cannabinoids AND “dental plaque”) query yielded four sources all relevant to this systematic review. Cannabinoids AND “gingivitis” AND “periodontitis” search in PubMed, yielded 5 studies in which none was found relevant to the goals of the current systematic review. The remainder of PubMed searches produced overlapping results (Table 1). Cochrane's search of the keywords produced one article. Boolean search in Source EBSCO host utilizing (Cannabinoid AND oral health) keywords in Dentistry & Oral Sciences database generated 15 articles, in which 2 were utilized for this review (Fig. 1), excluding duplicate articles.
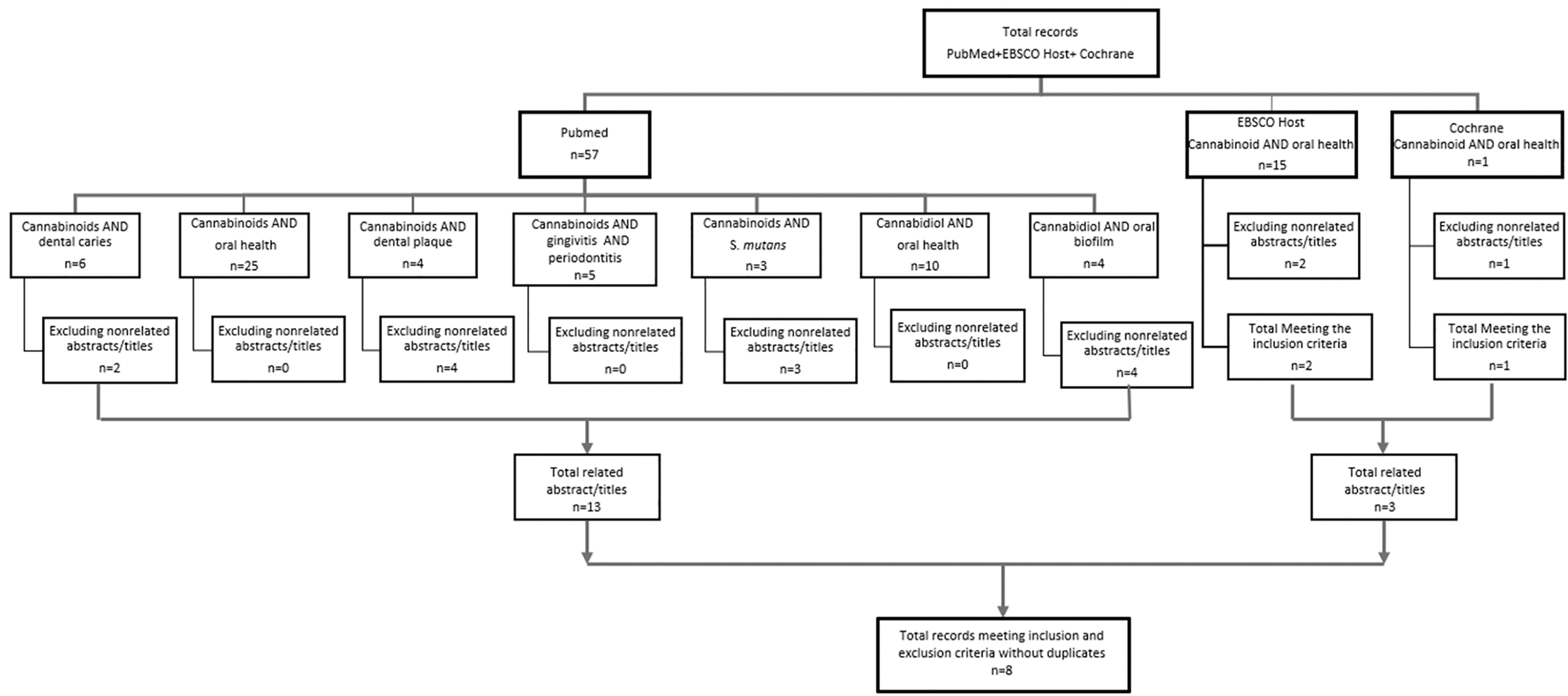
Flow chart depicting the search strategy following PRISMA, n. PRISMA, Preferred Reporting Items for Systematic Reviews or Meta-Analysis.
Detailed Example of Search Results in PubMed
Results
Selected articles, all from Belgium and Israel, included in vitro studies and clinical trials on cannabinoids like CBD and cannabigerol (CBG) in oral care products. These studies appeared in seven different journals. The keywords used in the study (Fig. 2) totalize 26 terms, with the most used being “Streptococcus mutans” (n=4) followed by CBD and Cannabinoid with 3 mentions each.

World cloud of keywords.
In a zone of inhibition (ZOI) laboratory study conducted by Stahl and Vasudevan, 13 the antibacterial effect of CBD oil was compared with the chlorhexidine gluconate. The study evaluated the bactericidal efficacy of CBD and CBG mouthwashes (containing <1% cannabinoids) on the oral biofilm of 72 adults 18–83 years of age. The results showed these mouthwashes had a ZOI comparable to the gold standard, chlorhexidine 0.2% (CHX 0.2%). CBD mouthwash produced a statistically significant ZOI, and CBG mouth wash with nearly significant ZOI indicates that the bactericidal properties of the Cannabinoid-containing mouthwash are comparable to the gold standard. Limitations include the in vitro design, which may not fully represent oral complexities or systemic cannabinoid effects, and potential bias in comparing CBD to CHX 0.2%.
An in vitro study examined CBG's antibacterial effects on S. mutans a bacteria linked to dental caries. The study found that CBG inhibits the growth of S. mutans. 14 Researchers found that CBG disrupts the S. mutans’ cell membrane, increasing permeability and decreasing metabolic activity. CBG treatment also inhibited the bacteria's pH-lowering effect and showed bacteriostatic and bactericidal properties at concentrations of 2.5 and 5–10 μg/mL, respectively. 14 This study's potential bias is its sole focus on CBG's antibacterial effects on S. mutans, neglecting possible adverse effects, other bacterial strains, or long-term oral health impact.
In an in vitro study conducted by Barak et al., the minimum inhibitor concentration (MIC) of CBD against planktonic S. mutans and its inhibitory properties against biofilm formation (MIBC) were measured. 15 The study found that 5 μg/mL CBD significantly reduced S. mutans’ biofilm, metabolic activity, and growth. Bacteria cultured on BHI agar with 5 μg/mL CBD showed inhibited growth after 24 h, indicating its bacteriostatic effect. CBD at concentrations of 5 μg/mL and 10 μg/mL not only restricted bacterial growth but also maintained a neutral pH of 7.2–7.3 during incubation. 15 The results of this study suggest the presence of bacteriostatic and anticaries properties of CBD.
Avraham et al.'s 2023 study investigated the combined antibacterial and antibiofilm effects of CBD and triclosan against S. mutans. The study examined varying concentrations of these compounds on biofilm formation after 24 h of incubation. 16 It was discovered that 2.5 μg/mL CBD when combined with 5 μg/mL triclosan leads to an additive antibacterial and antibiofilm formation effect, with a lower MIC for each agent alone at 5 μg/mL CBD and 10 μg/mL triclosan. 16
Vasudevan and Stahl discovered the superior efficacy of CBD-supplemented air powder polishing in reducing oral biofilm and its antibacterial and substantivity properties compared with the standard powder polishing agent. 17 Oral biofilm from 12 subjects were collected for the study. Six got standard polishing; six had added 1% CBD. In vitro results showed CBD significantly cut colony forming units (CFU) and hindered certain bacteria. It suggests that CBD may block new biofilm but may be biased for not including other polishing agents.
A clinical trial compared the antibacterial effects of cannabinoids and commercial oral care products on dental plaque in 60 adults. Cannabinoids, such as CBD, CBC, CBN, CBG, and CBGA, outperformed Oral B and Colgate in reducing bacterial colonies, as measured by CFU counts. 18 The fact that this study compares the antibacterial effects of cannabinoids with specific commercial products may introduce bias as there are many other oral care products available on the market that were not included in the comparison. The summary of the studies is presented in Table 2.
Characteristics of the Selected Articles
CBG, cannabigerol.
Discussion
This systematic review revealed limited primary research on oral health benefits of CBD, as well as anticaries and antigingivitis benefits of this compound. The inclusion criteria of this systematic review limited the addition of primary research and clinical trials utilizing the synthetic CBD compounds, and in vivo animal studies. Despite the limited primary research on anticaries and anti-inflammatory effects of cannabinoids, there is a newfound presence of review of literature on health benefits of CBD in dentistry. 19
In a recent review of literature, the potential health benefits of hemp or cannabis products on health parameters, oral health, and possible drug interactions were discussed in detail.20,21 To better understand the possible attributes of cannabis, the authors largely focused on human ECS. The study found that phytocannabinoids like CBD, THC, and CBG effectively alleviate oral pain and inflammation as adjunctive therapy. These compounds boost anti-inflammatory cytokine IL-10 production while suppressing proinflammatory cytokines.
Inflammation and pain arise from injury or infection, sharing common pathways across different conditions like diabetes and arthritis. Research indicates that proinflammatory triggers activate anti-inflammatory endocannabinoids affecting CB2 receptors. 22
The review analyzes existing evidence on CBDs' anti-inflammatory and antibacterial effects for treating gingivitis. Generally, gingivitis and periodontitis stem from oral microbial imbalance and the body's inflammatory response through proinflammatory mediators. 23
Periodontal disease, characterized as a chronic inflammatory condition, stands as the primary cause of tooth loss in adults. Porphyromonas gingivalis is an oral pathogen proven to be a major contributor to the breakdown of periodontal tissue. 24 Nakajima et al. discovered that AEA existing in gingival crevicular fluid reduces the production of proinflammatory mediators induced by P. gingivalis Lipopolysaccharide, thus could regulate the inflammatory process in the periodontal tissue. 25
Researchers inferred that CBD induces suppression of proinflammatory mediator production caused by invasion of the periodontal cells by P. gingivalis. Current research suggests that CBDs can potentially “promote the regeneration of the periodontal connective tissue.” 26
In their literature review, Lowe et al. propose that the anti-inflammatory properties of cannabinoids, such as THC and CBD, CBC and CBG could offer potential benefits in treating disease. 27 Given the role of inflammatory mediators in periodontal disease, this research suggests that cannabinoids could potentially slow its progression.
The anti-inflammatory and oral health benefits of cannabinoids are discussed in depth by Klein et al. The results of in vivo studies strongly support the modulatory effect of CBD on the proinflammatory mediator secretion, neutrophil proliferation, and chemotaxis, which directly influence treatment modalities of periodontal disease. 28
Qi et al.'s 2022 rodent study explored CBD's effect on oral ulcer healing. Acid-induced ulcers were treated topically with varying CBD concentrations. Results showed faster healing, reduced inflammation, and increased mucosal thickness. CBD also lowered proinflammatory cytokines, such as IL-1β while boosting keratinocyte production, speeding up wound recovery. 29 These findings suggest that CBD has the potential to aid in the healing of oral ulcers in humans caused by a range of conditions such as trauma, cancer, and radiation therapy.
Candida albicans, a virulent fungal pathogen, is known for its opportunistic behavior and ability to invade various types of human tissue, often leading to both oral mucosal and systemic infections in individuals with compromised immune system. 30 The virulency of C. albicans is greatly influenced by the formation and dispersion of oral biofilm. In a laboratory study, the antifungal effect of CBD and triclosan through a sustained release varnish (SRV), was measured. 31
In an ex vivo study, CBD-SRV and triclosan–SRV both effectively reduced C. albicans biofilm and changed its structure. The combined CBD–triclosan–SRV solution not only inhibited biofilm but also had a 14-day sustained release. 32
Conclusion
The incorporation of cannabinoids in oral health products seems to be effective in reducing disease-causing bacteria. There is a notable lack of research and clinical trials on the oral health benefits of cannabinoids. Further research and clinical trials are necessary to explore the oral health benefits of cannabinoids in depth and establish evidence-based guidelines for their utilization in oral health care.
Footnotes
Authors' Contributions
J.T. took the lead role in developing the protocol for the review, conducting the research of articles in the databases, analyzing the data, and writing the original draft of the article. H.L. and M.H. played supporting roles in the development of the review design, assisting in the analysis of articles sourced from database searches, and contributing to the writing of the article. All three authors actively participated in writing, reviewing, and reading the final article before submission.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.