
Abstract
Introduction:
Liver cirrhosis is a condition characterized by the gradual replacement of normal liver tissue with scar tissue, ultimately leading to liver failure. This slow and progressive disease begins with a chronic inflammatory process induced by a noxious agent. In its advanced stages, the disease lacks effective therapies. Research has demonstrated the significant involvement of the endocannabinoid system in the pathogenesis of this disease. This study evaluated the hepatoprotective effect of cannabidiol (CBD) in the progression of experimental hepatic cirrhosis induced by thioacetamide (TAA) in rats.
Methods:
A randomized experimental design was employed using Holtzman rats. Hepatic cirrhosis was induced by intraperitoneal administration of TAA at a dose of 150 mg/kg for 6 weeks, with treatment initiated additionally. The groups were as follows: Group 1: TAA + vehicle; Group 2: TAA + CBD 2 mg/kg; Group 3: TAA + CBD 9 mg/kg; Group 4: TAA + CBD 18 mg/kg; Group 5: TAA + silymarin 50 mg/kg; and Group 6: Healthy control. Serum biochemical analysis (total bilirubin, direct bilirubin, ALT, AST, alkaline phosphatase, and albumin) and hepatic histopathological study were performed. The Knodell histological activity index (HAI) was determined, considering periportal necrosis, intralobular degeneration, portal inflammation, fibrosis, and focal necrosis.
Results:
All groups receiving TAA exhibited an elevation in AST levels; however, only those treated with CBD at doses of 2 mg/kg and 18 mg/kg did not experience significant changes compared to their baseline values (152.8 and 135.7 IU/L, respectively). Moreover, ALT levels in animals treated with CBD showed no significant variation compared to baseline. The HAI of hepatic tissue was notably lower in animals treated with CBD at doses of 9 and 18 mg/kg, scoring 3.0 and 3.25, respectively, in contrast to the TAA + vehicle group, which recorded a score of 7.00. Animals treated with CBD at 18 mg/kg showed a reduced degree of fibrosis and necrosis compared to those receiving TAA alone (p ≤ 0.05).
Conclusion:
Our findings demonstrate that cannabidiol exerts a hepatoprotective effect in the development of experimental hepatic cirrhosis induced in rats.
Introduction
The progression of hepatic fibrosis is a critical process in the transition to hepatic cirrhosis, characterized by a sequence of pathological events that begin with inflammation of the endothelial intima, followed by stasis in the central veins and hepatic sinusoids. These processes trigger apoptosis, atrophy, and nodular regenerative hyperplasia, ultimately leading to hepatic fibrosis. Cirrhosis, in turn, is associated with significant complications that increase morbidity and mortality, such as ascites, hepatorenal syndrome, esophageal varices, hepatic encephalopathy, spontaneous bacterial peritonitis, and hepatocellular carcinoma.1,2
Unfortunately, the feasibility of implementing preventive therapies targeting the etiology of cirrhosis remains limited, prompting a continuous exploration of novel therapeutic targets. Despite various strategies aimed at slowing or reversing the fibrotic process, finding an effective therapeutic target continues to be challenging. The causative factors have been attributed to toxicity from alcohol consumption, as well as nutritional and metabolic influences. 3
In this context, high expression of CB1 receptors has been observed in human cirrhotic cells and hepatic fibrogenic cells. Research indicates that treatment with CB1 receptor antagonists reduces scarring in acute hepatic injuries and slows the progression of fibrosis in chronic liver injury models, suggesting a protective role for CB1 antagonists. 4 Moreover, in an experimental model of acute hepatitis induced by carbon tetrachloride (CCl-4), the absence of CB2 receptors was associated with accelerated liver injury, increased liver enzymes, hepatocyte apoptosis, and delayed liver tissue regeneration. Conversely, treatment with CB2 receptor agonists resulted in reduced liver injury and accelerated tissue regeneration. 5
A systematic review that included nine studies aimed at evaluating the influence of Cannabis sativa on the prevalence and progression of hepatic fibrosis in patients with chronic liver disease yielded controversial results. The review concluded that cannabis consumption does not increase the prevalence or progression of hepatic fibrosis in patients co-infected with hepatitis C virus. Contrarily, it revealed a marginal reduction in prevalence. 6
These findings have motivated further research to assess the hepatoprotective effect of cannabidiol (CBD). Consequently, this study aims to demonstrate the hepatoprotective effect of CBD in the progression of experimental hepatic cirrhosis in rats.
Materials and Methods
Animals
Male Holtzman rats (350–380 g) were procured from the National Institute of Health (NIH, Lima). They were housed in the Bioterium of the Faculty of Medicine at the Universidad Nacional Mayor de San Marcos-UNMSM and maintained under a 12-h light/12-h dark cycle in temperature- and humidity-controlled conditions. The rats had ad libitum access to food and water. All experimental procedures were performed according to the ethical principles outlined in the National Institutes of Health’s Guide for the Care and Use of Laboratory Animals. 7 The ethical aspects of the protocol were evaluated and approved by the ethics committee of the Faculty of Pharmacy and Biochemistry-UNMSM, Lima, Peru (approval number: 008-CE/UDI-FFB-19).
Experimental model of hepatic cirrhosis induction
Cirrhosis was induced by thioacetamide (TAA) from Sigma Chemical Co (St. Louis, MO, USA), diluted in 0.9% saline and administered at a dose of 150 mg/kg intraperitoneally twice a week for a period of 6 weeks. The control group animals received the same volume of 0.9% saline. 8
Treatment groups
A processed product of Cannabis sativa, in the form of tetrahydrocannabinol-free CBD tincture 500 mg/oz, manufactured by SClabs-USA, was utilized. It contains 17.9 mg/ml (1.79%) of CBD, as per the certificate of analysis.
The animals were randomly assigned to treatment groups and received daily treatments for a duration of 6 weeks, after the model was established. The groups were delineated as follows: Group 1 (n = 6): TAA + saline 2 mL/kg, Group 2 (n = 6): TAA + CBD 2 mg/kg, Group 3 (n = 6): TAA + CBD 9 mg/kg, Group 4 (n = 6): TAA +CBD 18 mg/kg, Group 5 (n = 6): TAA + Silymarin 50 mg/kg, and Group 6 (n = 6): Saline. Both CBD and silymarin were administered orally in a volume of 2 mL/kg. The experimenters were blinded to all treatment conditions.
Body weight recording
The body weight of the animals was systematically documented at the initiation of the study and then biweekly until its culmination.
Biochemical analysis of serum markers of hepatic function
At both the initiation and conclusion of the experiment, animals were intraperitoneally anesthetized with 75 mg/kg ketamine. 9 Blood samples (3 mL) were collected intracardially, and hepatic function profiles were assessed, including total bilirubin (TB), direct bilirubin (DB), total proteins, albumin, glutamic-oxaloacetic transaminase, glutamic-pyruvic transaminase, and alkaline phosphatase (ALP). All markers were evaluated using a semiautomated spectrophotometry analyzer (Emperor, Model EMP-168) and commercially available detection kits (Wiener Lab, Argentina) after the manufacturer’s instructions.
Histological analysis
At the end of the experiment, euthanasia was conducted for all animals. Liver dissection, fixation in 10% buffered formalin, embedding in paraffin, and sectioning into 5 µm sections were carried out. Staining procedures included hematoxylin and eosin (H&E) as well as Masson’s trichrome. The Knodell histological activity index (HAI) was employed for the numerical scoring of liver biopsy samples, considering parameters such as periportal necrosis, intralobular degeneration, portal inflammation, fibrosis, focal necrosis, ductal proliferation, apoptosis, and cholangitis (Table 1).10–11
Histological Activity Index for Numerical Scoring of Liver Biopsy Samplesa
The histological activity index score is the combined score of necrosis, inflammation, and fibrosis.
Statistical analysis
Results were expressed as mean ± standard deviation (SD). Significant differences between treatment groups were determined using one-way analysis of variance (ANOVA), followed by the Tukey test for multiple comparisons. Pairwise comparisons were conducted using the t-Student test. A p-value < 0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics 27.0 software.
Results
Effect on body weight
All subjects administered with TAA experienced a decrease in body weight at the end of the experiment. In the analysis of weight loss compared to the healthy control group, which only received the vehicle, animals treated with CBD at 18 mg/kg demonstrated no statistically significant difference, registering a weight loss of 8.0 g (p = 0.401). Conversely, groups treated with CBD at doses of 2 and 9 mg/kg, as well as the silymarin-treated group, experienced significant weight loss compared with the healthy group. No mortality was observed during the entire duration of the study.
Effect on biochemical markers of liver function
A significant increase in direct bilirubin levels was observed in rats treated with CBD at 9 mg/kg, reaching 0.25 ± 0.06 mg/dL. The group receiving CBD at 2 mg/kg recorded significantly higher alkaline phosphatase levels, exceeding all other groups, with a value of 468.11 ± 6.39 U/L. It is important to note that other biochemical parameters described in the table remained within similar ranges across all studied groups (Table 2).
Biochemical Analysis of Liver Function Parameters in Animals with Induced Cirrhosis Treated with Cannabidiol
p < 0.05. ANOVA test. Compared to TAA + Vehicle group.
DB, direct bilirubin; TB, total bilirubin; ALP, alkaline phosphatase.
In the comparison of AST levels at the initiation and conclusion of the treatment, an increase was observed in all TAA-receiving groups. Remarkably, only the groups treated with CBD at 2 and 18 mg/kg demonstrated no significant modification compared to baseline values, registering 152.8 ± 15.2 and 135.7 ± 10.4U/L, respectively (p < 0.05) (Fig. 1).

Determination of baseline AST/ALT to week 6 of the treatment with cannabidiol.
ALT levels remained unchanged in relation to their baseline values in all groups, except for the TAA + vehicle group, where a significant increase was observed, reaching up to 95.6 ± 7.4 U/L (p < 0.05) (Fig. 1).
Histopathological analysis of liver tissue
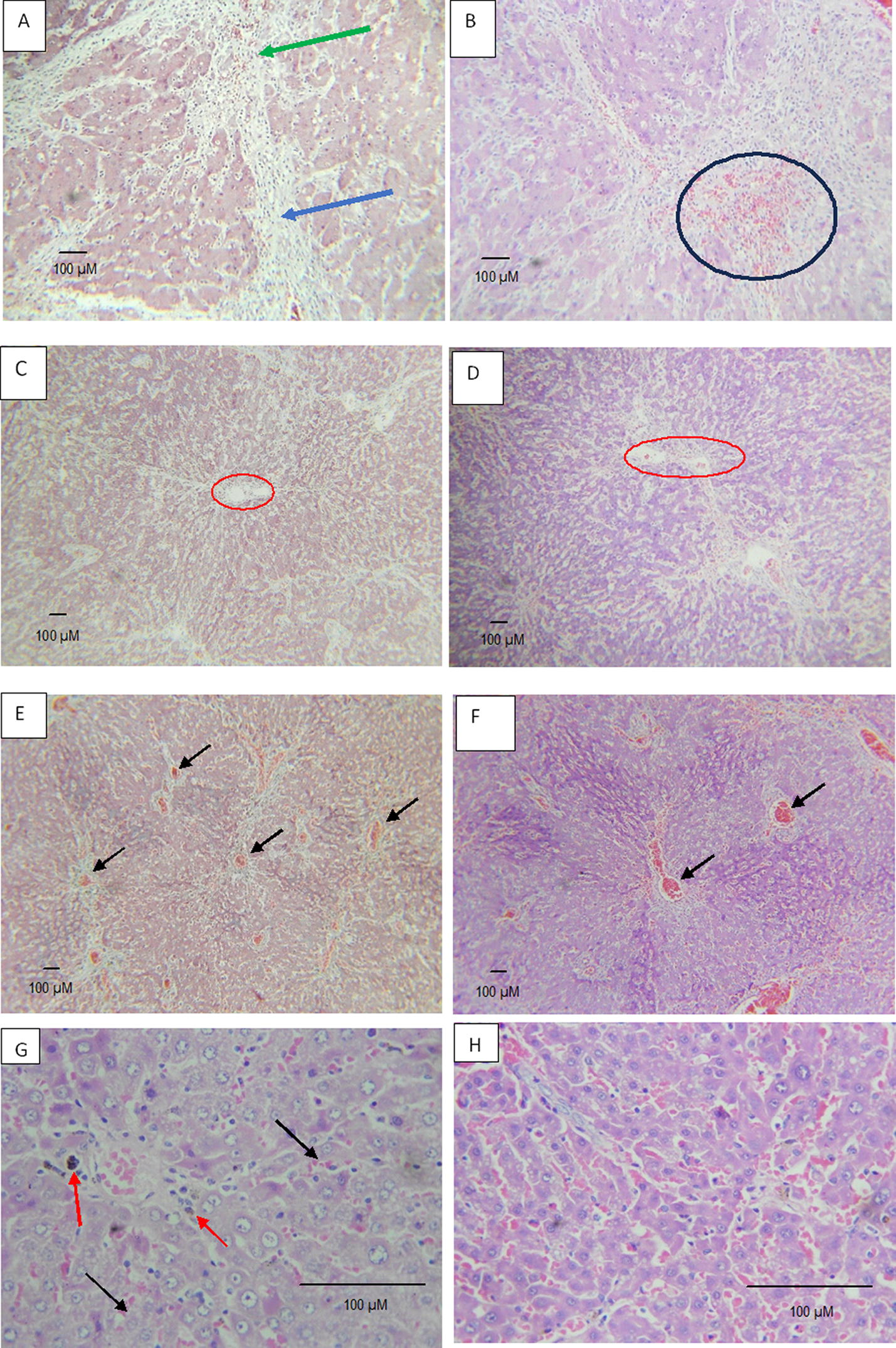
Animals treated with TAA + vehicle developed severe cirrhosis with erythrocytes in the portal space, increased bile ducts in the portal space, and the formation of fibrosis islands. Rats treated with CBD 9 mg/kg and 18 mg/kg exhibited a lower degree of periportal necrosis compared with those receiving only TAA (p ≤ 0.05). Only the group treated with CBD at 9 mg/kg exhibited a decrease in the degree of intralobular degeneration, slight damage to the portal space, a mild increase in bile ducts, and deposits of macrophages with bile pigment. In contrast, rats treated with CBD at 18 mg/kg showed a reduction in periportal inflammation; however, this difference was not statistically significant. Animals receiving CBD at doses of 2 mg/kg and 18 mg/kg showed a lower degree of fibrosis and necrosis. Tissues treated with silymarin exhibited bridge formation, macrophages in portal spaces, and mild congestion, as well as periportal damage due to increased bile ducts (Fig. 2 and 3).
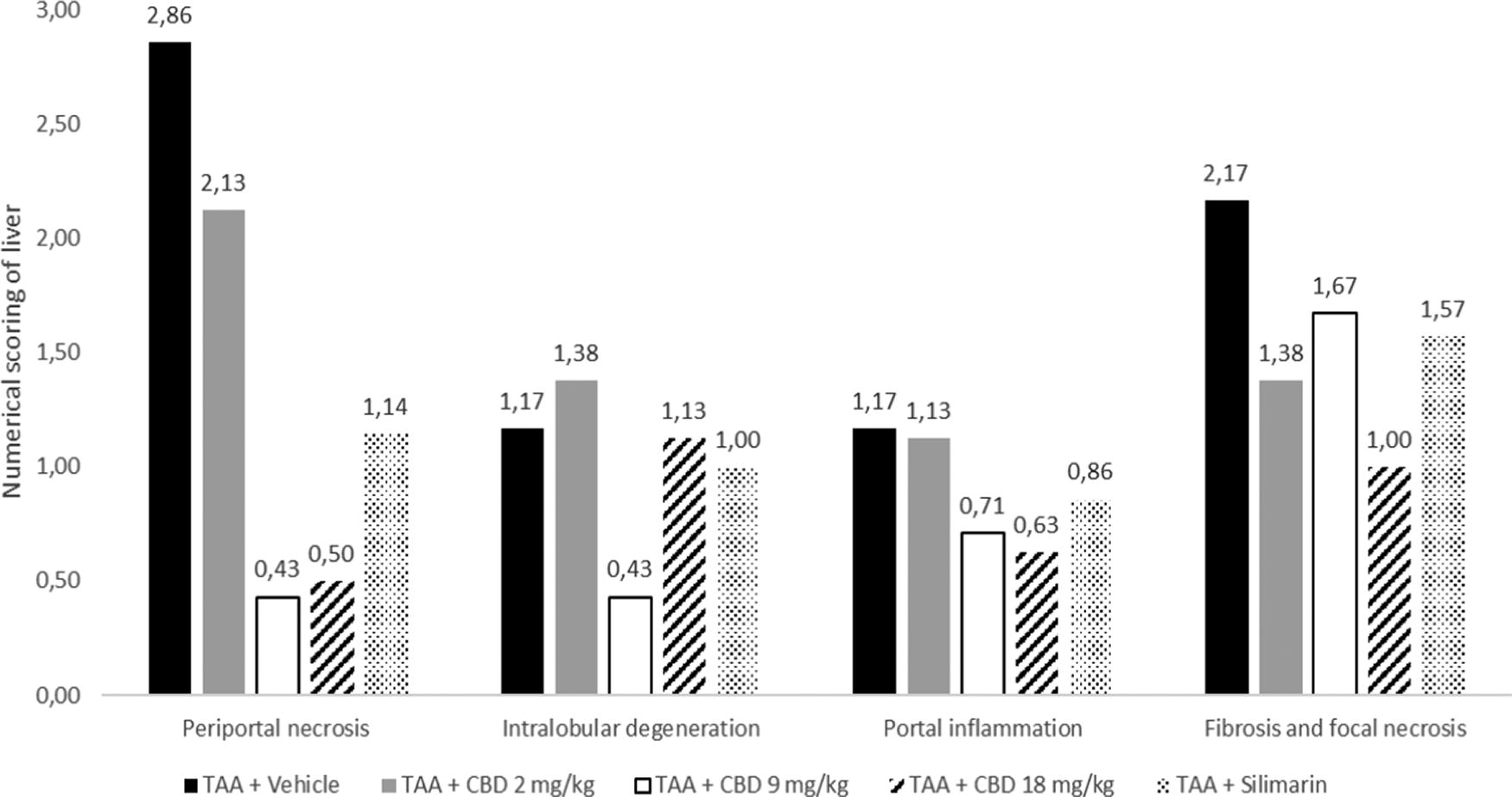
Histopathological analysis of liver tissue from animals treated with cannabidiol. The data represent numerical scoring of each component in liver biopsy samples ± SD. *Significant statistical difference with respect to TAA + Vehicle group (p < 0.05). ANOVA test and Post Hoc Tukey test. TAA, thioacetamide.
The HAI in liver tissue was significantly lower in animals treated with CBD at 9 mg/kg and 18 mg/kg, scoring 3.00 and 3.25, respectively, compared to the group receiving TAA + vehicle, which recorded a score of 7.0 (Fig. 4).

Histological activity index (HAI) in liver tissue with cirrhosis induced in rats treated with cannabidiol. The data represent total score of HAI in liver tissues ±SD. *Significant statistical difference with respect to TAA + Vehicle group (p < 0.05). ANOVA test. Post Hoc and Tukey test. TAA, thioacetamide.
Discussion
The endocannabinoid system comprised CB1 and CB2 receptors, their endogenous lipid ligands, and a pathway responsible for endocannabinoid synthesis and degradation. These components are distributed throughout tissues, including the brain and liver. Existing evidence strongly suggests the involvement of the endocannabinoid system in regulating hepatic hemodynamics, fibrosis formation, and lipid metabolism. Dysregulation of these functions is observed in pathological conditions such as cirrhosis, alcoholic fatty liver, and ischemia/reperfusion injury.12–14
Our results indicate that, at the end of the treatment period, groups receiving TAA experienced an increase in AST levels compared to baseline values. However, those treated with CBD at doses of 2 mg/kg and 18 mg/kg showed no significant change with an increase of 26.2 and 13.3 IU/L, respectively, compared with the TAA + vehicle group, which experienced a notable increase of 41.7 IU/L (p < 0.05). Similarly, ALT levels remained unchanged in all groups compared with their baseline serum levels. Only the TAA + vehicle group showed a significant increase in AST levels, reaching up to 95.64 IU/L (p < 0.05). Both ALT and AST are indicators of liver damage, and the observed decreases in the CBD-treated groups suggest a potential hepatoprotective effect. Other parameters such as alkaline phosphatase, bilirubin, albumin, and proteins did not show significant modifications at the end of the treatment. It is possible that the 6-week evaluation period is insufficient to detect variations in these tests, and cannabinoids’ inhibition of CYP450 may also contribute to these results. 15
Previous research on CBD’s therapeutic potential in hepatic injury induced by ischemia/reperfusion in rats demonstrated a significant reduction in serum levels of ALT and AST with CBD treatment at 5 mg/kg. 16 In addition, the role of CB2 receptors in the regenerative process related to hepatic injury has been investigated. In a model of acute hepatitis induced by CCl4, mice without expression of CB2 receptors experienced worsening hepatic injury, with elevated levels of AST and ALT, hepatocyte apoptosis, and delayed hepatic regeneration. Conversely, treatment with a CB2 receptor agonist resulted in a decrease in hepatic injury and an acceleration of hepatic regeneration, mediated by paracrine mechanisms affecting hepatic myofibroblasts. 5
Liver cirrhosis is a complex condition that involves structural changes in the liver tissue and alterations in biochemical markers. Levels of TB, DB, and ALP are commonly assessed as an indirect marker of liver fibrosis, which reflects alterations in hepatic function. However, it alone may not fully reflect the degree of cirrhosis. Nonetheless, it is an important indicator used alongside other clinical, imaging, or histopathological findings to evaluate liver function and disease severity.
Liver biopsy is a direct marker of liver fibrosis. Histopathological analyses have revealed that CBD-treated groups, particularly those receiving doses of 9 mg/kg and 18 mg/kg, exhibited reduced periportal necrosis compared to the TAA-only group. In addition, rats treated with CBD at 18 mg/kg showed decreased periportal inflammation and focal fibrosis and necrosis. Notably, only the groups receiving CBD at 9 mg/kg and 18 mg/kg demonstrated a statistically significant reduction in periportal necrosis. Concerning the HAI of hepatic tissue, animals treated with CBD at 9 mg/kg and 18 mg/kg exhibited lower scores of 3.00 and 3.25, respectively, compared to the TAA vehicle group, which recorded a score of 7.00.
The mechanisms underlying the hepatoprotective effects of CBD are complex. Some studies suggest that CBD can protect the liver against oxidative stress-induced steatosis caused by alcohol in mice, potentially by preventing the increase in oxidative stress and the activation of the JNK MAPK pathway. In addition, CBD has been observed to enhance autophagy in both HepG2 cells expressing CYP2E1 and mouse liver. 17 Treatment with CBD significantly mitigates increases in serum transaminases induced by alcohol-induced hepatic injury, along with reducing hepatic inflammation, oxidative/nitrative stress, triglyceride levels, and alcohol-induced liver fat accumulation. 18
It is highly probable that chronic activation of the CB2 cannabinoid receptor is related to the reduction of hepatic damage, as demonstrated in cirrhotic rats with ascites treated with a selective CB2 receptor agonist. This treatment improved blood pressure, reduced inflammatory infiltration, decreased the number of activated stellate cells, increased apoptosis in nonparenchymal cells, and reduced fibrosis compared to cirrhotic rats treated only with a vehicle. 19
In general, further research is needed to fully comprehend the molecular and cellular mechanisms through which CBD exerts its hepatoprotective effects. This could involve investigations into intracellular signaling and interactions with the endocannabinoid system, and how CBD specifically affects different types of hepatic cells, including hepatocytes, stellate cells, and immune cells in the liver. Determining the optimal CBD dosage for preventing the progression of hepatic cirrhosis remains a critical area of research. Moreover, the comparison with silymarin is still insufficient, as other agents have also demonstrated efficient action on stellate cells, preventing their activation and conversion. 20 In addition, exploring a diet-induced cirrhosis model rather than a toxin-induced model could provide valuable insights, considering the most common form of cirrhosis is derived from dietary and metabolic imbalances. 21
Conclusion
In conclusion, our results indicate that CBD has a hepatoprotective effect in the progression of experimental hepatic cirrhosis in rats. These findings suggest the potential of CBD in the therapy of hepatic cirrhosis, although further research is needed to fully understand its mechanism of action and clinical applicability.
Footnotes
Acknowledgment
We thank Reynaldo Madrid Prado and Diana Flores for their invaluable assistance and support throughout this research project.
Authors’ Contributions
D.F.-C. and E.V.-P. participated in the conceptualization, methodology, and investigation. C.I.-P., J.T.-B., J.R.-T., and G.G.-G. participated in the validation and investigation. D.F.-C., E.V.-P., J.T.-B., and J.R.-T. were involved in writing—reviewing and editing.
Authors Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
The project was supported by the Universidad Nacional Mayor de San Marcos (UNMSM) RR N°03556-R-19. Project number A19010411. The funders had no role in the study design, data collection and interpretation, or the decision to submit the work for publication.