
Abstract
Introduction:
Studies show that acute cannabis use significantly increases heart rate (HR) and mildly raises blood pressure in the minutes following smoked or inhaled use of cannabis. However, less is known about how the THC concentration of the product or an individual’s frequency of use (i.e., tolerance) may affect the magnitude of the change in HR. It is also relatively unexamined how the physical effects of increased HR after acute cannabis use relate to self-reported drug effects or blood THC levels.
Aims:
To describe the relationship between THC concentration of product used, self-reported subjective intoxication, THC blood levels, and frequency of cannabis use with the change in HR after acute cannabis use.
Materials and Methods:
Participants (n = 140) were given 15 min to smoke self-supplied cannabis ad libitum, HR was measured at baseline and an average of 2 min post-cannabis smoking. The ARCI-Marijuana scale and Visual Analog Scales (VAS) were administered, and blood samples were taken at both time points. Participants were asked about their frequency of use. Information about the product used was recorded from the package. Linear regression was used to analyze the relationship between changes in HR (post-pre cannabis use) and post-cannabis use HR, blood THC concentration, THC product concentration, frequency of use, and self-reported drug effect.
Results:
There was a significantly higher HR among those who smoked cannabis compared to the controls (p < 0.001), which did not significantly differ by frequency of use (p = 0.18). Higher concentration THC (extract) products did not produce a significantly different HR than lower concentration (flower) products (p = 0.096). VAS score was associated with an increase in HR (p < 0.05). Overall, blood THC levels were not significantly related to the change in HR (p = 0.69); however, when probed, there was a slight positive association among the occasional use group only.
Discussion:
Cardiovascular effects of cannabis consumption may not be as subject to tolerance with daily cannabis use and do not directly increase with THC concentration of the product. This is a departure from other effects (i.e., cognitive, subjective drug effects) where tolerance is well established. These findings also suggest that, at least among those with daily use, higher concentration THC products (>60%) do not necessarily produce cardiovascular physiological effects that are significantly more robust than lower concentration (<20%) products.
Introduction
After acute cannabis use, heart rate (HR) has consistently been shown to increase. 1 Studies have found that increases in HR after acute cannabis use can surpass the threshold of tachycardia (i.e., >100 beats per min), 2 and this effect has been observed across different modes of use (i.e., smoked, edible). 3 The ability to develop tolerance to the cognitive impairing effects of cannabis has been recognized for some time in the literature; however, there is conflicting data on the tolerance to the physiological change of increased HR. 4 Benowitz & Jones 5 found evidence of tolerance to the tachycardic effect of cannabis. Newmeyer et al. 6 did not find significant differences between use groups when comparing change in HR from pre- to post-cannabis use, but they did find that tetrahydrocannabinol (THC) concentration was associated with increased HR and THC blood levels in occasional users, which was not significant in daily users. This suggests partial tolerance to cardiovascular effects, irrespective of self-titration.
Few studies of acute cannabis use have included participants with a pattern of daily cannabis use or studied the effects of high THC concentration products. Among the only studies to consider this, Hendrickson et al., 2 did not find a difference in the frequency of tachycardia for those inhaling flower product compared to concentrate products, based on data taken from a poison control center.
The purpose of this study was to examine the acute effects of smoking cannabis on HR, exploring the effects of THC concentration in the product used, frequency of use, and the relationship with self-reported effects and blood THC levels. As an innovation to prior studies, the current study examined the use of products purchased from a retail marketplace (including extract products with high THC concentration) where recreational cannabis use is legal, allowing us to study these phenomena in an ecologically valid setting.
Methods
Participants (n = 140) were consented and enrolled into one of four cannabis use categories based on the frequency of their cannabis use (daily vs. occasional) and type of product used during the study (flower vs. extract products with a high THC concentration, herein referred to as “concentrate”): daily flower use (n = 39), daily concentrate use (n = 38), occasional flower use (n = 31), or no-use of cannabis as a comparison group (n = 32). There was no planned occasional concentrate use group. The Colorado Multiple Institutional Review Board approved the study procedures.
Participants were asked to abstain from cannabis use (8 h) before the start of their visit. They self-reported significant medical history and medication use and recalled their cannabis use over the last 30 days or 90 days (for occasional use groups) using a Timeline Followback Calendar to confirm their frequency of use. The ARCI-Marijuana scale and Visual Analog Scales (VAS) were administered to measure self-reported drug effects.7,8 HR measurements were taken with a digital blood pressure monitor (Omron HEM-907XL). Normal HR was defined as a resting HR between 60 and 100 beats per min. 9 After baseline assessments, participants were given up to 15 min to smoke ad libitum, except for the no-use group who did not use cannabis. The end of cannabis use was noted and typically occurred in fewer than the full 15-min period. Participants were asked to bring their own cannabis labeled with THC concentration, containing less than 2% cannabidiol (CBD), from a licensed Colorado dispensary. Details of the product label were recorded to obtain THC concentration. Venous blood samples were taken at baseline and after inhalation from an intravenous line. An average of 2 min after the participant’s end of inhalation, the ARCI and VAS scales were re-administered, and HR was recorded. Blood samples were taken approximately 20 min after the first inhalation of cannabis.
Linear regression was used to analyze the relationship between changes in HR (post-pre cannabis use) and post-cannabis use HR with (1) blood THC concentration, (2) THC product concentration, (3) frequency of use, (4) subjective drug effects, and (5) the interaction between blood THC level and frequency of use. All models were adjusted for age, gender, and race/ethnicity. Medications and medical conditions that suppress or induce tachycardia were controlled for in the analysis (Supplementary Tables S1 and S2).
Results
Participants used a wide range of cannabis concentrate and flower products procured from licensed dispensaries. These included flower buds, pre-rolled joints, cannabis concentrates (e.g., ‘sugar’, ‘shatter’), and oil. Methods for flower consumption included joints, bongs, ‘dry herb’ vaporizers; for concentrate consumption, dab rigs, ‘nectar collectors’, and vaporizers. On average, participants took 5.8 to 7.8 min to inhale their cannabis. The average THC content for flower products were 21.4% for those with occasional cannabis use and 22.2% for those with daily use. The average THC concentrate for concentrate products was 75.6% (Table 1).
Participant Characteristics and Cannabis Use
HR, heart rate; SD, standard deviation.
Participants in the daily flower and concentrate groups reported use on at least 29 of the last 30 days, while the occasional flower group reported use at least 3 but no more than 36 times in the 90 days prior to data collection, per the eligibility criteria. Participants were mostly White (81%), with 55.7% identifying their gender as male, 43.6% as female, and 0.7% did not identify on the gender binary. Most (46%) participants were between 30 and 39 years old at the time of data collection (Table 1). Table 1 presents the overall and mean blood THC levels, product THC concentrations, and HR pre- and post-cannabis use, categorized by use group.
Overall, in adjusted models (Table 2), among those who inhaled cannabis, the average increase in post-consumption HR was 26.6 beats per min (bpm) for daily use participants compared to non-users, and 31.6 bpm higher for occasional use participants to non-users (p < .001).
Analytic Results of Subjective Drug Effects and Cannabis Use/Products, Stratified by Use Group
Note: Values are regression coefficients adjusted for age, gender, race/ethnicity, medication use and medical conditions. Bolding indicated values are significant (p < 0.05).
The ARCI Marijuana questionnaire states, “I notice that my heart is beating faster” Participants marked “True” or “False”.
The drug effect questionnaire (VAS) asked, “Do you feel HIGH right now?” Participants marked on a 100 mm line visual analog scale from “not at all (0 mm)” to “extremely (100 mm)”.
CI, confidence interval; IR; interquartile range; VAS, Visual Analog Scales.
The concentration of THC in the product used was not significantly associated with the change in HR (p = 0.13). Further, the form of the product used (concentrate vs. flower) was not significantly associated with post-cannabis use HR (p = 0.08) or the change in HR (p = 0.16; Fig. 1, Table 2). There was no significant difference in HR or change in HR (pre-to-post) between the daily use and occasional use groups (Table 2). Additionally, there were no significant differences in post-consumption HR between daily concentrate vs. daily flower, daily flower vs. occasional flower, or daily concentrate vs. occasional flower (p ≥ 0.07) (Table 2). Blood THC level was not significantly related to the change in HR (p = 0.69) or post-consumption HR (p = 0.92) after adjusting for demographics, medications, and conditions (Table 2, Fig. 2). However, when evaluated by use group, blood THC level was positively associated with both the change in HR (p = 0.012) and post-consumption HR (p = .018) for the occasional flower group, but was not significant in the daily flower or daily concentrate groups ((p = 0.47) and (p = 0.25), respectively) (Supplementary Table S3).
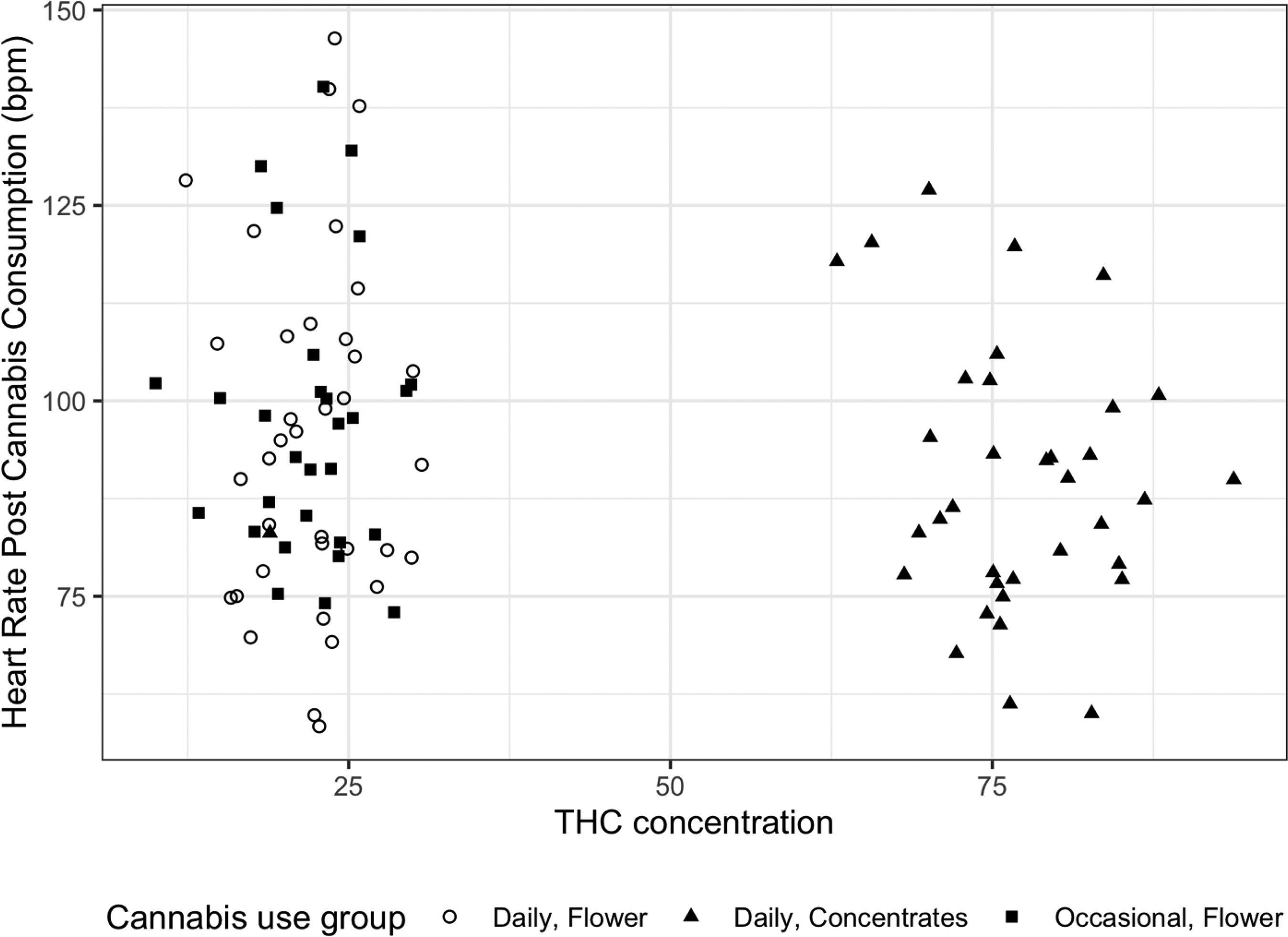
Post-consumption heart rate by THC concentration.
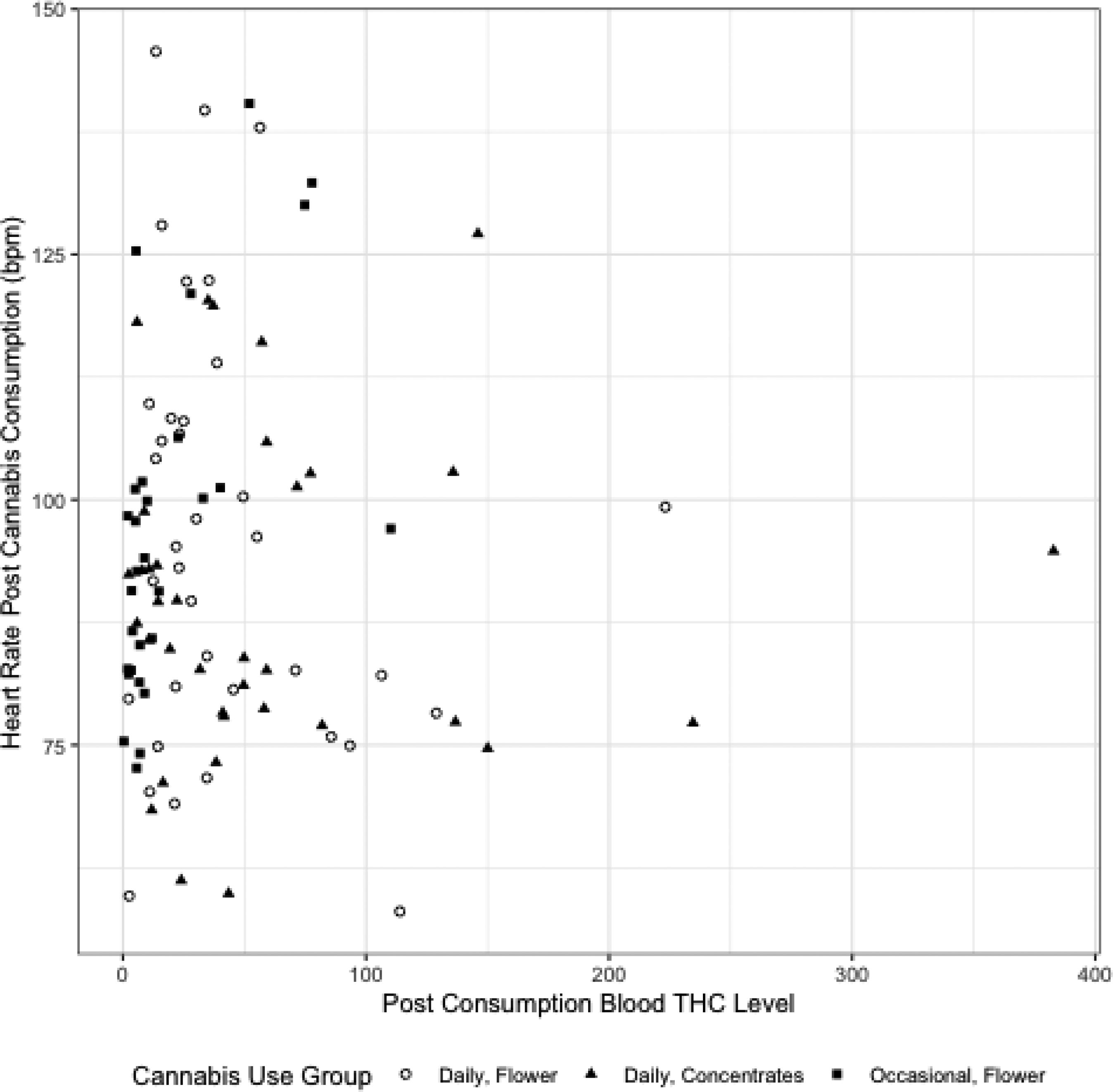
Post-consumption heart rate by blood THC level.
Self-reported feeling that the heart is beating faster (from ARCI-Marijuana Scale, post-cannabis consumption) were associated with a higher post-cannabis HR (p < 0.001). Feeling ‘high’ right now (from VAS) was associated with a greater increase in HR (p < 0.01) and significantly associated with post-consumption HR (p < 0.05), after adjusting for demographics, medication use, and medical conditions (Table 2).
Discussion
Definitions of “high” or “higher” THC concentration in products have evolved over time and historically ranged from anything above 2% to 18%.10–12 Nearly all prior studies no longer reflect what is sold in current retail marketplaces in US states with legal adult cannabis use. Recent studies have used products reflective of today’s legal market, such as >60% THC concentration, but much remains unexamined about the differential effects of higher THC concentration products. 13 Our results indicate that high THC concentration cannabis products (e.g., >60%) do not necessarily produce more robust changes in HR than products with lower concentrations (e.g., <20%). These findings corroborate data that previously demonstrated more robust cardiovascular effects were not associated with higher THC concentrate use. 2 It is important to gather more data on the relationship between high concentration products (representative of the modern marketplace) and physiological effects to distinguish the difference between dose (amount consumed) versus concentration of the product used.
We considered participants’ frequency of cannabis use as a measure of tolerance to the effects of THC, with daily use equating to potential tolerance. We did not find significant differences in post-use or change in HR between those with a pattern of daily use versus occasional use. This finding contrasts with other effects observed in prior studies, such as cognitive or subjective drug effects, where tolerance to cannabis is well established.14,15 Despite not finding an overall effect between blood THC level and HR, we did find a small positive relationship for the occasional use group only. Taken as a whole, our findings may suggest that the physiological effects of cannabis are less impacted by tolerance. This reduced physiological tolerance might be due to self-titration of use, regardless of product concentration. These findings are consistent with those of Leung et al., 15 who found that self-reported measures did not differ by mode of use or THC concentration and suggested that the lack of discrepancy might be due to tolerance of the neurological effects of THC and self-titration to euphoric symptoms. The observation that even with daily use there are changes in HR supports the use of HR as an objective marker of an isolated cardiovascular effect after recent cannabis use, regardless of pattern or product used, and could be used to validate self-reported use.
A limitation of this study is that HR was taken as a routine part of data collection for the purposes of participant safety and was not intentionally timed to capture near peak cardiovascular effects. We only observed HR at one time point post-consumption. We relied on self-report for medical conditions and prescription medication data. It is possible that medications may have influenced the subject’s baseline HR and response to cannabis. Another limitation is that we did not have an occasional concentrate use group and were unable to more extensively examine the relationship between tolerance and THC concentration. Additionally, our blood levels were measured approximately 20 min after the start of smoking, which does not necessarily reflect peak blood THC levels. Future research should examine what contributes to the differences in HR between individuals after acute cannabis use, as we did not find it be related to the product used or use history.
Further study is needed to tease out the nuance of the relationship between THC concentration, tolerance, and the physiological effects of cannabis. Additionally, future research should explore how oral cannabis use (i.e., the use of edibles) relates to cardiovascular effects, which was not examined in the current study. Data exploring and explaining the nature of this relationship may help inform the evolution of regulations regarding high concentration products.
Footnotes
Acknowledgment
The authors would like to acknowledge their research team who collected these data and the people who participated in the study.
Authors’ Contributions
S.L.: Conceptualization, Methodology, Writing, Data Curation, Original Draft Preparation. S.G.: Data curation, Writing—Original draft preparation, Software, Analysis, Validation. J.W.: Reviewing, Editing, Validation, Software, Supervision. G.S.W.: Reviewing, Editing, supervision. A.B.-R.: Writing—Reviewing and Editing, supervision.
Author Disclosure Statement
The authors of this article (Sarah Limbacher, Suneeta Godbole, Julia Wrobel, George Sam Wang & Ashley Brooks-Russell) have no conflicts of interest to disclose related to this work.
Funding Information
These data were taken from a larger study funded by NIH (NIDA)
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.