
Abstract
Background:
In 2023, Japan’s Cannabis Control Act underwent its first major revision since its establishment in 1948. The legal framework surrounding cannabis had long remained rigid, with limited scope for medical or industrial applications.
Methods:
This review examines the content and implications of the 2023 legal amendments based on governmental documents, legislative records, and secondary analyses of regulatory shifts. The assessment focuses on three key domains: medical application, industrial use, and drug control.
Results:
Under the revised law, cannabis-derived products intended for medical use were brought under the same regulatory framework as opioid analgesics, theoretically enabling physicians to prescribe them. Simultaneously, the longstanding restriction limiting industrial use to mature stalks and seeds was lifted. However, this liberalization was counterbalanced by the introduction of a stringent THC threshold. On the criminal side, cannabis continues to be regulated as an illicit substance, and new penalties for use have been introduced. The revised law came into effect on December 12, 2024.
Conclusion:
The 2023 amendment represents a significant shift in Japan’s cannabis policy, aiming to balance expanded medical and industrial opportunities with continued drug control. Its practical implications remain to be seen and warrant close monitoring in the coming years.
Introduction
The year 2023 marked a significant turning point in Japan’s cannabis policy as the Cannabis Control Act (CCA) underwent its first revision in 75 years. This amendment addresses various aspects, including the legalization of medical cannabis, the tightening of regulations on cannabis as an illegal drug, the promotion of the cannabinoid industry, and the protection of traditional hemp industries. Given the lack of academic reports on the history and content of these legal changes, this review aims to provide a comprehensive overview of cannabis use history in Japan, the background leading to the legal amendments, the details of the changes, and the future prospects following these revisions.
History of Cannabis Use in Japan
Cannabis use in Japan dates back at least 10,000 years, as evidenced by the discovery of cannabis ropes and seeds at Jomon-era archaeological sites. 1 Cannabis fibers were historically used to make ropes and clothing, while the leftover stalks were utilized for thatched roofs. Waste fibers were employed as materials for mud walls and plaster, and burned ash was used in portable heaters. Leaves served as fertilizer, and roots and flowers had medicinal applications. A medical textbook published in 1911 for aspiring physicians and pharmacists states that cannabis flowers were prescribed as a hypnotic and sedative. 2 Further, according to Keiken Senpō (“A Thousand Practical Remedies”), a comprehensive compilation of folk medicine published in 1817, a decoction made from cannabis roots was recommended for treating retained placenta after childbirth. 3 During the Meiji period (1868–1912), cannabis extracts and tinctures from Indian hemp were listed in the Japanese Pharmacopoeia from 1886 to 1951 and were used to treat conditions such as asthma and pain. 2 Cannabis seeds were not only consumed as food and animal feed but also used in traditional Chinese medicine under the name “Mashin-nin” for their laxative properties. Believed to ward off evil spirits, cannabis continues to be used in religious artifacts such as talismans (“Ise Jingu Taima”), purification rituals, and sacred ropes in Shinto shrines. 4
The Origins of Cannabis Regulation
In Japan, the cultural absence of cannabis as a recreational drug meant that regulation as a narcotic was introduced from abroad as part of international policy. Japan’s first cannabis regulation came under the International Opium Convention of 1912, which was largely symbolic. Effective regulation began with the enactment of the CCA in 1948. At the time, Japan was under Allied occupation, and General Douglas MacArthur, as Supreme Commander for the Allied Powers, played a pivotal role in establishing the nation’s legal framework. The Act was heavily influenced by the United States, where cannabis regulation had already been implemented. American officials, including narcotics officers and public health officials, advocated for a complete prohibition on cannabis cultivation. However, Japan’s appeals to permit cultivation, along with concerns from other departments of the General Headquarters about postwar shortages, led to a compromise directive that formed the foundation of the current CCA. 5 The law drew a distinction between narcotics managed by physicians and cannabis handled by farmers, resulting in the simultaneous enactment of the Narcotics and Psychotropics Control Act (NPCA) and the CCA on July 10, 1948. 6
Pre-Amendment Drug Regulations in Japan
Japan’s legal framework for regulating cannabis and cannabinoids includes three laws: the CCA, the NPCA, and the Pharmaceuticals and Medical Devices Act (PMDA).7–9
Cannabis Control Act
The CCA forms the backbone of cannabis regulation, prohibiting possession, cultivation, transfer, and use for research purposes by anyone other than licensed cannabis handlers. Article 4 of the Act explicitly bans the manufacture, prescription, and administration of cannabis-derived medicines, thereby clearly prohibiting medical use. Violators face penalties ranging from 5 to 10 years of imprisonment, although first-time offenders found in possession of small amounts typically receive a sentence of 1 year with a 3-year suspension. 10 Notably, the Act’s definition of cannabis excludes mature stalks and seeds, as well as products derived from them. This exclusion stems from the law’s origins in 1948, reflecting the traditional use of cannabis stalks and seeds for fiber and food. 11 Cultivation and research of cannabis are subject to licensing by prefectural governors, and usage is restricted to stalks and seeds. The extraction of cannabinoids, including from flowers and leaves, is prohibited under the current legal framework.
Narcotics and Psychotropics Control Act
While naturally derived Δ9-tetrahydrocannabinol(Δ9-THC) falls under the CCA, synthetic tetrahydrocannabinol(THC) compounds are regulated as narcotics under the NPCA. These compounds include seven variants, namely, Δ6a(7)-THC, Δ6a(10a)-THC, Δ7-THC, Δ8-THC, Δ9-THC, Δ9 (11)-THC, and Δ10-THC. 12 As narcotics, these compounds can only be accessed through prescriptions by licensed physicians, and unauthorized possession or use is strictly prohibited. Currently, these substances are not approved for medical use in Japan, leaving no legal means for their utilization.
Pharmaceuticals and Medical Devices Act
Since 2010, the regulation of novel synthetic cannabinoids (NSCs) has emerged under the PMDA. NSCs, which are absent or present only in trace amounts in natural cannabis, are chemically modified derivatives of THC, often exhibiting intoxicating effects.13,14 Under Japan’s designated substance system, NSCs identified as potentially harmful are regulated within ten days of designation, with penalties for violations including up to 3 years’ imprisonment or fines up to 3 million yen. 15
Current Status Under Existing Laws
Cannabis use and law enforcement
Japan’s lifetime cannabis use rate is 1.4%, among the lowest globally. 16 However, cannabis use has been increasing, particularly among younger populations. In 2023, cannabis-related arrests reached 6,482, surpassing arrests for violations of the Stimulants Control Act for the first time. 17 Authorities have conducted awareness campaigns targeting young people, although the effectiveness of these efforts remains unverified.
Cannabis cultivation
The number of cultivation licenses issued has dropped drastically from over 37,000 in 1954 to 27 in 2022. 18 In 2016, a licensee was arrested for possessing cannabis for recreational use, leading the Ministry of Health, Labour and Welfare (MHLW) to advise prefectures against issuing new licenses. 19
CBD product distribution
Exploiting a legal loophole, cannabidiol(CBD) products derived from mature stalks and seeds with undetectable THC levels have been imported legally since 2013. 20 Following the 2018 amendment to the U.S. Farm Bill, Japan saw an increase in CBD product imports. The domestic CBD market is projected to reach 80 billion yen (around 550 million USD at the current exchange rate) by 2025. 21
The trend and regulation of NSCs
Since October 2021, when hexahydrocannabinol (HHC), a NSC, began circulating, Japan has experienced what can be termed a second synthetic cannabinoid boom. The MHLW has consistently used the designated substance system to regulate new compounds as they emerge. From the regulation of HHC on March 17, 2022, to October 2024, there have been 14 additions to the list of designated substances. 22 However, the market continues to see the introduction of new compounds. As part of these regulatory measures, tetrahydrocannabivarin(THCV), a naturally occurring cannabinoid in cannabis plants, was designated as a controlled substance on September 10, 2023. THCV has a structure similar to Δ9-THC, a psychoactive component, but acts as a CB1 receptor antagonist in small amounts, lacking psychoactive effects. 23 The regulation made it impossible to use CBD supplements containing trace amounts of THCV. Following a plea from Ann Takahashi and her family, whose epileptic seizures relapsed due to the prohibition, academic organizations such as the Japan Clinical Association of Cannabinoids and advocacy groups such as Green Zone Japan and Patients of Cannabinoid Therapy submitted a joint petition through senator Kozo Akino, requesting the MHLW to allow the use of cannabinoid products containing trace amounts of THCV for health purposes. 24 Consequently, an individual application system was established to permit the use of such products. 25
Background of Legal Amendments
Since 2013, the domestic distribution of CBD products has enabled self-treatment by some patients with intractable epilepsy. The first documented case in Japan involved a six-month-old patient with developmental and epileptic encephalopathy. 26 Concurrently, Epidiolex, a CBD-based pharmaceutical, was approved in the United States for certain forms of intractable epilepsy. In 2019, Senator Kozo Akino asked in the Diet about the possible use of CBD pharmaceutical for epilepsy, based on a petition by Dr. Ichiro Takumi (last author of this article), in collaboration with Okinawa Red Cross Hospital, in responses to the voices of patients within Okinawa Prefecture, Japan. The MHLW publicly confirmed that clinical trials were feasible under the legal framework at that time, regardless of whether it is approved medicine in other countries or not, as long as phase II trials were completed.27,28 Subsequently, a government task force was established, which published its report in 2020. 29 Following this, Jazz Pharmaceuticals, the manufacturer of Epidiolex, submitted a notification for a multi-site clinical trial in Japan in 2022. 30
Since the CCA prohibited the use of cannabis-derived medicines after clinical trials, a movement toward amending the law began in January 2021. Initially aimed at enabling prescription CBD medicines, the amendment also sought to strengthen drug enforcement and promote industrial applications. Between January and June 2021, the MHLW held seven expert meetings to confirm its intention to continue prosecuting cannabis offenses. 31
In June 2021, a parliamentary group focusing on CBD was formed, and it has held periodic study sessions on cannabinoid utilization. 32 By April 2022, a study group led by prominent members of the ruling Liberal Democratic Party, including former Prime Minister Shinzo Abe, discussed preserving traditional cannabis cultivation. 33 Reflecting these efforts, the CCA amendment was passed during the 2023 extraordinary session of the National Diet. 34 The legislative intent behind this amendment of the CCA was to enable the medical use of cannabis in Japan, a statement repeatedly affirmed by the government of Japan as expressed by Kozo Akino, a member of the House of Councillors.
Summary of the New Law
The major changes resulting from the legal revisions are summarized in Table 1.
List of Major Changes Due to the Amendment of the Law
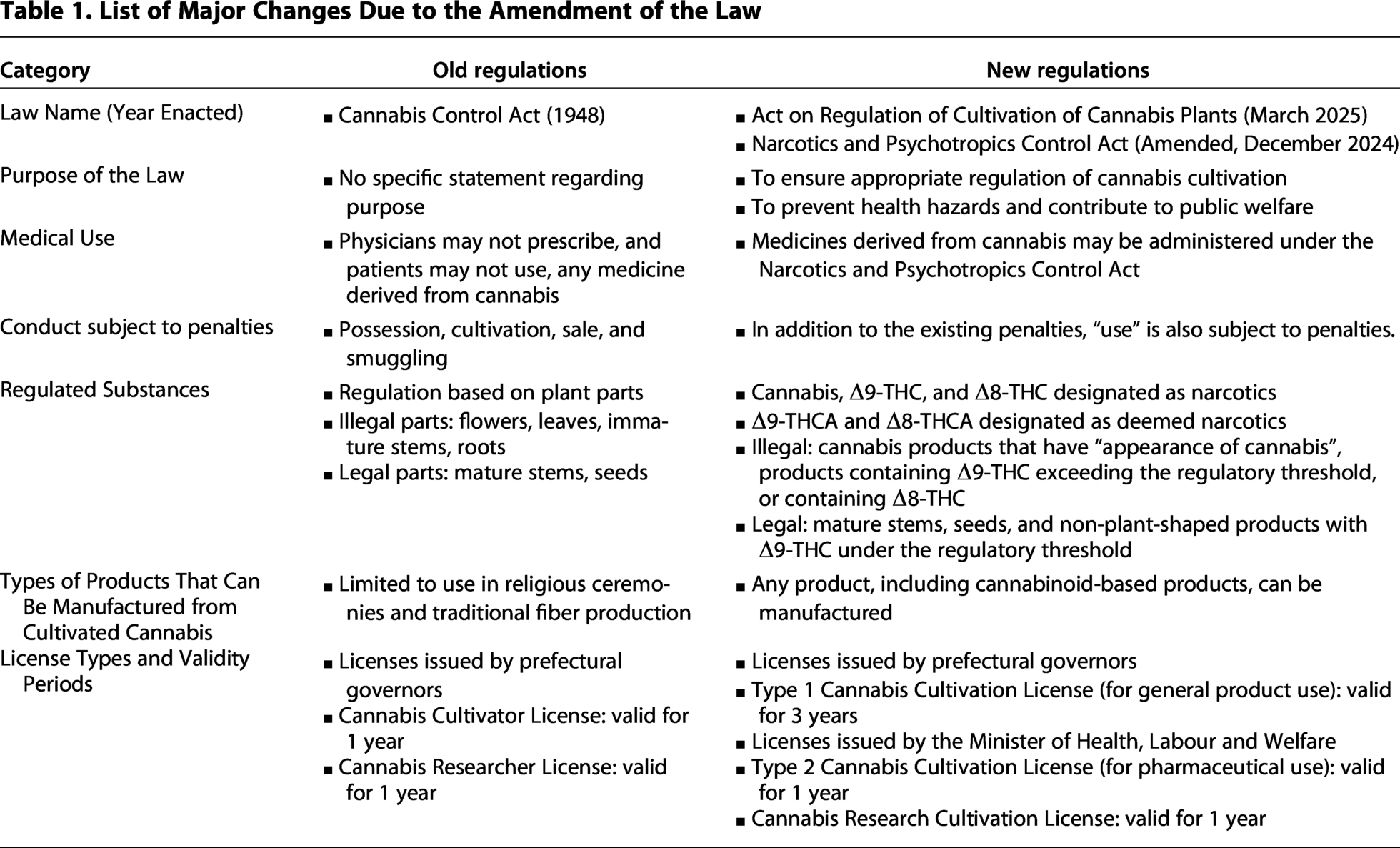
Legalization of medical use
The amendment repealed Article 4 of the CCA, which prohibited medical use of cannabis. Regulation of cannabis was transferred to the NCPA. 35 As a result, cannabis-derived medicines will now be treated similarly to opioids and other controlled substances, subject to strict prescription and use guidelines. Epidiolex, a CBD formulation expected to contain trace THC levels exceeding thresholds, is anticipated to be managed as a narcotic. 36
Control of cannabinoids as illegal substances
By transferring cannabis regulation to the NPCA, the distinction between synthetic and natural THC has been eliminated, unifying their management. Additionally, tetrahydrocannabinolic acid (THCA), a precursor to THC, is now classified as a narcotic. 34 The revised law imposes penalties of up to 7 years imprisonment for cannabis use, aligning it with other narcotics. Regulation of new synthetic cannabinoids continues under the PMDA’s designated substance system.
Industrial use of cannabinoids
Cannabinoids not classified as illegal substances can now be used industrially. The new law permits the use of cannabis-derived products, such as flowers and leaves, if their THC residue is below the specified threshold and if the products lack the “appearance of cannabis.” However, the definition of this term remains ambiguous. Differences in thresholds by product category are summarized in Table 2. Proposed thresholds for THC residue include 10 ppm for oils and powders, 0.1 ppm for aqueous solutions, and 1 ppm for other materials. 37
Differences in Thresholds by Product Category (Published by the Ministry of Health, Labour and Welfare)

Regulation of cultivation
The amended law, renamed the Act on Regulation of Cultivation of Cannabis Plants, introduced three cultivation licenses: Type I for low-THC industrial hemp (licensed by prefectural governors), Type II for medicinal cannabis (licensed by the MHLW), and a research cultivation license (licensed by the MHLW). Type I license is for the cultivation of cannabis varieties with a THC concentration of 0.3% or less, while Type II targets pharmaceutical applications, which allows growing any THC-containing cannabis cultivars. Type II licenses are intended for the sale of cannabis extracts to pharmaceutical companies and do not account for personal cultivation for self-use. The cultivation requirements for both Type I and Type II licenses include maintaining a cultivation area of at least 100 square meters. This stipulation is designed to prevent cultivation driven by personal hobbies or preferences.
Under the former CCA, cultivation licenses imposed excessively strict regulations, such as the installation of 2-meter-high physical fences and surveillance cameras for theft prevention, mandatory locks on entry gates, regular patrols of cultivation areas, and prohibitions on external visitors, photography, and accepting agricultural trainees. However, under the new law, cultivation of hemp varieties with a THC concentration of 0.3% or lower can meet requirements by implementing general anti-theft measures for agricultural crops. Additionally, Type I license holders, with additional authorization from the MHLW, are now permitted to import viable seeds from overseas and extract cannabinoids from the flowers and leaves of cannabis plants to manufacture and sell cannabinoid products. The Cannabis Research Cultivation License is designated for research related to cannabis cultivation. THC analysis can now be conducted by obtaining a Narcotics Researcher License.
Future Prospects and Challenges
Drug development and clinical research
The new law allows for the approval of cannabis-derived medicines through clinical trials, enabling their inclusion in Japan’s national health insurance system. At present, the only large-scale clinical trials being conducted are those using Epidiolex as the investigational drug, targeting Dravet syndrome, Lennox-Gastaut syndrome, and tuberous sclerosis complex. 30 These three conditions represent only a small fraction of refractory epilepsy cases, and it is anticipated that many epilepsy patients will continue to purchase and use commercially available CBD products.
However, stringent THC thresholds may limit patient access to certain CBD products. To address this, the MHLW has proposed a framework for “special clinical research” to facilitate the controlled use of such products. 38 A government task force on cannabis, led by Dr. Ichiro Takumi, has taken the initiative to design a research plan (jRCT s031240495 39 ), with studies initially set to focus on refractory epilepsy. This research has started in Dec 2024, and the patient inclusion will take place early 2025. It is hoped that the scope of research will eventually expand to include conditions beyond the three conditions of intractable epilepsy, to the various types of epilepsy, to the other medical conditions which are difficult to treat by the standard medical treatments.
The primary medical uses of cannabis in various countries include chronic pain, anxiety, insomnia, depressive symptoms, and malignant tumors, among others. 40 In Japan, the prevalence of chronic pain is 22.5% among adults, corresponding to an estimated 23.15 million people. 41 Additionally, approximately 6.03 million individuals are affected by some form of mental conditions, and around 1 million people are newly diagnosed with cancer each year.42,43 If patients with these conditions were granted access to cannabinoid-based products, it is anticipated that over 20% of Japan’s population could potentially benefit from such treatments.
Future prospects of the cannabinoid product market
The THC threshold set by the recent legal reform is expected to be one of the strictest standards in the world. A key challenge in operating under this stringent threshold will be addressing uncertainties, such as discrepancies in test results between different testing institutions. Additionally, there is concern about the possibility of testing institutions providing biased results to align with client intentions. Establishing a stable and reliable testing system will be critical in ensuring trust in the market.
The legal reform has raised expectations for major corporations to enter the cannabinoid product market. While the clarification of regulatory thresholds facilitates decision-making for market entry, the strict THC limits also increase the risk of unintentional regulatory violations, which may deter companies from entering the market. In general, under the NPCA, whether a violation is intentional or not is a critical focus. According to statements from government representatives during parliamentary discussions, exceeding the THC threshold by trace amounts does not automatically lead to regulatory actions, product recalls, or administrative guidance. 44 As long as companies investigate the cause and implement preventive measures, they are unlikely to face criminal charges or legal investigations.
Regarding synthetic cannabinoids, strict monitoring and guidance by regulatory authorities are expected to continue. However, the stringent THC threshold may pose a barrier to the utilization of naturally derived cannabinoids, potentially increasing the distribution of more potent and unknown synthetic cannabinoids. This situation raises concerns about a recurrence of the “cat-and-mouse” issues observed in the United States during the 2010s, where successive regulatory measures led to the emergence of new synthetic cannabinoids, causing widespread health risks. 45
Direction of drug policy
In the recent legal reform, the MHLW reaffirmed its policy of approving cannabis for medical use while simultaneously strengthening criminal penalties for illegal cannabis users. This punitive approach is often justified by the low rate of illicit drug use in Japan compared with other countries, which is perceived as evidence of the success of strict policies. However, this low usage rate may also reflect the exclusion of a small number of drug users from society, using them as examples or scapegoats, and relying on the “deterrent” effect of the law. Cross-sectional studies conducted in medical institutions and web-based surveys targeting cannabis users in Japan indicate that health and social harms caused by cannabis use are not clearly evident.46,47 Moreover, the number of users who meet the criteria for dependence is relatively low compared with other drug users, and many of these individuals also suffer from co-occurring mental health disorders. The strengthening of criminal penalties against cannabis users risks labeling such individuals as “criminals,” incarcerating them, and further excluding them from access to health and welfare services as “offenders,” thereby hindering their social reintegration. In this context, the priority for Japan’s drug policy should shift from strengthening criminal penalties to improving access to support services for individuals with drug-related issues and reducing stigma.
In recent years, international drug policies have been shifting toward alternatives to punitive measures. In 2021, the United Nations Office on Drugs and Crime, the Office of the High Commissioner for Human Rights, and the Department of Peace Operations jointly urged member states to reconsider the excessive incarceration of individuals involved in drug offenses. 48 Additionally, in March 2024, the 67th session of the UN Commission on Narcotic Drugs adopted a recommendation recognizing harm reduction measures, with Japan voting in favor. 49 In the United States, which has greatly influenced Japan’s cannabis policy, as of October 2024, 38 states and Washington, D.C. have legalized medical cannabis, while 24 states and Washington, D.C. have legalized recreational cannabis. 50 Further, in October 2022, President Biden acknowledged the errors of previous punitive cannabis policies and announced a shift in approach, including granting pardons to offenders. 51 Following this, in April 2024, the Drug Enforcement Administration announced its intention to reclassify cannabis from Schedule I to Schedule III under federal law. 52 Possession and use of cannabis by adults aged 18 and over has already been legalized in Canada in 2018 and in Germany in 2024.53,54 The influence of these countries is expected to gradually spread to surrounding regions in the coming years.
An example of delayed administrative action despite scientific consensus can be seen in Japan’s handling of Hansen’s disease. Although Hansen’s disease became treatable with the invention of Promin in 1943, and the 7th International Leprosy Congress held in Tokyo in 1958 recommended transitioning to outpatient treatment instead of isolation policies, the Japanese government did not repeal its isolation policy until 1996. 55 This delay led to large-scale compensation claims by patients, resulting in a court ruling against the government and the payment of reparations. 56
The recent amendment to the CCA includes a provision for reviewing its content within 5 years. It is hoped that future reviews will incorporate international recommendations on drug policy. Further, drug education activities should be adjusted to balance messages about abuse prevention and medical use, and the effectiveness of such educational efforts should be rigorously evaluated.
Future prospects of cannabis cultivation
In the past, the unavailability of domestically produced cannabis in Japan forced the traditional crafts industry to rely on synthetic fibers or imported cannabis materials. However, with the implementation of the new law, it has become possible to utilize domestically cultivated cannabis materials once again. Hemp, derived from fibers, seeds, and flowers or leaves, has a wide range of applications, including clothing, accessories, food products, supplements, cosmetics, paper, construction materials, bedding, plastics, animal feed, and fertilizers. It has also gained attention for its potential to contribute to CO2 reduction. 57 Pioneering initiatives have already begun in Tochigi, Mie, and Hokkaido Prefectures, where cannabis is being explored as an agricultural crop to promote regional development and agricultural revitalization.58–60 Additionally, the new law permits not only seed cultivation but also vegetative propagation through cloning, paving the way for companies to explore cannabis cultivation in fully artificial environments such as plant factories.
On the other hand, while the THC threshold for agricultural purposes is set at 0.3%, the threshold for final products is an extremely strict 1/300th of that value. This creates significant barriers for the domestic production of CBD raw materials due to the advanced knowledge and expensive equipment required for purification, as well as competition with imported cannabinoids. Moreover, the THC threshold may impose restrictions on the use of seeds, as well as the application of flowers and leaves in foods, cosmetics, animal feed, and fertilizers. As a result, efforts are underway to introduce THC-free hemp varieties developed abroad and to initiate breeding research aimed at reducing THC content to zero in domestic varieties.61,62
As for cultivating cannabis for pharmaceutical purposes, the 75-year prohibition period has made it unlikely that domestic pharmaceutical or herbal medicine companies will readily engage in cultivation research. However, the new law, which classifies cannabis flowers and natural Δ9-THC as narcotics, allows for collaborative research using cannabis cultivation researcher licenses and narcotics researcher licenses. Given the lack of knowledge from human clinical trials and animal studies, progress in these research areas is highly anticipated. Further, with the expected increase in entrants into cannabis-related industries under the new law, operational insights regarding the legal framework are likely to accumulate. This may reveal situations where issues arise uniquely within Japan compared with other countries. It is essential to incorporate feedback from practitioners into future reviews of the legal framework and related policies.
Conclusion
The 2023 amendment to the CCA marks a significant milestone in Japan’s drug policy, enabling medical cannabis use and promoting industrial applications while maintaining strict control over recreational use. Its implementation on December 12, 2024, will require careful observation to assess its broader impact.
Authors’ Contributions
Y.M.: Project administration, methodology, writing—original draft, conceptualization, and investigation. Y.A.: Conceptualization, writing—original draft, and investigation. M.K.: Conceptualization and writing—original draft. F.U.: Conceptualization and writing—original draft. N.M.: Writing—review and editing and conceptualization. R.N.: Conceptualization and writing—original draft. K.S.: Conceptualization and writing—original draft. C.Y.: Conceptualization and writing—original draft. R.M.: Conceptualization and writing—original draft. T.M.: Writing—original draft, supervision, and conceptualization. K.A.: Conceptualization and direct lead on the legal reform. I.T.: Funding acquisition, conceptualization, and direct participation in discussions on legal reform.
Footnotes
Funding Information
Article submission fee of this report was funded by the Fiscal 2024 Health and Labor Sciences Research Grant, entitled “Regulatory oversight of cannabinoid pharmaceuticals and cannabinoid products 24CA2012 (to Y.M., Y.A., T.M., N.M., and I.T.)” in part. This study was also supported in part by the Japanese Clinical Association of Cannabinoids.
Declaration of Conflicting Interests
The author(s) declared potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Financial relationships
Y.M. and N.M. receive a salary from Green Zone Japan. R.N. is a shareholder of Asabis Inc., which has business relationships with companies involved in cannabidiol-related products, and receives a salary from the company. K.S. is a shareholder of ONE-INCH Ltd., a company engaged in the sale of cannabidiol-related products, and receives a salary from the company. C.Y. is a shareholder of ASTRASANA JAPAN Co., Ltd., a company engaged in the sale of cannabidiol-related products, and receives a salary from the company.
Institutional relationships and sponsorship
Y.M. reports that a non-profit organization with which he is affiliated (Green Zone Japan) has received sponsorship from companies involved in cannabidiol-related products. He received no personal fees from these sponsors.
Research funding
Y.M., Y.A., T.M., N.M., and I.T. are members of a research group supported by the Health, Labour and Welfare Policy Research Grants (24CA2012 and 25KC2006).
Non-financial relationships
Y.M., Y.A., and I.T. are affiliated with the Japanese Clinical Association of Cannabinoids (JCAC). K.A. is a Senator and a member of the House of Councillors (Fukuoka Prefecture), Japan. I.T. leads a government task force on cannabis and is responsible for developing a research plan (jRCT s03124049539), with studies initially focused on refractory epilepsy.
Statement on funding and role of organizations
The study was supported in part by the Health, Labour and Welfare Policy Research Grants (24CA2012). The funders had no role in the study design, data collection, analysis, interpretation, manuscript preparation, or decision to publish. The organizations listed above did not provide funding, materials, or editorial support for this work.