
Abstract
Introduction:
With the changing legal landscape, the acceptance and availability of cannabis products have increased. Cannabis products are generally considered “natural” and relatively safe by consumers. However, growing empirical evidence from humans and other animals indicates that cannabis negatively affects human health. In contrast to the well-known teratogenic effects of alcohol and tobacco products, the safety of cannabis product use during pregnancy has not yet been established. The goal of this systematic review was to determine the patterns that exist in human and rodent literature on the effects of prenatal exposure to cannabis products and delta-9-tetrahydrocannabinol (THC) on birth outcomes.
Methods:
A systematic review of rodent and human studies was conducted using PRISMA guidelines. Rodent search strategy used PubMed and Scopus with terms “prenatal OR perinatal OR in utero OR maternal exposure AND cannabis OR THC or cannabinoids AND exposure NOT review NOT Human.” Human search strategy used PubMed, CINAHL, and Scopus with terms “cannabinoids OR cannabis OR THC OR marijuana” AND “pregnancy OR pregnant OR prenatal AND “infant outcome OR infant health.” After deleting duplicates and studies that did not fit the inclusion criteria, 21 rodent and 36 human studies were selected for review. Rodent studies focused on birth weight, litter size, mortality, and gestation length. Human studies have focused on birth weight, gestational age, and infant health at delivery.
Results:
In both human and rodent studies, prenatal exposure to cannabis was significantly associated with lower birth weight; however, it was not significantly associated with gestational age in rodents or humans. In most rodent studies, prenatal exposure to cannabis did not affect mortality or litter size. In human studies, there was a tendency for infants exposed to cannabis during pregnancy to have worse health at delivery. Findings indicate that cannabis exposure in utero may be associated with worse birth outcomes; however, the results are mixed and vary by species and outcome.
Discussion:
Methodological differences and scant existing research may have contributed to this inconsistency. Given the legalization of cannabis product use for recreational and medicinal purposes is growing, additional research is necessary to determine its influence on fetal and infant health outcomes.
Introduction
Over the past 25 years, societal perceptions and use of cannabis products have shifted significantly. As of early 2024, recreational use of cannabis was legalized in 24 U.S. states: Guam, the Northern Mariana Islands, and Washington, D.C. 1 In 2022 alone, 3.7 million people over the age of 12 used cannabis products for the first time, representing a 42% increase from the previous year.2,3 Cannabis products are often marketed as a safe and natural solution to general discomfort, including pregnancy-related effects, such as morning sickness, insomnia, and pain. 4 Indeed, cannabis use has increased substantially among pregnant persons. 5 From 2002 to 2017, cannabis use during pregnancy increased from 3.4% to 7.0%. 6 More recently, the rate of cannabis product use by pregnant people was as high as 16.2% nationally, with some states reporting up to 26%. 7 Moreover, 18.1% of those reporting cannabis product use during pregnancy met the criteria for abuse and/or dependence. 8 Unlike the well-known teratogens, alcohol, and tobacco, relatively little research has focused on the potential deleterious effects of cannabis product use during pregnancy. With the increasing rate of cannabis use during pregnancy, there is a critical need for a clear understanding of the effects of cannabis and its constituent compounds on aspects of fetal development and birth outcomes.
The primary psychoactive compound in cannabis is delta-9-tetrahydrocannabinol (THC), which binds and activates endocannabinoid receptors. Vertebrate animals, including humans, have an evolutionarily well-maintained endogenous cannabinoid system that modulates the stress response, anxiety, memory, pain, and motivated behavior across the lifespan. 9 Endocannabinoid signaling also modulates physiological processes necessary for the development, maturation, and refinement of neural circuits throughout adolescence, establishing this system as an integral component in the developing neonate. 10 Two cannabinoid receptor subtypes, CB1 (i.e., CB1R) and CB2 (i.e., CB2R), are expressed throughout the body. CB1 is expressed at relatively higher levels in neural tissues, including the brain, and is responsible for the well-documented euphorigenic effects of THC. 11 In contrast, CB2 is constitutively expressed peripherally in immune cells and inflamed or damaged tissues and at low levels in the brainstem. Cannabinoid receptors are expressed on placental membranes and within the developing fetus. 12 The presence of receptors allows THC to cross the placenta,13,14 which may negatively impact the facilitation of the exchange of oxygen, vital nutrients, micronutrients, waste, and endocrine signals between the mother and fetus.15,16 Deficiency in any of these functions may increase the risk of preterm birth, congenital anomalies, neurobehavioral dysfunction, and perinatal mortality.17,18 Given the growing prevalence of cannabis product use, it is imperative to determine the extent to which cannabis exposure during pregnancy affects fetal and birth outcomes.
The endocannabinoid system is evolutionarily conserved in vertebrates and shares homology with rodents and humans. Thus, rodents offer a suitable preclinical model to investigate the effects of prenatal THC exposure in humans. Indeed, most experimental animal literature has focused on rodent models. The effects of prenatal cannabis or THC exposure have been assessed across three broad categories of outcomes: birth, neurodevelopment, and behavior. Previous reviews of rodent literature have identified the potentially adverse effects of prenatal THC exposure on neurodevelopmental and behavioral outcomes. For example, objectively measured deficits in executive function have been associated with prenatal cannabis or THC exposure, such as reduced attention and inhibitory control associated with increased aggression and widespread alterations in various neurotransmitter systems. 19 In addition, prenatal THC exposure has been associated with poor locomotor and exploratory behaviors in rats. Cognitive impacts include memory and learning impairments, attention deficits, prolonged task completion times, and altered responses to visual stimuli. Emotional changes in rodents prenatally exposed to THC included increased separation-induced ultrasonic vocalizations, decreased social interaction and play behavior, and heightened generalized anxiety. 20 Thus, adverse effects of prenatal cannabis or THC exposure have been noted for neurodevelopmental and behavioral infant outcomes, but most of these studies were conducted in rodents. Given the ethical and logistical constraints (e.g., time and money), very little research has been conducted on humans.
The developmental origins of health and disease (DOHaD) hypothesis suggests that the perinatal environment influences both fetal and lifelong health. 21 As the interface between maternal and fetal systems, the placenta mediates the transfer of nutrients, oxygen, and xenobiotics, including THC and its metabolites, making it a direct archive of in utero cannabis exposure. Placental analysis enables quantification of cannabinoids and assessment of related gene expression and epigenetic changes, offering insight into pathways through which cannabis may affect fetal development and preterm birth. As a routinely collected and ethically accessible tissue, the placenta serves as a valuable tool for studying prenatal cannabis exposure within the DOHaD framework. 21 For example, preterm infants often experience retinopathy of prematurity, an irreversible visual impairment, and 23% of preterm infants who require respiratory support develop bronchopulmonary dysplasia, a chronic lung disease.22,23 Moreover, lifelong limitations, such as cerebral palsy, kidney disease, and cognitive impairment, are common. 24 Given these potentially devastating outcomes, it is critical to understand whether prenatal cannabis exposure alters birth outcomes, which may be indicative of neurodevelopmental and behavioral concerns.
The goal of the current systematic review was to recapitulate preclinical rodent and human literature on the effect of prenatal cannabis exposure on neonatal birth outcomes. We operationalized birth outcomes as any metric of the progeny’s overall health, gestational characteristics affecting birth (e.g., length of gestation), or general physical features (e.g., birth weight). Thus, we were able to compare the effects of THC and cannabis products on the physical state of neonates.
Method
Search strategy
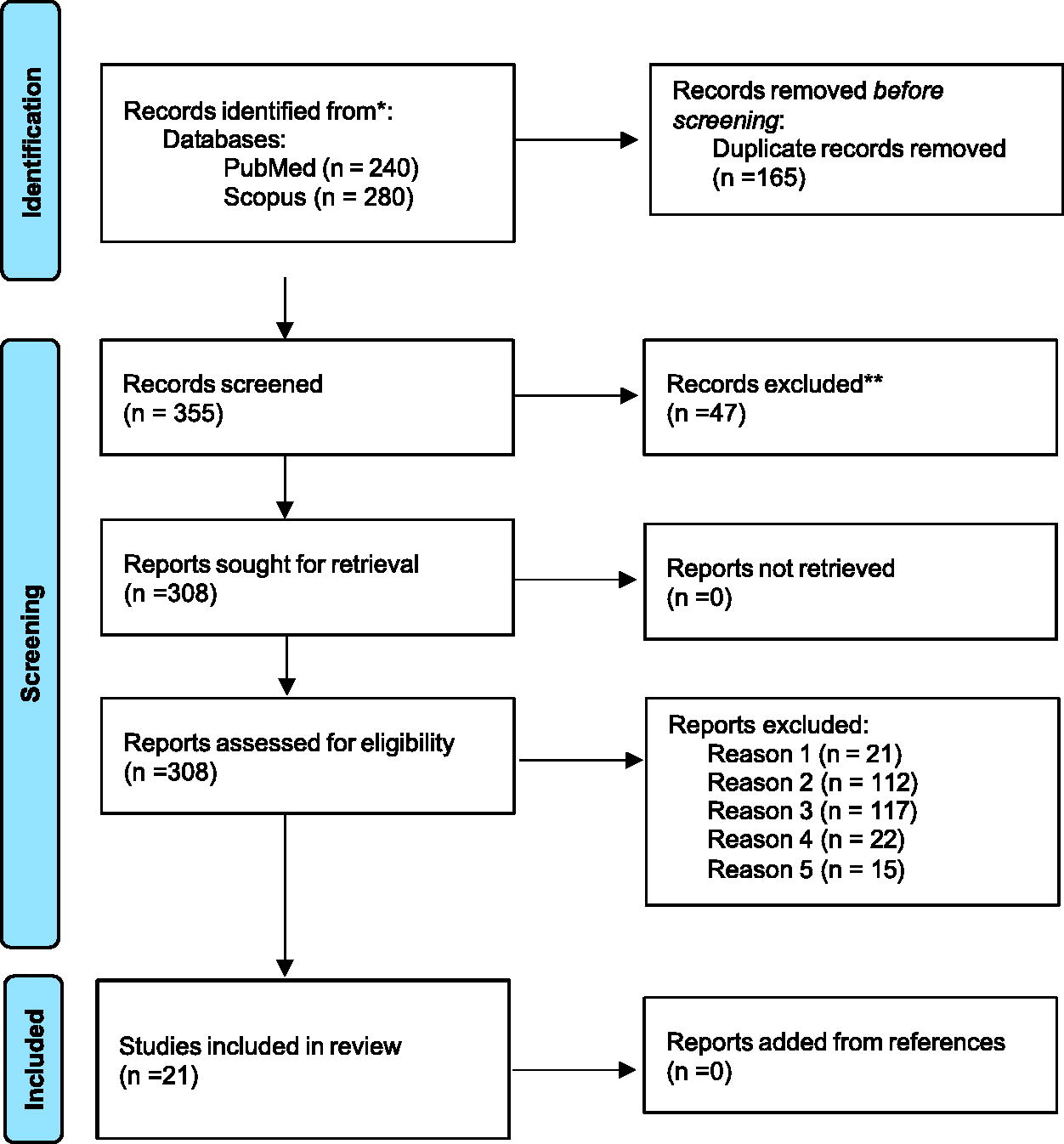
The systematic literature review was conducted per PRISMA guidelines. 25 All search criteria and review procedures were determined a priori, although the review was not preregistered. A comprehensive search of preclinical (rodent) literature was conducted in PubMed and Scopus, initially on March 22, 2024, and again on July 18, 2024. The search terms were “prenatal OR perinatal OR in utero OR maternal exposure” AND “cannabis OR THC OR cannabinoids” AND “exposure.” The search excluded review articles, human studies, and articles published in languages other than English. A literature search was conducted by two independent reviewers (A.M.R. and S.O.V.; see Fig. 1).
Identification of preclinical studies via databases and registers.

Identification of human studies via databases and registers.
For the human literature, a comprehensive search was performed in PubMed, CINAHL, and Scopus with the terms “cannabinoids OR cannabis OR THC OR marijuana” AND “pregnancy OR pregnant OR prenatal” AND “infant outcome OR infant health.” The search excluded review articles, non-human studies, and articles in languages other than English. A literature search was conducted by two independent reviewers (T.R. and S.G.C.; see Fig. 2). The reference lists of the identified articles were reviewed to identify additional relevant studies.
Identification of human studies via databases and registers.
Duplicate articles were removed after compiling the search results. Articles were initially screened based on their title and abstract for eligibility for review. Those deemed relevant were further assessed for inclusion based on a full-text evaluation.
Eligibility criteria
Inclusion criteria for preclinical literature were gestational exposure to THC, rodent exposure to THC during gestation and before birth, articles written in English, articles published in the last 50 years, and articles focused only on rodent models. The exclusion criteria included non-primary research sources (reviews, opinion pieces, etc.), testing age > postnatal day 30, and human studies.
The inclusion criteria for human literature were documentation of cannabis product use, examination of infant birth outcomes, publication within the past 10 years (2014–2024), and English language. Articles were excluded if they were not primary research articles (e.g., reviews, opinion pieces, etc.) or if the relationship between prenatal cannabis product use and study outcomes was not assessed independently of polysubstance use.
Data extraction and synthesis
Two independent coders reviewed articles that met the inclusion criteria. The following data were extracted from rodent literature: Species Strain, THC Dose and Route of Administration, Prenatal Treatment Timing, Major Outcome Variable(s), Sex, Testing Age, Statistical Significance, and Effect Size (see Table 1). For human literature, the following data were extracted: Study Design, Major Outcome Variable(s), Statistical Significance, Effect Size, Major Findings, Sample Size and Year Participant Was Enrolled, Demographics, and Method of Cannabis Measurement (see Table 2). The extracted data were analyzed and synthesized narratively, with a primary focus on the relation between prenatal cannabis product use or THC exposure and birth outcomes.
Data Extracted from Rodent Literature
s.c., subcutaneous; THC, delta-9-tetrahydrocannabinol; ns, Not Significant; ND, Natal Day; ROA, Route of Administration; NR, Not Reported.
Data Extracted from Human Literature
APGAR, Appearance, Pulse, Grimace, Activity, Respiration; BL, birth length; BW, birth weight; CUD, cannabis use disorder; ELBW, extremely low birth weight; FGR, fetal growth restriction; FPWR, feto-placental weight ratio; GA, gestational age; HC, head circumference; LBW, low birth weight; NICU, neonatal intensive care unit; NNR, neonatal resuscitation; O2, required oxygen; PCE, prenatal cannabis exposure; PTB, preterm birth; RDS, respiratory distress syndrome; SB, stillborn; SCN, special care nursery (step-down-from NICU); SGA, small for gestational age; ns, Not Significant.
Results
Selection of sources
The systematic search of the rodent literature identified 520 articles (Fig. 1). Following the removal of duplicates and initial exclusion, the titles and abstracts of 30 articles were screened according to inclusion and exclusion criteria. Of these, 21 were selected for full-text analysis, all meeting inclusion criteria for the data extraction and review.
A total of 611 human subject articles were initially identified in the search (Fig. 2). After removing duplicates, the titles and abstracts of 417 articles were screened, and 51 articles were removed based on the inclusion and exclusion criteria for abstract screening. Sixty-six articles underwent a full-text review to determine eligibility based on the inclusion and exclusion criteria. Of these, 36 met the inclusion criteria for data extraction and analysis.
Study characteristics
Of the 21 rodent articles reviewed, the majority were conducted in the United States (n = 10),26,27,33–35,37,38,42,80,81 followed by Canada (n = 6),30,32,36,39–41 Italy (n = 2),29,31 Hungary (n = 1), 43 Spain (n = 1), 28 and France (n = 1). 44 The route of administration of THC differed between oral (n = 10),27,28,33,35,37,38,41,80,81 intraperitoneal (n = 7),30,32,36,39,40,43,44 subcutaneous (n = 3),26,29,31 and vapor inhalation (n = 1). 42 The initiation of prenatal THC injections varied, although the majority began treatment before day 10 of gestation (n = 18), which is generally considered the end of the first human trimester when extrapolating development to rodent models. Among the 21 studies investigating birth outcomes preclinically, body weight was the most common outcome variable (n = 21), followed by litter size (n = 14), mortality rates (n = 9), and length of gestation (n = 5).
Of the 36 human subject articles reviewed, the majority (n = 25)8,45–48,50,51,53,56–61,66–68,70,71,73–75,77–79 were conducted in the United States, followed by Canada (n = 5), Australia (n = 3), and the United Kingdom (n = 1). Two studies included international samples from Australia, New Zealand, Ireland, and the United Kingdom.55,63 All studies employed quantitative designs; most were retrospective (n = 35). However, three studies utilized a prospective cohort design.55,60,63 Sample sizes varied widely from 198 mother–infant dyads to 4.8 million mother–infant dyads. 8 Among the 36 human subject articles reviewed, infant birth weight was the most frequently investigated outcome (n = 35), followed by length of gestation (n = 24) and infant health at the time of delivery (n = 18).
Birth outcomes
Is prenatal cannabis or THC exposure related to birth weight?
Birth weight has been the most frequently examined outcome in both rodent and human studies. All 21 rodent studies investigated the impact of prenatal cannabinoid exposure (PCE) on birth weight compared with control groups. Of these, 16 reported significantly lower body mass in PCE groups than in control groups.26–30,32,33,36,37,39,41–44,80,81 The other five articles did not find significant differences between groups.31,34,35,38,80 In addition to general body mass, heart,36,41 liver,39,80 placenta,28,39,41 pancreas, 32 and brain mass 30 were lower in PCE groups compared with control groups. Notably, the effect of PCE on birth weight in rodents may be time dependent. Eleven articles measured rodent body mass at varying developmental time points. They reported that the differences between the PCE and control groups became comparable following either a “postnatal catch-up” period26,29,30,32,36,41,44,81 or when assessed at an early point in gestation (i.e., before birth).39,80 This time-dependent effect of PCE on body mass in rodents is underscored by one study, which measured average body mass gain over time and found that mass was significantly lower in PCE groups compared with non-PCE control groups early in the postnatal period, but no longer differed from the non-PCE control groups from postnatal day 11 onward. 33
Thirty-five human articles examined the association between infant birth weight and cannabis product use during pregnancy. Birth weight is a crucial indicator of an infant’s health. Those infants born at lower birth weights typically require neonatal intensive care unit (NICU) admission and more potentially stressful interventions. However, the definition of birth weight varies. Most studies (n = 25) classified birth weight outcomes categorically as small for gestational age (SGA; <10th percentile) or low birth weight (LBW; birth weight <2,500 g). Four studies examined birth weight as a continuous variable (i.e., weight in grams or ounces).55,60,62,76 Fifteen studies reported that infants with PCE were more likely to be SGA than non-PCE infants.8,45,46,48,50,52,59,62,64,69,73–75,78,79 Thirteen studies found that prenatal cannabis product use was associated with a higher risk of delivering an LBW infant.8,46,49,53,54,56–58,64,71,72,75,78
Furthermore, eight studies reported a significant relationship between prenatal cannabis use and lower mean birth weight.8,55,60,62,67,76–78 Notably, one study observed this effect only in male infants. 67 Conversely, seven studies found no significant association between maternal prenatal cannabis exposure and birth weight, including categorical and continuous measure of birth weight.51,53,56,61,63,71,82
Is prenatal cannabis or THC exposure related to gestational age?
The effect of PCE on gestation length was assessed in five rodent studies.18,25,81,83,84 None of the included studies reported a significant effect. That is, gestation length did not differ significantly between the PCE and control groups.
The relationship between prenatal cannabis product use and gestational age at delivery in humans was examined in 30 studies. Of these, 25 addressed the correlation between PCE and preterm birth (i.e., delivery before 37 weeks of gestation) and full-term birth. Four studies investigated the association between cannabis product use during pregnancy and overall length of gestation.54,55,67,70 Among the studies focusing on preterm birth, 10 reported a significant association between prenatal cannabis product use and an increased likelihood of preterm delivery,8,46–48,63–65,70,72,73 whereas 11 reported no association between PCE and preterm delivery.49,52–54,57,59–61,69,71,74 Of the four studies that examined the overall length of gestation, two reported that a lower gestational age was associated with PCE.55,70 In contrast, two studies reported no association between PCE and gestation length.54,67
Is prenatal cannabis or THC exposure related to mortality rates and health at the time of delivery?
Within rodent studies, litter size (n = 14) and mortality rates (n = 9) following PCE administration were compared with those in controls.26–31,33,34,37,39,41,42,44,81 Only one study found a significantly smaller litter size following PCE compared with controls, 26 whereas most studies (n = 13) found no difference in litter size. When assessing mortality rates in rodent pups (i.e., perinatal mortality rates, total mortality rates, and percentage of successful pregnancies), four articles reported increased mortality rates in PCE pups compared with controls,33,37,41,81 and five studies found no difference in mortality.26–28,36,44,81
Several human subject studies (n = 18) have examined the relationship between PCE and overall infant health at birth. Of those, one study used Appearance, Pulse, Grimace, Activity, Respiration (APGAR) scores recorded at birth, 77 and seven used admissions to the NICU for additional care.8,46,48,53,61,73,79 At the same time, 10 included both APGAR and NICU admissions.47,52,54,57,58,60,62,66,72,74 The APGAR score is a critical tool for evaluating newborn well-being across five categories: appearance, pulse, grimace, activity, and respiration. APGAR scores were measured at 1 min to assess how well the infant tolerated the birth process, whereas the 5-min score assesses how well the infant is transitioning to life outside the womb. An APGAR score below 7 typically signals the need for further intervention. Similarly, admission to the NICU generally indicates suboptimal infant health following delivery, necessitating continued treatment. 85
Five studies reported significantly lower APGAR scores at 5 min of life among PCE infants,47,52,62,72,77 and two studies documented significantly lower APGAR scores at 1 min of life associated with PCE.47,77 However, one study identified an association between PCE and lower APGAR scores at five but not at 1 min of life. 72 Two studies reported no association between PCE and 5-min APGAR scores.57,58
Of the 18 articles examining the relationship between PCE and NICU admission, 11 reported that prenatal cannabis product use increased the risk of NICU admission, indicating poor infant health at delivery.8,46–48,52,58,61,62,66,72,73,79 However, six studies reported no association between PCE and NICU admission,8,53,54,57,68,74 and one study found that NICU admissions were the lowest among PCE infants. 66
Discussion
Among the 57 included articles (21 focused on rodents and 36 on humans), we found mixed evidence linking prenatal THC exposure to worse birth outcomes (i.e., birth weight, gestational age, mortality rate, and health at delivery). Birth weight was the most common birth outcome in rodent and human studies, providing the most consistent pattern of evidence for a significant association. Most studies have found that prenatal cannabis or THC exposure is significantly associated with lower birth weight. However, some evidence suggests that in rodents, any differences become non-significant after a postnatal catch-up period. Most of the gestational evidence indicates that prenatal cannabis or THC exposure is not associated with altered gestational age (i.e., none of the rodent studies found a significant effect, and less than half of the human studies found an association with lower gestational age). Finally, the evidence for PCE associations with mortality and health at birth is inconsistent across species. A few rodent studies have suggested that PCE increased mortality, but most studies did not find a significant effect, and litter size was largely unaffected. In human studies, infant health at delivery was generally worse, as assessed by APGAR scores and NICU admissions, in PCE infants. Still, roughly 40% of the studies did not find a significant effect. Overall, preclinical and human evidence suggest that PCE is associated with lower birth weight, and the human literature suggests poor infant health at delivery. However, the existing literature is scant, and additional research is necessary to reconcile these inconsistencies.
The inconsistency in findings may be attributed to methodological differences between human and animal models, as well as the lack of standardized procedures within each model. Animal models allow for greater experimental control, including dosage, frequency, route, and timing of THC administration, which are often unknown or less reliable variables in human literature. For example, the frequency and type of cannabis product used (e.g., smoking, edibles) have usually not been assessed in detail in human studies and typically rely on self-reporting, which is often influenced by social desirability or accuracy biases. In addition, prenatal cannabis use cannot be manipulated ethically in human subjects; therefore, evidence is solely correlational, and causal conclusions cannot be drawn. Other variables may account for significant associations and may differ between studies, such as disparities between high- and low-income geographic areas, the context of legalization within that area, and differences between retrospective chart reviews and cohort studies. Furthermore, many human studies have not considered polypharmaceutical use, including known teratogens such as tobacco and alcohol. There were also inconsistencies in the controlling variables, such as maternal age, ethnicity, education, marital status, access to quality health care, and socioeconomic status.
Although preclinical rodent studies allow for a more rigorous control, the literature highlights several methodological limitations. A notable difference between these studies is the route of THC administration. Most studies have employed oral administration, which may better reflect the human use of edible cannabis products, although dosage concentrations varied. A significant finding in rodent literature using oral administration was the impact of prenatal cannabis exposure on mortality, an effect observed exclusively in studies administering THC orally. This outcome may be attributed to the different pharmacokinetics of THC, depending on the route of administration. Beyond mortality, no other birth outcome was uniquely associated with a specific administration route. Future studies should explore the effects of various THC metabolites on neonatal survival to clarify these findings further.
In addition to the route of THC administration, the concentration and prenatal dosing period vary across rodent studies. For instance, among studies administering THC intraperitoneally (i.p.), five used a dose of 3 mg/kg, whereas two used doses of either 1 µg/kg or 0.02 mg/kg. Notably, all studies utilizing the i.p. route observed a decrease in body weight at birth, regardless of when prenatal cannabis exposure began, as all studies administered daily injections until birth. It might be helpful to examine whether this effect on body weight can be replicated with a single exposure during gestation.
For subcutaneous administration, two of the three preclinical studies used a dose of 2 mg/kg, whereas the third employed significantly higher doses of either 25 or 50 mg/kg. The results were mixed; one study using a 2 mg/kg dose reported decreased birth weight, while another found no effect. However, higher doses (25 or 50 mg/kg) were associated with a reduced litter size and body weight. Studies using subcutaneous THC were consistent in their dosing period, initiating treatment on either the 5th or 6th day of gestation and continuing until birth.
Variability in THC dosage and timing was most pronounced among studies that used oral administration. Commonly, studies have employed low (15 mg/kg) and high (30 or 50 mg/kg) doses, although individual studies have also used doses of 5, 10, or 50 mg/kg. The timing of prenatal treatment also varied, with most studies starting between days 2 and 8 of gestation or later, days 12 or 14. The observed effects of oral THC administration on birth outcomes were not dose- or time dependent. However, owing to insufficient studies employing inconsistent methodologies, firm conclusions cannot yet be drawn. These effects on birth outcomes seem to arise from a combination of the THC dose and the specific gestational period during which it is administered.
Results from human literature on the impact of prenatal cannabis use on birth outcomes remain complex and inconclusive. Although the preponderance of evidence suggests that prenatal cannabis exposure is adversely associated with lower infant birth weight and poorer health at delivery, several reviewed studies reported no significant findings. One possible explanation for these inconsistencies is the variability in the methods used to measure cannabis use across studies. Most studies (n = 16) relied solely on self-reported data from mothers regarding cannabis use during pregnancy. Other methodologies include urine toxicology screening for mothers and/or infants, meconium testing of infants, and the use of International Classification of Disease codes to identify diagnoses of cannabis use disorder. Variations in cannabis use measurement may lead to an underestimation of the prevalence of prenatal cannabis use, as some mothers may underreport their usage.
In addition, many studies have relied on a single biospecimen analysis, which may fail to capture all instances of cannabis exposure. This variability highlights the need for more standardized and comprehensive measurement techniques in future research to accurately assess the association between prenatal cannabis use and birth outcomes. Furthermore, prenatal cannabis product use within samples varied greatly between studies, ranging between 0.3% 72 and 34%. 60 These varying methodologies and conflicting results underscore the need for additional research to further explore the association between cannabis use and birth outcomes.
Most human studies have relied on a single retrospective report of prenatal cannabis use, often after childbirth. Only three of the included studies55,58,63 assessed cannabis use at multiple time points throughout pregnancy, either through questionnaires or laboratory testing. These data provide valuable insights into the use of cannabis during pregnancy and its trimester-specific effects on birth outcomes. Future research should incorporate multiple time points of cannabis testing throughout pregnancy to better understand the impact of cannabis use at distinct stages of pregnancy on infant birth outcomes. Furthermore, only four46,55,63,71 examined the dose–response relationship between cannabis use and birth outcomes. This was assessed by evaluating the frequency of prenatal cannabis use. The inclusion of dose-specific data in future research would enhance our understanding of the dose-dependent effects of prenatal cannabis use on birth outcomes.
Implications for policy and practice
Further rigorous research is necessary to better understand the effects of cannabis product use on fetal and infant health outcomes. This is a vital step in identifying the gaps in health care education and practice. In addition, it is crucial to explore the attitudes and beliefs of pregnant individuals regarding cannabis use and how these perceptions influence their health decisions.
It is equally important to examine health care providers’ perspectives on cannabis use during pregnancy, as there remains no clear consensus on its impact on fetal and infant health. A more comprehensive understanding of the dose-dependent effects of prenatal cannabis exposure, along with the attitudes, beliefs, and behaviors of both pregnant individuals and health care providers, is essential to address this uncertainty. Moreover, further research is needed to expand the safety data on prenatal cannabis use and its long-term consequences for fetal and infant development.
These insights have the potential to shape health care education, enhance provider counseling strategies, and inform policy changes regarding the marketing and availability of cannabis products, particularly for pregnant women.
Limitations
As with any study, there are limitations to the present review. Articles included in the systematic review were limited to the English language, published articles, and rodent or human studies. However, few studies have been conducted on other species. We excluded these studies to reduce inter-species differences. We also did not seek non-published studies, which may have added more non-significant findings. Finally, the effect size was generally not reported in the studies included in the review, so we cannot speak to the magnitude of the effect prenatal cannabis exposure may have on birth outcomes. Future studies should report the effect size to determine the real-world relevance of these findings. Finally, birth outcomes were limited to birth weight, gestational age, mortality, and health at delivery as these were the most common outcomes. Some studies have used other metrics (e.g., stillbirth and premature rupture of membranes), but these were often assessed in a single study. Thus, there is insufficient evidence for a review.
Conclusions
This systematic review is the first to assess the association between prenatal cannabis or THC use and birth outcomes in human and rodent studies. Overall, evidence suggests that prenatal cannabis use adversely affects birth outcomes (i.e., lower birth weight and poorer health at delivery in human infants), which has potentially negative implications for later neurodevelopment and behavior. However, the existing literature is scant, and the findings are somewhat mixed. With the increasing use of cannabis products during pregnancy, the inconsistencies observed in both animal and human studies underscore the urgent need for rigorous research to clarify the outcomes of cannabis use and inform policies and interventions that promote maternal, fetal, and infant health.
Footnotes
Acknowledgments
The authors acknowledge Enya Goonetillke for her technical support.
Author Disclosure Statement
The authors report no conflicts of interest.
Funding Information
Funding was provided by the University of Connecticut, School of Nursing, Dean's Seed Grant.