
Abstract
In this naturalistic study, we assessed the effect of sluggish cognitive tempo (SCT) symptoms in the response to methylphenidate (MPH) in 88 children and adolescents with attention-deficit/hyperactivity disorder–Inattentive Type (ADHD-I) according to Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) criteria. SCT symptoms were assessed in these subjects by means of the Child Behavior Checklist (CBCL) scale. The response to MPH after 1 month of treatment was assessed by parental scores in the Swanson, Nolan, and Pelham Questionnaire–Version IV (SNAP-IV) scale. No significant differences were found between subjects with and without SCT symptoms in the response to MPH either assessing presence of SCT symptoms categorically (at least 1 symptom) or dimensionally (p < 0.5 for both analyses; effect size [ES] = 0.24). Our findings corroborate previous phenotypic data suggesting that SCT symptoms do not define a clinically relevant type of ADHD-I.
Introduction
In the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association 1994) field trials for attention and disruptive behavior disorders, SCT symptoms were proposed as potential components of ADHD diagnostic criteria. However, such items were excluded from the final version of DSM-IV due to their poor negative predictive power for the inattention symptom group (their absence did not predict the absence of inattention) (Frick et al. 1994).
Recently, there is a growing debate on research opportunities for ADHD in the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-V) (Rohde 2008). Although recent studies have documented the high prevalence of ADHD–Inattentive Type (ADHD-I) in community samples (Woo and Rey 2005) and specific environmental and genetic correlates for this subtype (Schmitz et al. 2006a; Schmitz et al. 2006b), several investigations suggested that there is not enough evidence to support ADHD subtypes as proposed by the DSM-IV (see Rohde 2008).
In this context, there is a new resurgence of interest in SCT as a possible discriminating factor for ADHD subtypes (McBurnett et al. 2001). Some studies have examined the potential utility of the SCT symptoms as part of the diagnostic criteria for ADHD (Hartman et al. 2004; Todd et al. 2004; Capdevila-Brophy et al. 2006), but none of them has assessed the response to methylphenidate (MPH) comparing patients with and without SCT symptoms. Therefore, the objective of this study was to evaluate the prognostic validity of SCT symptoms in patients with ADHD-I by comparing two groups of ADHD-I patients (with and without SCT symptoms) in their response to treatment with MPH.
Brief Report
This is a retrospective assessment from a naturalistic study (noncontrolled cohort). Subjects were enrolled in the ADHD outpatient clinic at the Child and Adolescent Psychiatry Division of Hospital de Clínicas de Porto Alegre (HCPA). The HCPA is the university hospital of the Federal University of Rio Grande do Sul, Brazil. Data were collected during the period from January, 2000, to February, 2008. The study was approved by the Institutional Review Board (IRB) of our university hospital (approved as an IRB by the Office for Human Research Protections, United States of America–IRB 00000921).
Subjects included in this study were outpatients aged between 4 and 17 years, with a clinical diagnosis of ADHD-I based on DSM-IV criteria (American Psychiatric Association 1994). However, for the purpose of this study, we also included those who fulfilled all DSM-IV criteria for ADHD except the age-of-onset criterion (criterion C), as this criterion was not empirically derived and recent investigations have documented its lack of validity (see Reinhardt et al. 2007). To be included in the study, the subjects had to be drug naïve for MPH and had to use MPH as the primary medication for the disorder in doses equal or higher than 0.30 mg/kg per day.
The diagnoses of ADHD and co-morbid disorders for children and adolescents were based on a three-stage process, including the application of semistructured interviews Kiddie Schedule for Affective Disorders and Schizophrenia–Epidemiological version (K-SADS-E). This process was extensively described previously (see Polanczyk et al. 2003; Rohde et al. 2005).
Symptoms of SCT were retrospectively assessed through the parents' form of the Child Behavior Checklist (CBCL) (Achenbach 1991). We established the independent variable based on the CBCL questions that define Sluggishness: “being confused or lost” (question 13); “daydreaming” (question 17); “stares” (question 80) and “drowsiness” (question 102). The independent variable was defined both categorically (the presence of at least one of the four SCT questions rated as “frequently” by the parents in the CBCL) and dimensionally (total sum of the scores of SCT symptoms in the CBCL, ranging from 0 to 8). The dependent variable was the total score of the Swanson, Nolan, and Pelham Questionnaire scale–version IV (SNAP-IV) after 1 month of MPH treatment. The SNAP-IV is based on a 0–3 rating scale and has been frequently used in ADHD investigations, including those designed to assess clinical interventions (Swanson et al. 2001). The scale was completed using information gathered from the subjects' parents. Patients were evaluated for ADHD symptoms at baseline and after 1 month of treatment with the same scale. Demographic characteristics (gender, ethnic background, and age) were collected by direct interview. Intellectual functioning was measured in children and adolescents by the Wechsler Intelligence Scale–Third edition (WISC-III) (Wechsler et al. 1991) administered by trained psychologists to assess the full-scale intelligence quotient (IQ) score.
Patients were treated according to the program's protocol. Doses of short-acting MPH were augmented until there was no further clinical improvement or there were limiting side effects (Polanczyk et al. 2007b). MPH was administered preferentially twice daily (8 a.m. and noon), but an extra dose at 5–6 p.m. was allowed for children needing continuous coverage in the evening. The minimum dose of MPH accepted in this protocol was 0.30 mg/kg per day. Concomitant use of other medications was allowed.
The definition of potential confounders was based on conceptual analyses of the literature and a broad statistical definition (association with both the independent and dependent variables, considering a p ≤ 0.20). This approach assured very conservative analyses. Baseline demographic characteristics (age, gender, ethnicity, and socioeconomic status), IQ, co-morbid conditions (disruptive behavior disorders, anxiety, and mood disorders), baseline SNAP-IV scores, doses of MPH, and use of a second medication were compared between the two groups (with SCT symptoms and without SCT symptoms) using the chi-squared test or Fisher exact test (categorical variables), and the Student t-test (continuous variables). We also determined the association between all the above-mentioned variables and response to MPH (dependent variable). The effect of the SCT symptoms on the SNAP-IV total score at 1 month of treatment was assessed through analysis of covariance (ANCOVA) with baseline scores and potential confounders as covariates. A 5% significance level was accepted in all these comparisons (two-tailed). An unbiased estimate of the effect size (ES) was also computed for the total score of the SNAP-IV (pretreatment mean score - 1-month mean score/pooled standard deviation [SD]). An ES < 0.80 was considered large, between 0.50 and 0.80 was considered moderate, and >0.20 was considered small.
From a total sample of 148 children and adolescents with ADHD-I who were enrolled in the ADHD Outpatient Program during the study period and who fulfilled our inclusion/exclusion criteria, we were able to include 88 (59.4%) subjects for analyses (see Fig. 1). We compared patients included and not included on demographic characteristics (age, gender, ethnicity, and socioeconomic status), IQ, co-morbid conditions (disruptive behavior disorders, anxiety, and mood disorders), SNAP-IV scores at baseline, doses of MPH, and use of a second medication. No significant between-group difference was found.
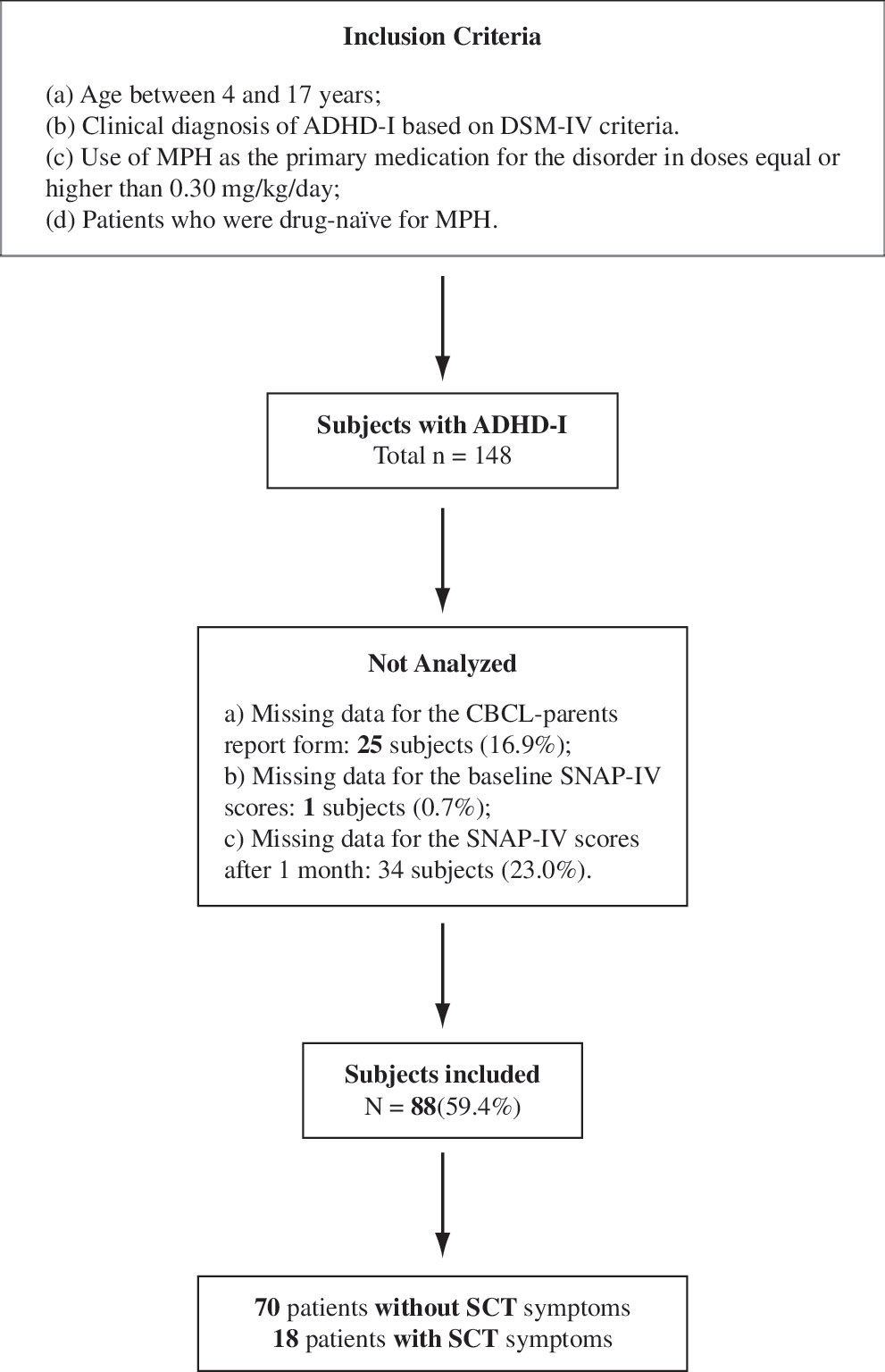
Flow chart for this naturalistic study. ADHD-I =Attention-deficit/hyperactivity disorder–Inattentive type; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, 4th edition; MPH = methylphenidate; CBCL = Child Behavior Checklist; SNAP-IV = Swanson, Nolan, and Pelham Questionnaire–Version IV; SCT = sluggish cognitive tempo.
The demographic characteristics, IQ, co-morbidities, dose of MPH, and scores in the SNAP-IV scale for subjects included in the study can be found in Table 1. The only between-group significant difference was detected in gender. The fact that the gender breakdown has been different in our sample—more girls in the SCT group—might indicate that this subgroup of ADHD-I type represents an even more refined subtype.
Mean and SD reported for continuous variables; n and percentage reported for categorical variables.
p < 0.05; no other variables were significantly different between groups.
Abbreviations: IQ = intelligence quotient; MPH = methylphenidate; SNAP-IV = Swanson, Nolan, and Pelham questionnaire–version IV; ADHD-I = attention-deficit/hyperactivity disorder–inattentive type; SCT = sluggish cognitive tempo; ODD = oppositional defiant disorder; CD = conduct disorder.
Subjects with and without SCT symptoms did not have a significantly different SNAP-IV total score after 1 month of MPH treatment (F = 13.410; degrees of freedom [df] = 2; p = 0.524), after controlling for baseline SNAP-IV scores (no other potential confounders were selected for this analysis). To confirm these findings, we also ran an ANCOVA with SCT symptoms treated as a dimensional—the total sum of the scores in the four CBCL items related to the SCT (possible range, 0–8). In this analysis, opposition defiant disorder (ODD) and the baseline total score for the SNAP-IV were the only confounding variables that survived our threshold. No significant effect was found for SCT symptoms on the response to MPH (F = 5.657; df = 8; p = 0.660). Additionally, we ran logistic regression analyses using a clinical cutoff score indicating a moderate response to treatment in ADHD naturalistic trials (reduction ≥ 50%; see Spencer et al. 1996). Subjects with and without SCT symptoms again did not present a significant difference in the response to treatment with MPH (odds ratio [OR] = 2.7; 95% confidence interval [CI] = 0.85–8.67), after controlling for age and baseline SNAP-IV scores (the only confounders for this analysis). In addition, we ran analyses considering symptoms as a dimensional variable and the results were similar (OR = 1.02; 95% CI = 0.76–1.35), after controlling for potential confounder (ODD, age, and baseline SNAP-IV scores). Finally, we assessed the effect size from the between-group comparison for the total score of the SNAP-IV at 1 month. Only a small, nonclinically significant effect size was detected (ES = 0.24).
More than 30 years ago, Robins and Guze (1970) proposed a strategy for assessing the validity of diagnostic constructs in psychiatric disorders that has been used in several investigations. Regarding psychiatric disorders of childhood and adolescence, Jensen et al. (1997) adapted the strategy including eight criteria: Clinical phenomenology; demographic, psychosocial, and biological factors; family genetics and environmental factors; natural history; and intervention response.
Although, as stated above, medication response solely is not the gold standard for validating diagnostic criteria (even more so in a dimensional disorder like ADHD), our findings corroborate previous phenotypic data suggesting that SCT symptoms do not define a clinically relevant type of ADHD-I. For example, Todd et al. (2004), measuring the impact of including SCT items on the factor and latent class structure of ADHD subtypes, demonstrated that the inclusion of SCT symptoms (“daydreams” and “low energy”) does not support the presence of additional discrete subtypes. These SCT symptoms do not discriminate a specific subgroup when analyzed together with the 18 DSM-IV symptoms. Moreover, ours is the first study that evaluates whether or not the SCT symptoms are associated with a different response to treatment in patients with ADHD-I.
The results reported in this study must be interpreted in the context of some methodological limitations. First, it is important to note that we only addressed symptomatic short-term response to treatment with MPH, and the absence of differences on this measure alone does not necessarily indicate that the subgroups demonstrate similar treatment responses on other clinically relevant measures. Second, we were not able to analyze data from 40.6% of eligible subjects. However, we extensively assessed a huge number of potential confounding factors and no variable was significantly different between patients included and those not included in this protocol. Third, our definition of the presence or absence of SCT was arbitrary, based on four symptoms of the CBCL scale. It is important to note that there is no consensus on how to establish the best symptomatic pattern to capture the SCT construct and our approach included most of the SCT symptoms described in the majority of the few studies conducted on this issue (McBurnett et al. 2001; Hartman et al. 2004; Todd et al. 2004). Fourth, we did not have an internal control to correct for any effect of time or expectancy bias because we did not have a placebo arm in this study. However, the improvement of ADHD symptoms was comparable to those previously reported in randomized clinical trials, and there is no conceptual reason to expect a specific interaction between time/expectancy with group status (with or without SCT symptoms). Finally, although this is the first study to evaluate MPH response in this subgroup of patients, we cannot exclude a type II error (false negative) due to our small sample size of subjects with SCT symptoms. Therefore, the current study provides an interesting, but initial, finding suggesting that the presence of these SCT symptoms may not alter the response to treatment with MPH in patients with ADHD-I.
Footnotes
Disclosures
Dr. Rohde was on the speakers' bureau and/or acted as consultant for Eli-Lilly, Janssen-Cilag, and Novartis in the last 3 years. Currently, his only industry-related activity is taking part of the advisory board/speakers bureau for Eli Lilly and Novartis (less than US$ 10,000 per year and reflecting less than 5% of his gross income per year). The ADHD and Juvenile Bipolar Disorder Outpatient Programs chaired by him received unrestricted educational and research support from the following pharmaceutical companies in the last 3 years: Abbott, Bristol-Myers Squibb, Eli-Lilly, Janssen-Cilag, Novartis, and Shire. Mr. Ludwig, Mr. Matte, and Mrs. Katz have no conflicts of interest or financial ties to disclosure.