
Abstract
Background:
Children and adolescents are being treated increasingly for attention-deficit/hyperactivity disorder (ADHD) with a variety of stimulants in higher than Food and Drug Administration (FDA)–approved doses and in combination with other medications.
Objective:
We sought to determine methylphenidate (MPH) concentrations in children and adolescents treated with high-dose, extended-release osmotic release oral system (OROS) MPH plus concomitant medications, and to examine MPH concentrations with respect to the safety and tolerability of treatment.
Methods:
Plasma MPH concentrations were measured by liquid chromatography–mass spectrometry 4–5 hours after administration of medication in a sample of youths diagnosed with ADHD. These youths were treated naturalistically with higher than FDA-approved doses of OROS MPH in addition to their concomitant medications. Markers of safety and tolerability (e.g., measures of blood pressure and heart rate) were also examined.
Results:
Among the 17 patients (with a mean age of 16.2 ± 2 years and a mean number of concurrent medications of 2.23 ± 0.94), the mean plasma MPH concentration was 28 ± 9.1 ng/mL, despite a mean daily dose of OROS MPH of 169 ± 5 mg (3.0 ± 0.8 mg/kg per day). No patient had a plasma MPH level ≥50 ng/mL or clinical signs of stimulant toxicity. No correlation was found between plasma MPH concentrations and OROS MPH dose or changes in vital signs.
Conclusions:
High-dose OROS MPH, used in combination with other medications, was not associated with either unusually elevated plasma MPH concentrations or with clinically meaningful changes in vital signs. Study limitations include a single time-point sampling of MPH concentrations, a small sample size, and a lack of outcome measures to address treatment effectiveness.
Introduction
One such preparation, osmotic release oral system (OROS) MPH is a once-a-day formulation of MPH that has an efficacy and tolerability profile comparable to that of three times-a-day immediate-release MPH (Pelham et al. 2001; Wolraich et al. 2001; Swanson et al. 2004). In both 1- and 2-year open follow-up studies, OROS MPH has been well tolerated with few clinically significant adverse effects (e.g., tics, vital sign abnormalities, laboratory test abnormalities, or inhibition of growth) (Wilens et al. 2003; Wilens et al. 2005).
On average, there is a linear relationship between the MPH dose and the reduction of ADHD symptoms (Pliszka et al. 2007). However, the relationship between MPH dose and clinical efficacy can vary widely among individual patients (Markowitz et al. 2003a). Stimulant dosing remains largely empirical, yet informed by dosage guidelines from the U.S. Food and Drug Administration (FDA) and clinical practice parameters (Greenhill et al. 2002). For children and adolescents, the FDA recommends maximum daily MPH doses of up to 60 mg/day for short-acting forms and 72 mg/day for extended-release preparations; others recommend up to 2 mg/kg/day of racemic MPH (Biederman et al. 2006a). In clinical practice, these guidelines often prove troubling. For example, a 140-pound adolescent with ADHD treated according to the 2-mg/kg guide has an implied maximum MPH dose of 125 mg daily, a figure that is more than twice the FDA-approved maximum. Moreover, little is known about dosing in the context of use of concomitant medications.
With the exception of case reports (e.g., Lipkin et al. 2003) and studies of toxicity with pediatric MPH exposure (Klein-Schwartz 2003), little is known about the use of higher than FDA-approved doses of MPH, especially in youths. In adults, Biederman and colleagues (2006b) showed that symptoms of ADHD in 141 patients were reduced with a mean daily dose of 87 mg of the OROS formulation. Over the course of this 6-week study, higher doses of OROS MPH were well tolerated but were associated with small yet statistically significant increases in systolic blood pressure (SBP), diastolic blood pressure (DBP), and heart rate. A study of 11 adults chronically treated with ≥100 mg/day of MPH for narcolepsy (with a mean daily dose of 198.2 ± 127.9 mg) found no worsening of hypertension. Furthermore, cases of treatment-emergent psychosis arose only when there was pretreatment paranoia or a family history of psychosis (Pawluk et al. 1995).
Given the paucity of information available on use of high-dose MPH in youths, several questions remain unanswered. For example, do higher doses of MPH result in correspondingly elevated blood concentrations of MPH? Are high doses of MPH associated with elevations in blood pressure and pulse? Therefore, we sought to determine whether higher than FDA-approved doses of extended-release MPH, in the context of use of other medications, were associated with unusual elevations of MPH plasma concentrations or with adverse cardiovascular effects. On the basis of literature indicating relatively poor and variable bioavailability of MPH (Patrick and Markowitz 1997), including OROS MPH (Markowitz et al. 2003b), we hypothesized that patients treated with higher than FDA-approved doses of OROS MPH would have plasma MPH concentrations that were within the range of concentrations reported to be therapeutic for ADHD.
Methods
Patient sample
Patients included for analyses were children and adolescents treated with higher than FDA-approved doses of OROS MPH (i.e., greater than 72 mg daily) by a senior child and adolescent psychiatrist (R.G.) in the Beaverton, Oregon, area (between December, 2006, and August, 2007). Patients were treated in both residential treatment (Pendleton Academy, Pendleton, Oregon) and outpatient settings in a naturalistic fashion for their psychiatric presentation. Patients treated with concurrent medications were not excluded from analysis. All patients were diagnosed with ADHD (Predominantly Inattentive Type, Predominantly Hyperactive-Impulsive Type, or Combined Type) as defined by the criteria in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association, 1994). Plasma MPH concentrations were drawn from boys and girls to safeguard patient safety in the absence of clear guidelines for clinical monitoring of patients receiving higher than FDA-approved doses of MPH. The residential treatment center Institutional Review Board (IRB) approved the retrospective review and analysis of the data.
Two patients in our sample were overweight (weight >95th percentile for his or her age). All patients were otherwise healthy (by history, physical examination, and basic laboratory monitoring indices).
Blood sampling and analysis of plasma MPH concentrations
Plasma MPH levels were assessed in those who had been maintained on a stable dose of OROS MPH for at least 2 weeks; concentrations were drawn between 4 and 5 hours after morning administration of the medication. Some (Markowitz et al. 2003b), though not all (Modi et al. 2000), pharmacokinetic studies have shown that OROS MPH has plateau concentrations at 3.3 and 6 hours after administration. Approximately 3 mL of venous blood were drawn from each patient into EDTA vacutainer tubes. The blood samples were processed immediately by centrifugation and were stored at approximately −20°C before frozen shipment on dry ice for laboratory analysis. Blood samples were analyzed by high-performance liquid chromatography with tandem mass spectrometry (HPLC/MS) at two laboratories. Fourteen out of 17 samples (82%) were analyzed at Medtox Scientific, Inc (St. Paul, MN); three samples (18%) were analyzed at Quest Diagnostics–Nichols Institute (San Juan Capistrano, CA). At both facilities, the lower limit of quantification (LLOQ) for the assay was 1 ng/mL. At Medtox Scientific, Inc., the intrarun precisions (relative standard deviation (RSD)) were 2.2% at 3 ng/mL and 2.6% at 20 ng/mL (n = 5). The interrun precisions were 2.6% at 3 ng/mL and 2.2% at 20 ng/mL (n = 15). At Quest Diagnostics–Nichols Institute, the intraday precisions (RSD, n = 10) were 9.4% at 5 ng/mL, 6.1% at 25 ng/mL, and 6.9% at 70 ng/mL. The interday run precisions (RSD) were 9.7% at 5 ng/mL (n = 60), 8.4% at 25 ng/mL (n = 50), and 10.4% at 70 ng/mL (n = 50). Measured MPH concentrations represent total MPH values (i.e., combined l-MPH and d-MPH isomers).
Statistical analysis
Correlation was used to determine whether there was an association between plasma MPH concentration and vital signs abnormalities or an association between MPH dose and plasma MPH concentration. t-Tests were used to determine whether there were differences between separate classes of concomitant medication (e.g., selective serotonergic reuptake inhibitors [SSRIs], lithium, or atypical antipsychotics) and plasma MPH concentrations. An alpha-level of 0.05 was used to assert statistical significance; all statistical tests were two-tailed. We calculated all statistics using Microsoft Excel.
Results
Eighteen youths with ADHD who received higher than FDA-approved doses of OROS-MPH were identified; 1 patient was not included because of concerns about poor medication adherence. Therefore, 17 youths were included in the analysis. Basic demographic information and characteristics of the sample are shown in Table 1. The mean age of the sample was 16 years, with a range of 11–20 years. The most common co-morbid disorder with ADHD was a mood disorder followed by pervasive development and oppositional disorders.
Abbreviations: ADHD, Attention-deficit/hyperactivity disorder; SD, standard deviation.
Information regarding psychiatric medication other than MPH used by the sample is shown in Table 2. All patients were receiving concomitant psychotropic medication during the evaluation period. Bupropion, SSRIs, and lithium were the most commonly co-administered medications with OROS MPH. The mean number of co-medications used by each patient at the time of MPH plasma testing was 2.23 ± 0.94.
Not mutually exclusive.
Abbreviations: SSRI, selective serotonin reuptake inhibitors.
The mean total daily dose of OROS MPH was 169 mg/day ± 31 mg/day (range, 126–270 mg/day) or 2.97 ± 0.76 mg/kg per day (range, 1.13–4.21 mg/kg per day). The mean plasma concentration of OROS MPH was 28.0 ± 9.1 ng/mL (range, 15.5–49.0 ng/mL). The distribution of plasma OROS MPH levels in our sample is presented in Fig. 1. We failed to find any association between the MPH dose and plasma MPH concentration (r 2 = 0.09, p = not significant [N.S.]).
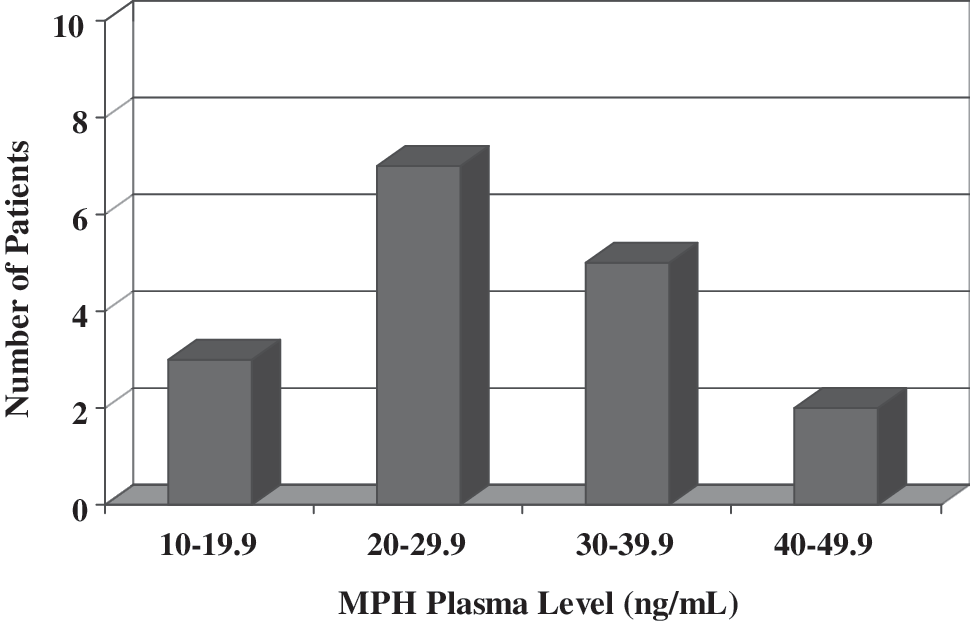
Frequency distribution of plasma methylphenidate (MPH) concentration in attention-deficit/hyperactivity disorder (ADHD) patients.
We examined the relationship between plasma MPH concentrations and the effect of different classes of concomitant medication. There was no association between any individual class of concomitant medication (e.g., bupropion, SSRIs, lithium, or atypical antipsychotics) and plasma MPH levels (all p values N.S.).
No serious adverse effects or adverse cardiovascular outcomes occurred during the evaluation period (i.e., during the inpatient hospitalization). There was no association between OROS MPH concentration and various cardiovascular effects including SBP (r 2 = 0.05), DBP (r 2 = 0.04), and heart rate (r 2 = 0.00; all p values N.S.) (Fig. 2).
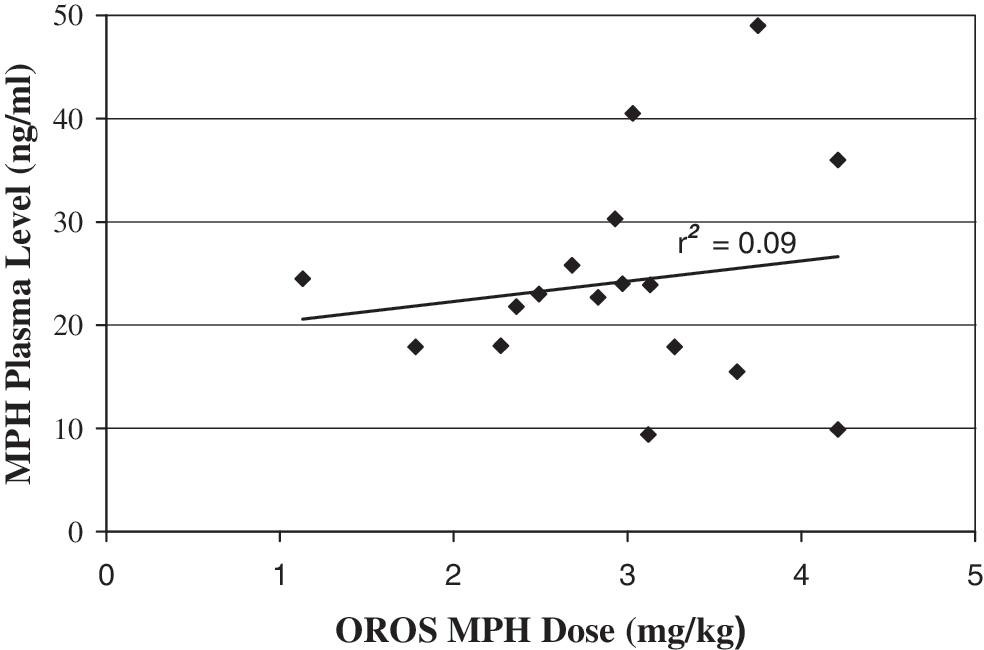
Scatter plot of Osmotic Release Oral System methylphenidate (OROS MPH) dose by plasma level in attention-deficit/hyperactivity disorder (ADHD) youths.
Discussion
To our knowledge, this is the first systematic examination of high-dose OROS MPH (>72 mg/day) in youths treated naturalistically with concomitant medication. In this small patient sample receiving higher than FDA-approved doses of extended-release MPH, the OROS formulation was well tolerated; no clinically meaningful vital sign abnormalities were observed in this medically healthy group. Moreover, high-dose OROS MPH treatment resulted in plasma MPH concentrations that were similar to those found in patients with ADHD taking other modified-release MPH formulations, such as the MPH transdermal system. In fact, plasma MPH concentrations in the current study (mean, 28.0 ± 9.1 ng/mL; range, 15.5–49.0 ng/mL) were lower than those recently reported with transdermal MPH using FDA-approved doses. For example, in a sample of 8 children with ADHD treated with 30 mg/9 hours of transdermal MPH, Pierce and colleagues (2008) found peak d-MPH concentrations [Cmax] of 46.5 ± 27.3 ng/mL, with no reports of adverse effects suggestive of major toxicity in this study group. Another example, involving phase III trials of 6-week treatment with the transdermal MPH system, showed that the mean Cmax values of d-MPH in children (ages 6–12 years) was 39 ng/mL (range, 0–114 ng/mL) (Daytrana [packet insert], 2008). These mean peak concentrations varied inversely by age ranging from 25 ng/mL (range, 2–80 ng/mL) in 12 year olds, to 53 ng/mL (range 18–83 ng mL) in 6 year olds.
Transdermal MPH systems appear to avoid the first-pass metabolism of oral dosage forms and exposure to the preponderance of hepatic carboxylesterase-1A1 (CES1), the primary enzyme involved with MPH metabolism. Although MPH from transdermal origins is eventually hydrolyzed by hepatic CES1, the continual release of MPH through the skin over a day's wear time supplies a steady release of racemic MPH into the general circulation (Markowitz and Patrick 2008; Pierce et al. 2008). In contrast, orally administered MPH, including the OROS formulation, has low bioavailability (between 20% and 30%) and undergoes extensive presystemic metabolism through hydrolysis/de-esterification with limited oxidation (Patrick and Markowtiz 1997; Markowitz et al. 2003b). Although it is unclear why patients in our sample had MPH levels within a range observed in previous clinical trials of MPH for ADHD patients, we suspect that the variable bioavailability of oral MPH may be involved.
There were a number of important methodological limitations to our study. We drew a single blood sample from each patient, which represents neither classical serial sampling nor method-driven population pharmacokinetic sampling. We used a postdosing testing period (i.e., 4–5 hours after dose administration) that is not universally accepted as representing the period of peak MPH concentration. This testing period cannot be assumed to be a reliable plateau because some formal pharmacokinetic studies have indicated that MPH blood concentrations may continue to rise during this phase (Modi et al. 2000). MPH plasma analyses were completed in two different laboratories. No outcome data were systematically collected using rating scales limiting our ability to comment on the effectiveness in this series. Other limitations included the small size of the sample, the retrospective nature of the analysis, high rates of psychiatric co-morbidity, and the naturalistic design including the simultaneous use of multiple psychotropics among the patients involved. In our sample, nearly half of patients (47%) had co-morbid depressive disorders and more than half were treated with bupropion or SSRIs. Despite the clinical heterogeneity of our sample, we felt that these patients were indicative of those treated in actual clinical practice in light of the frequent co-morbidity of ADHD with other psychiatric disorders and use of combined pharmacotherapy.
One of the primary clinical rationales for this study of high-dose MPH dosing regimens was the paucity of literature on this subject in youths, particularly as it related to objective plasma MPH concentrations and other tolerability outcomes. One of the objectives was to better assess the potential risk of peripheral and central nervous system (CNS) toxicity, in this case, using a commercially available assay to determine plasma MPH concentrations. However, the definition of a therapeutic or, conversely, a “toxic” MPH plasma concentration is not well established because reference ranges can often vary among commercial laboratories. In general, MPH concentrations reported to be “therapeutic” or in the “normal range” may be based on pharmacokinetic studies performed using normal volunteers. Similarly, elevated or “toxic” concentrations may find their origins in the toxicology literature, reflecting values from animal studies, case reports, postmortem data, or intentional overdoses (frequently involving other coingested medications) (Markowitz et al. 1997). Thus, drug concentration data drawn from these sources may assign a much lower concentration than is actually toxic or lethal. In sum, the subject of defining therapeutic and/or toxic MPH plasma ranges remains poorly understood and warrants further investigation.
Data from controlled trials indicate that 25%–35% of patients with ADHD receiving stimulants are either nonresponders or are intolerant of treatment when prescribed within traditional dosing guidelines (Wilens and Spencer 2000). Untreated or partially treated ADHD may lead to academic underachievement, poor interpersonal relationships, and low self-esteem (Swanson et al. 2004). While switching regimens is one strategy for managing ADHD, some clinicians may instead choose to increase MPH beyond FDA-approved dosages when patients have symptoms that are partially treated at the recommended maximum daily doses (Pliszka et al. 2007).
Previous authors have shown that expected physiological changes from MPH use may include an increase in blood pressure and pulse rate, and the release of corticotropin-releasing factor, corticotropin, and cortisol (Camí and Farré 2003). However, in cases of overdose, MPH may cause insomnia, irritability, aggressive behavior, and psychosis (e.g., paranoia). Medical complications of MPH intoxication include an altered mental status, autonomic instability (e.g., hyperthermia), seizures, or development of a serotonin syndrome (Caplan et al. 2007). It is notable that we did not observe clinically meaningful changes in blood pressure or heart rate in the current study, nor did we see evidence of CNS toxicity. Side effects in this study (e.g., blood pressure and heart rate changes) were similar to those reported in short- and longer-term studies of OROS MPH (Wilens et al. 2003; Wilens et al. 2005). MPH-associated morbidity is best avoided by cautious dosing of MPH when in supratherapeutic range, frequent monitoring of potential side effects, and consideration of obtaining plasma levels at the maximum approved dose for a particular preparation of MPH.
We did not find evidence of pharmacokinetically relevant drug interactions with MPH with many commonly used psychotropics. Combined medication regimens for youth with ADHD are often employed for co-morbid psychopathology (Tourette's Syndrome Study Group 2002; Findling et al. 2007; Palumbo et al. 2008), as well as for the treatment of stimulant-induced adverse effects (Wilens et al. 1995). Our naturalistic data suggest that these medications appear to be safely co-administered with MPH and none appears to grossly elevate MPH concentrations above typical concentrations observed in formal pharmacokinetic studies of the OROS formulation. Although our study was not designed to rule out possible drug–drug interactions, our data are consistent with growing literature indicating a paucity of known pharmacokinetic drug-interactions with MPH (Zhu et al. 2008). Further studies evaluating MPH concentrations prior to and in combination with other psychotropics are necessary to more accurately examine drug–drug interactions and before making formal recommendations about combination therapy.
Despite methodological limitations, our study suggests that in patients receiving higher than FDA-approved dosing of OROS MPH with concomitant psychotropics, plasma MPH concentrations were within the range of concentrations reported to be therapeutic for ADHD. Clinically, plasma concentrations may be useful to help guide treatment in patients requiring higher-than-approved dosing of MPH, particularly in the context of combined regimens. Further studies are needed to confirm the pharmacokinetic profile, bioavailability and metabolism profile, efficacy, and tolerability of high-dose MPH dosing strategies.
Footnotes
Disclosures
Dr. George is a speaker for McNeil, Shire, Novartis, and Lilly and a consultant to McNeil and Shire. Dr. Wilens receives grant support from Abbott, McNeil, Lilly, Merck, and Shire; is a speaker for Lilly, McNeil, Novartis, and Shire; and is a consultant for Abbott, McNeil, Lilly, NIH (NIDA), Novartis, Merck, and Shire. Dr. Stevens, Dr. Stern, and Mr. Fusillo have no conflicts of interest or financial ties to disclose.
Acknowledgments
The authors gratefully acknowledge Karen Conant-Norville, B.S.N., M.N., and Bridget Gessler, R.N., PMHNP, for their invaluable assistance with patient care and data monitoring. We would like to thank Marykate Martelon for her assistance with statistical analysis.
The data analysis of this research was funded by institutional funds from the Pediatric Psychopharmacology Unit at Massachusetts General Hospital.