
Abstract

Referring to those findings, we would like to describe the case of a 13-year-old girl with generalized anxiety disorder who was treated with 75 mg of fluvoxamine. Four months after introducing pharmacotherapy, the patient complained of irregular heartbeats. A standard 12-lead electrocardiogram showed sinus rhythm, 99–110/minute; PQ, 140 msec; QRS, 80 msec; QTc interval prolongation varying between 460 msec and 490 msec (based on Bazett`s correction formula; Bazett 1920) (Fig. 1). Measurement of the QT interval was performed in all leads. The end of the T wave was determined by both baseline (the visual return of the T wave to the baseline level) and tangent (the intersection of tangent to the steepest slope of the last limb of the T wave with the baseline) (Lepeschkin and Surawicz 1952). No arrhythmia was found in electrocardiogram (ECG) and 22-hour Holter monitoring. Serum sodium, potassium, and calcium levels were within the normal limits (138 mmol/L, 4,0 mmol/L, 5.1 mEq/L, respectively), but the magnesium level was 1.5 mg/dL (norm, 1.6–2.3 mg/dL). The dose of fluvoxamine was reduced to 50 mg, and QTc interval prolongation was no longer observed (Fig. 2).
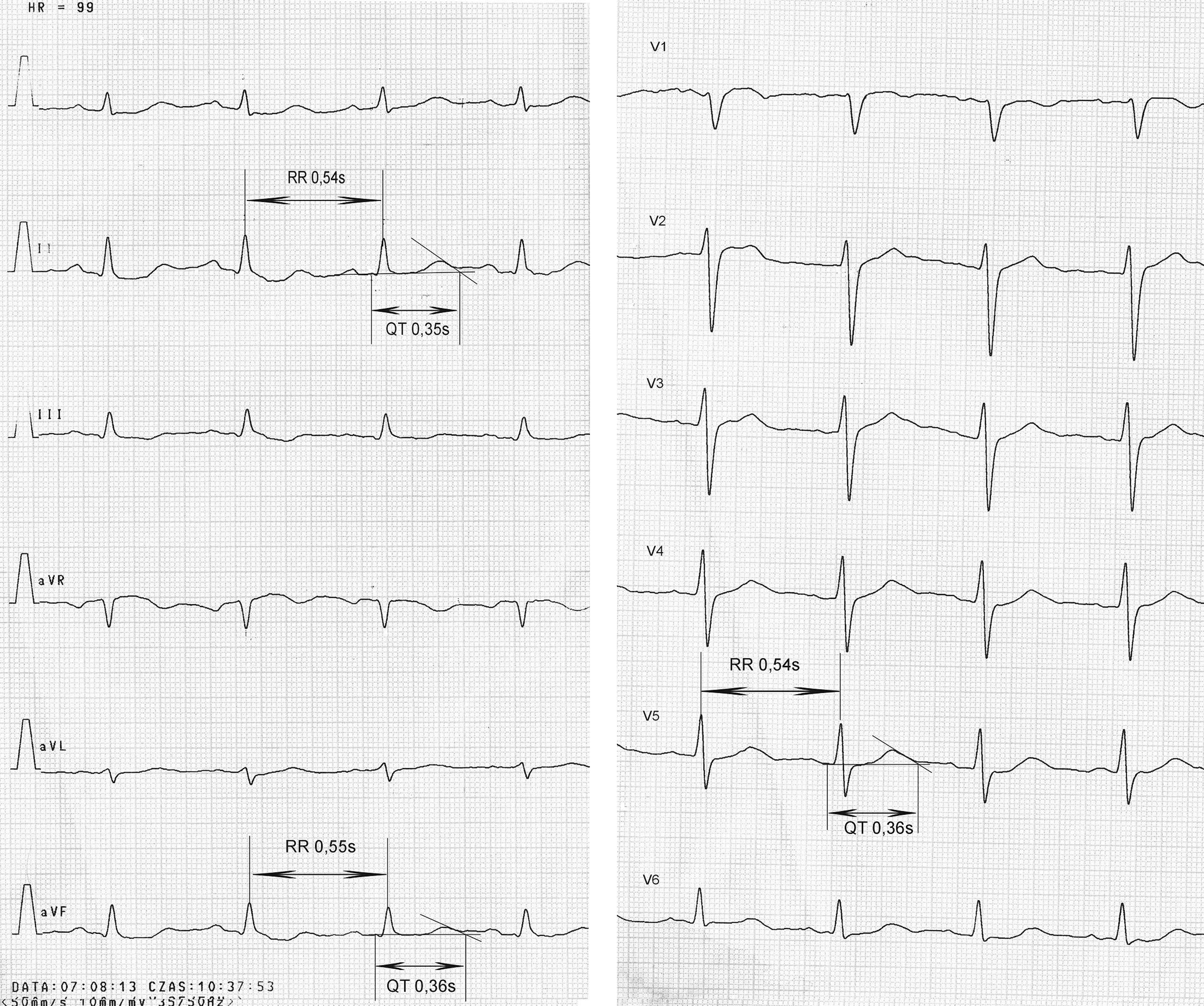
Electrocardiogram (ECG) from the patient during treatment with fluvoxamine (dose 75 mg/day).

Electrocardiogram (ECG) from the patient treated with fluvoxamine (dose 50 mg/day).
Apart from very mild hypomagnesemia that could contribute to QTc prolongation, other risk factors (cardiac, endocrine, metabolic disorders, concomitant medications, and long QT syndrome [LQTS]) have been excluded. Another explanation of the QTc prolongation phenomenon could be fluvoxamine's action. If so, there appears to be a striking dose effect. The prolongation occurred during treatment with a relatively low dose of fluvoxamine.
Until now, those abnormalities of QT interval observed have been due to fluvoxamine overdose (Solvay Pharmaceuticals). In our case, plasma concentration of fluvoxamine was not examined. Overdose was not suspected. Consecutive ECGs performed during 1.5-year follow-up (without pharmacological treatment) were within normal limits (QTc 400–420 msec).
To our knowledge this is the first case report concerning QTc prolongation in a patient treated with a therapeutic dose of fluvoxamine. No reports exist of fluvoxamine-induced QTc interval prolongation or torsade de pointes.
Footnotes
Disclosures
Drs. Brzozowska and Werner have no financial ties or conflicts of interest to disclose.