
Abstract
Aim:
The objective of this study was to evaluate predictors of long-term adherence to treatment with methylphenidate (MPH).
Methods:
A total of 134 children (ages 4–16) with a diagnosis of attention-deficit/hyperactivity disorder (ADHD) determined by specific protocols, including a semistructured parent interview, Conners' Teacher/Parent Rating Scales, cognitive and learning evaluation, and child self-reports for anxiety and depression, were assessed monthly for up to 36 months. At the end of the study (36 months), three outcomes were evaluated (continuing medication, medication withdrawn due to functional remission, and medication withdrawn for other reasons including poor compliance). Outcomes were first analyzed by mean of the chi-squared test, Mann–Whitney-U test, or t-test, and predictive models were subsequently generated using Cox proportional hazards model analysis. Age, ADHD subtype, co-morbidity, cognitive functioning, side effects, and family and social characteristics were considered as independent variables.
Results:
Thirty-six months after starting MPH, 62 children (46%) were still on treatment, 32 (24%) had stopped MPH due to functional remission, and 40 (30%) had suspended MPH for other reasons. Within the last group, 20 suspended for poor compliance, 10 for decrease of efficacy, 5 for side effects, and 5 because they entered in an atomoxetine clinical trial. The presence of associated disorders, younger age, female gender, and not living with both parents were predictors for continuing medication until end of the study (36 months); absence of associated disorders and older age were predictors of discontinuation medication due to functional remission before the end of study, older age, and hyperactive subtype were predictors of discontinuing medication for other reasons.
Conclusion:
Clinical outcome of ADHD treatment is heterogeneous: Specific clinical and social predictive parameters for long-term MPH use and compliance can be identified. An accurate tailoring of clinical intervention to the individual child appears crucial for good outcome.
Introduction
Because of the long-term nature of the treatment and the need for multiple doses of MPH, poor adherence turns out to be a crucial issue in the treatment of ADHD. Social stigmatization, privacy, inconvenience, and diversion of MPH are potential problems. Parents often think that taking drugs at school can embarrass their child and hurt his self-esteem (Pelham et al. 2001; Swanson 2003). Extended-release forms of MPH have been developed in the recent years to overcome these limitations of classical formulations. The National Institute for Clinical Excellence (NICE) found little difference in efficacy between multiple doses of immediate-release MPH and single doses of long-acting formulations (
Significantly different estimates of children and adolescent persistence with immediate-release formulations medication have been reported. In clinical research samples, reported persistence rates range from 53–81% after 1 year to 36–46% after 5 years (McBride 1988; Barkley et al. 1990; Thiruchelvam et al. 2001; Charach et al. 2004; Barbaresi et al. 2006). More recently, the Multimodal Treatment Study of Children with ADHD (MTA) study reported that 70% of children under intensively managed medication for 14 months (Med and Comb groups) were still on medication 3 years after randomization (about 2 years after the end of the intensive drug management) (Jensen et al. 2007). Retrospective, population-based studies, on the other hand, showed that after excluding patients with a prescription duration of less than a week, persistence on treatment after 1 year was approximately 15%; less than 50% of the patients continued medication for more than 3–10 months and less than 20% continued medication for at least 1 year (Firestone 1982; Marcus et al. 2005).
Studies on persistence suggest that predictors of poor adherence to medication may include older age (Thiruchelvam et al. 2001; Gau et al. 2006), male gender (Firestone 1982), lower intelligence quotient (IQ) (Firestone 1982; Brown et al. 1985), more severe ADHD (Charach et al. 2004), oppositional-defiant symptoms (Thiruchelvam et al. 2001), lower socioeconomic status (Ibrahim 2002), and three-times-daily regimen (Gau et al. 2006).
In Italy neither MPH, dextroamphetamine, nor atomoxetine was available on the market until March, 2007. Only recently did the Italian Drug Regulatory Agency approve the use of immediate-release MPH and atomoxetine under controlled prescription based on ADHD diagnosis, with staging performed at reference centers and 2-year follow-up at the prescribing center (Panei et al. 2004). At the time of the study (1998–2005), we were able to import immediate-release MPH from abroad after formal approval by the National Ministry of Public Health. After prescribing, medication was dispensed at our Hospital Pharmacy on a monthly schedule.
Previously, we have shown that the Diagnostic and Statistical Manual of Mental Disorders (DSM) taxonomy for developmental disruptive behaviors displays a construct validity independent from parent and teacher awareness for specific categorical disorders and from predominant clinical attitudes of professionals (Zuddas et al. 2006). Former and current restrictions on the availability of psychostimulants, together with a relatively poor parent and teacher awareness of ADHD, make Italy an interesting environment in which to identify sociodemographic and clinical predictors of duration and compliance to a long-term treatment with immediate-release MPH.
The aim of the study was to verify whether, in an intensive system of care with strict medication management, age at medication onset, severity, co-morbidity, cognitive level, family structure, and school support among other variables may predict clinical outcome and persistence of stimulants treatment.
Methods
Participants
All 187 participants receiving an ADHD diagnosis Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association 1994) criteria, taking at least one dose of MPH, between 1998 and 2005 at the Centre for Pharmacological Therapies in Children and Adolescent Psychiatry, an outpatient Clinic of the Cagliari University Hospital, University of Cagliari, Sardinia (Italy), were considered in the present study.
Fifty-three patients did not start chronic treatment after the test dose because of following reasons: Severe side effects (defined as dysphoria/irritability, logorrhea, persistent involuntary movement or over focusing, n = 12), because of lack of symptom improvement after at least one week of treatment (n = 10), or according to parental decision, immediately after test doses or during the first 2 weeks of treatment (n = 31). These patients were excluded from the study.
The medical charts of the 134 remaining ADHD children and adolescent taking MPH for at least 1 month were reviewed retrospectively to record their clinical history up to 36 months of monthly follow-up.
Diagnostic procedure and assessment measures
For all patients, the Conners' Teacher and Conners' Parent Rating Scales–Revised (CT/PRS-R) (Conners 1997) were used to collect information from teachers and parents. The Parent Interview for Children Symptoms (PICS-IV) (Ickowicz et al. 2006; Zuddas et al. 2006) was administered by experienced clinicians to confirm the diagnosis and to screen for symptoms of other disorders. Estimates of intellectual functioning were obtained using the Wechsler Intelligence Scales for Children (WISC-R) (Wechsler 1974). The child assessment also included self-report measures of anxiety (Multidimensional Anxiety Scale for Children [MASC]) (March et al. 1997) and depression (Children Depression Inventory [CDI]) (Kovacs 1992). Learning disorders were evaluated by reading/writing decoding, comprehension (MT) (Cornoldi and Colpo 1998), and arithmetic tests. A short informal parent educational training (5–10 hours during a few meetings) and an accurate medical evaluation were carried out for all the children before starting pharmacological treatment.
During treatment, prescriptions were renewed every month by a psychiatrist. At this time, global functioning was assessed with the Children's Global Assessment Scale (CGAS) (Shaffer et al. 1983) and degree of symptom improvement was assessed with the Clinical Global Impressions–Improvement score (CGI-I) (Guy 1976); severity of persisting symptoms was also assessed every 3–6 months by CT/PRS-R (Conners 1997). Telephone contacts with teachers and communication between hospital and community social workers were also performed when significant academic or social problems were reported by parents.
MPH treatment
Following the indication of the Italian law for the import of unregistered drugs, written informed consent for both medication administration and analysis of clinical data was obtained from parents and written or verbal assent was given by all participants. A single drug dose (MPH [Ritalin®]) was administered orally at the Hospital Clinic to all subjects (0.3–0.5 mg/kg using 10-mg tablets or fractional doses) to check acute side effects. After the single-dose test, the majority of children/adolescents started chronic treatment. For long-term treatment, MPH titration ranged from 0.3 to 0.5 mg/kg until an allowed maximum of 1 mg/kg per dose in a two to three daily doses. Drug titration was based on improvement in child behavior, school ability, and social skills with peers improvement. Conners' Rating scales were used weekly during titration to obtain information from teachers and parents. The hospital pharmacy was the only possible source of medication for these patients, allowing a strict drug management. Patients starting chronic MPH administration, but withdrawing after some time for different reasons, were followed with different time schedules (but at least annually). Patients who did not start chronic medication after the initial single drug dose were referred to the community child psychiatry system of care.
Treatment schedule included, in the majority of patients, at least 1 month of “drug holiday” during summer vacation. In Sardinia, during the summer, social rules for children's performance are significantly less demanding (e.g., long beach days), and the majority of parents ask for a decrease in drug exposure. The drug holiday was planned to decrease the effects of medication on height and weight as well as to assess the need for continuing medication during the first month(s) of school. Following parent request, a weekend drug holiday (on Sunday) was allowed for about 75% of children.
Assessment of compliance and side effects
Good compliance was defined as the child taking at least 80% of the prescribed pills on a monthly basis for at least 8 months per year: It was checked by the physician asking for, and, when possible, counting the unused pills at the end of each month. Side effects were recorded through a clinician-designed questionnaire asking for the adverse events reported in the Switzerland SPC.
Outcomes definition
At the end of the study (36 months of monthly follow-up), three outcomes were analyzed: (1) To still be on treatment with MPH at the end of study (i.e., patients with no discontinuation during the study); (2) to discontinue MPH during the study due to functional remission; (3) to discontinue MPH during the study for other reasons, such as reduction of efficacy after a period of good response, poor compliance, or other reasons.
Functional remission was defined as a decrease of the number of symptoms to less than five per clinical dimension (Inattention and Hyperactivity/Impulsivity, considering both parent and teacher information) and a score on the Global Assessment of Functioning Scale higher than 60 lasting for a month during school time without medication.
Demographic and clinical characteristics coded from case records
To identify predictive factors for each group, the following variables were considered: (1) Diagnosis, ADHD subtypes (inattentive, hyperactive or combined), and co-morbidity as presence or absence (dichotomous) and type of co-morbidity (DSM-IV diagnosis). (2) Severity of ADHD symptoms, as measured by CT/PRS-R. The following scores were calculated: ADHD index, DSM-IV total subscale, and Global Index total scores from both informants. Only the Parent ADHD index was used in Cox survival analysis (see below). (3) Clinical impairment, as measured by CGAS. (4) Age at the time of the MPH dose test. (5) Gender. (6) Cognitive level, considering IQ as a continuous variable. (7) Family, living with either natural parents or other figures (adoptive parents or guardians, grandparents, uncles) and being only child or having siblings. (8) Residency, living in urban/suburban or rural environment (as defined by Italian National Census; ISTAT 2001). (9) School, having a support teacher/home tutor or not. (10) Side effects, as presence or absence (dichotomous).
Statistical analysis
Three outcomes were considered in the analysis: “Still on treatment at the end of the study” (i.e., absence of remission of any type), “Discontinuation due to remission,” and “Discontinuation for reason other than remission.” Time to event was calculated as the time between first dose of MPH and discontinuation if this occurred (assessed during follow-up visit), for a period of up to 36 months (the end of the study). Predictive factors considered were the previously mentioned demographic and clinical characteristics listed above. Age, cognitive level, and severity of ADHD symptoms (Conners Parent ADHD Index) were considered as continuous covariates, whereas diagnosis was a categorical covariate and all other variables were codified as dichotomous.
According to variable and distribution characteristics, chi-squared, Kruskal–Wallis, Mann–Whitney, or t-tests were used to identify putative predictive parameters for the three outcomes. Considering the longitudinal nature of the study, relevant independent variables were entered into a backward, stepwise Cox proportional hazards model to identify significant predictive factors for each outcome. Goodness of fit of the models was evaluated using a likelihood ratio. Patients were considered: (1) Uncensored when the event happened during the study (i.e., before last follow-up at 36 months); (2) censored when the event happened after the end of study or did not happen.
Continuous variables identified as significant predictors of outcome, were represented graphically using Kaplan–Meier curves (see Fig. 2, below). All statistical procedures were performed using SPSS version 12.0 software package (SPSS Inc., Chicago, IL), with a critical alpha of 0.05 (two-tailed tests).
Results
Patients
Clinical records of the 134 children and adolescents taking medication for at least a month, providing information up to 36 months, were analyzed. Thirty-six months after starting MPH, 62 children (46%) were still on treatment, 32 (24%) had stopped MPH for functional remission, and 40 (30%) had suspended MPH for other reasons. Within the last group, 20 suspended for poor compliance, 10 for decrease of efficacy, 5 for side effects (1 headache, 2 overfocusing, 1 tics and decreased appetite, and 1 dysphoria/irritability), and 5 because they entered in an atomoxetine clinical trial (Fig. 1).
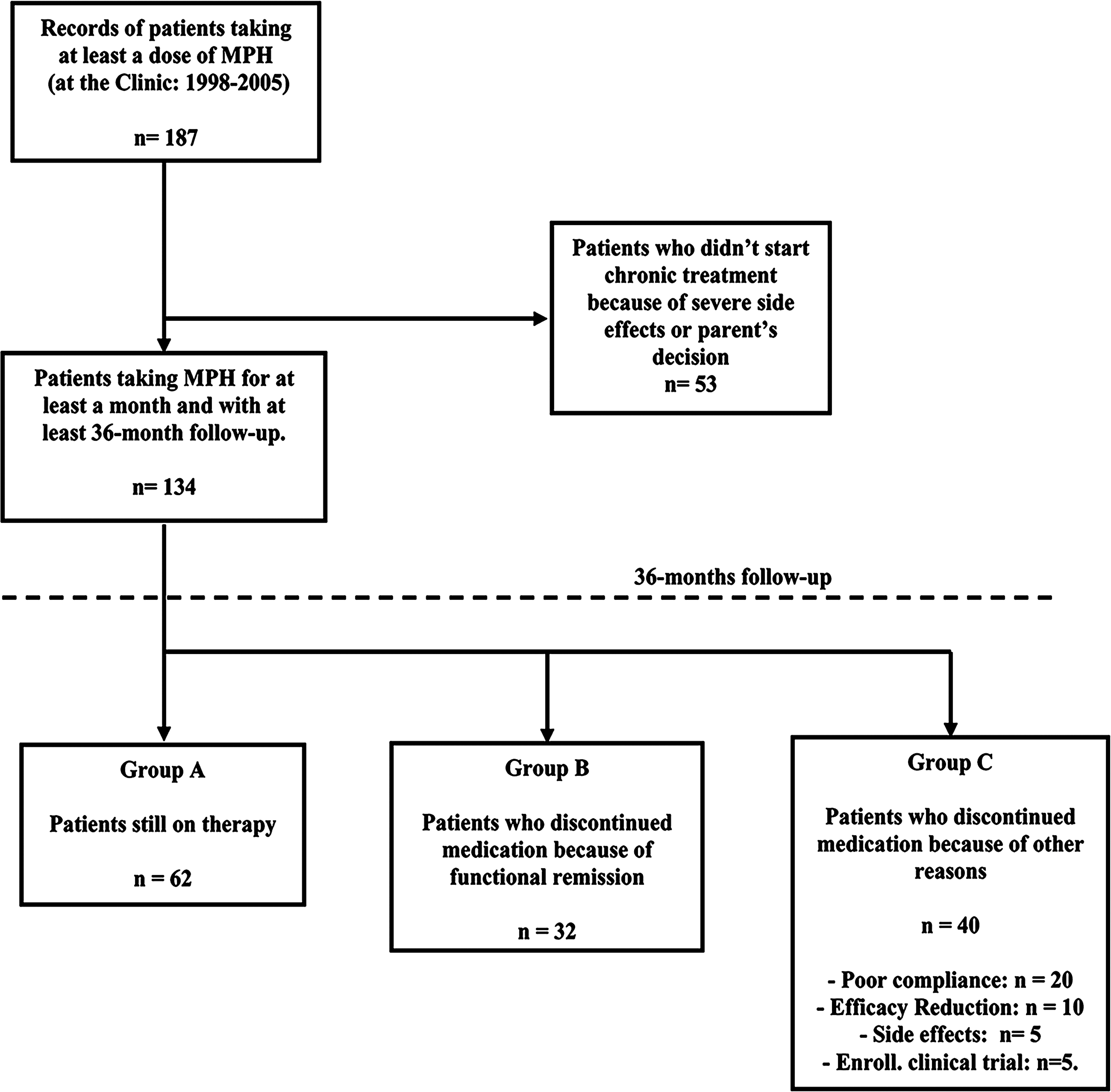
Diagram of subject flow by outcome group. MPH = Methylphenidate.
Demographics and clinical characteristics of the 134 subjects are shown in Table 1. Age ranged from 4 to 16 years (mean age 9 ± 2). Mean age at the beginning of treatment was significantly lower for children still on therapy at 36 months compared to children that discontinued therapy (p = 0.001). The majority of patients suffered from combined subtype (84%), a few children from hyperactive subtype (4.5%), and 12% from inattentive subtype. Duration of therapy for patients who discontinued due to functional remission was similar to those who discontinued for other reasons (mean 15.5 vs. 14.7 months, not significant [N.S.]).
Kruskal–Wallis test.
Chi-squared test.
Abbreviations: SD, Standard deviation; IQ, intelligence quotient; ADHD-C, attention-deficit/hyperactivity disorder combined type; ADHD-H, attention-deficit/hyperactivity disorder hyperactive type; ADHD-I, attention-deficit/hyperactivity disorder inattentive type; ODD/CD, oppositional defiant disorder/conduct disorder; PDD, pervasive developmental disorder.
Baseline severity of ADHD symptoms was measured by the CT/PRS-R. There were no significant differences between groups on any of the Conners' Subscales considered. The mean T-score for the main Conners' Subscale for both parents and teachers ranged from 68 to 75 in the three groups and CGAS was lower than 50 in all patients (mean 46 ± 5). The assignment of a support teacher and the presence of at least one associated disorder, in particular ODD, were more frequent among patients still on therapy (p = 0.008, p = 0.026, and p = 0.030, respectively).
The average dose of MPH ranged from 0.3 to 0.5 (mean 0.42 ± 0.06) mg/kg per dose, with a daily dose ranging from 0.5 to 1.4 (mean 0.96 ± 0.26) mg/kg. There were no significant differences in average doses among the three outcome groups. The majority of patients took the prescribed medications regularly; only 20 subjects reported lower adherence to the treatment (i.e., took less than 80% of the prescribed medication for at least 8 months per year) and eventually stopped medication before the end of the study. During chronic administration of MPH, 54 patients (40.3%) had side effects. The most frequent side effects were decreased appetite (n = 27), irritability (n = 9), and headache (n = 6). Vegetative symptoms (n = 4), stomach pain (n = 3), insomnia (n = 3), dysphoria ( n = 2), tics (n = 2), and logorrhea (n = 1) occurred less frequently. Side effects led to the discontinuation the treatment in only 5 patients.
After the single test dose, 53 patients did not start chronic treatment; they were mostly males (85%), and 89% of them had co-morbid psychiatric disorders. Mean age was 8 ± 3 years. After the first dose test, side effects occurred in 44% children of this group and in 17% of the group that actually started therapy (p < 0.001); children who did not start chronic treatment had significantly lower IQs (mean IQ = 77 vs. 84, p = 0.036).
Predictive factors for specific outcomes
To verify the predictive value of independent relevant variables, a stepwise Cox proportional-hazard model for survival analysis was used.
Patients on therapy at the end of study
Factors that predicted continuation of therapy were: Co-morbidity (p = 0.026, hazard ratio [HR] = 1.876; i.e., presence of associated disorders positively associated with outcome), age (p < 0.001, HR = 0.826; i.e., younger age when starting therapy), gender (p = 0.034, HR = 0.440; i.e., female gender), and family status (p = 0.024, HR = 0.475; i.e., not living with both parents).
Patients that discontinued due to functional remission
Predictors for remission during the study (before 36 months) were: Co-morbidity (p = 0.027; HR = 0.411); i.e., absence of associated disorder positively associated with outcome) and age (p = 0.001; HR = 1.258; i.e., older age at starting therapy).
Patients discontinuing MPH for other reasons
Of the 134 total, 40 children discontinued MPH before the end of the study for reasons other than remission, such as reduction of efficacy, side effects, changing to atomoxetine, and poor compliance. Children who discontinued for these reasons were older when starting therapy (p = 0.024; HR = 1.158) and were more likely to be of the hyperactive subtype (4 out of 6 ADHD-H were in this group) (p = 0.017; HR = 3.548).
This outcome variable was subdivided into the following components: Withdrawal for “poor compliance” (n = 20/134) or for “reduction of efficacy” (n = 10/134). Further analysis was conducted on these specific components. Only age was a significant predictor for the withdrawing due to “poor compliance” component (p = 0.007, HR = 1.270; i.e., older age). Low IQ (p = 0.019; HR = 0.949) and urban residency were predictive for reduction of efficacy component (p = 0.016; HR = 7.040). For the remaining subjects (stopping medication because of side effects or changing medication because entering into an experimental clinical trial with atomoxetine), the number of subjects in these two groups was too low (5 patients each) for further analysis.
Predictive Variables identified by Cox proportional hazards model were used to generate survival curves describing the effect of family structure (Fig. 2A), age (Fig. 2B), and co-morbidity (Fig. 2C) on medication status. A Cox regression model was used for Fig. 2A and Fig. 2C and Kaplan–Meier was used for age, using a cutoff of 12 years (p < 0.001). Mean time on therapy was 17 ± 11 months (median, 14) for patients older than 12 years, compared to 26 ± 12 months (median, 36) for those younger than 12; for co-morbid patients, mean time on therapy was 26 ± 12 months (median, 36), compared to 20 ± 11 months (median, 21) for subjects without co-morbidities; for patients living with both parents, mean time on therapy was 23 ± 12 months (median, 26), compared to 29 ± 11 months (median, 36) for those living in single-parent families.
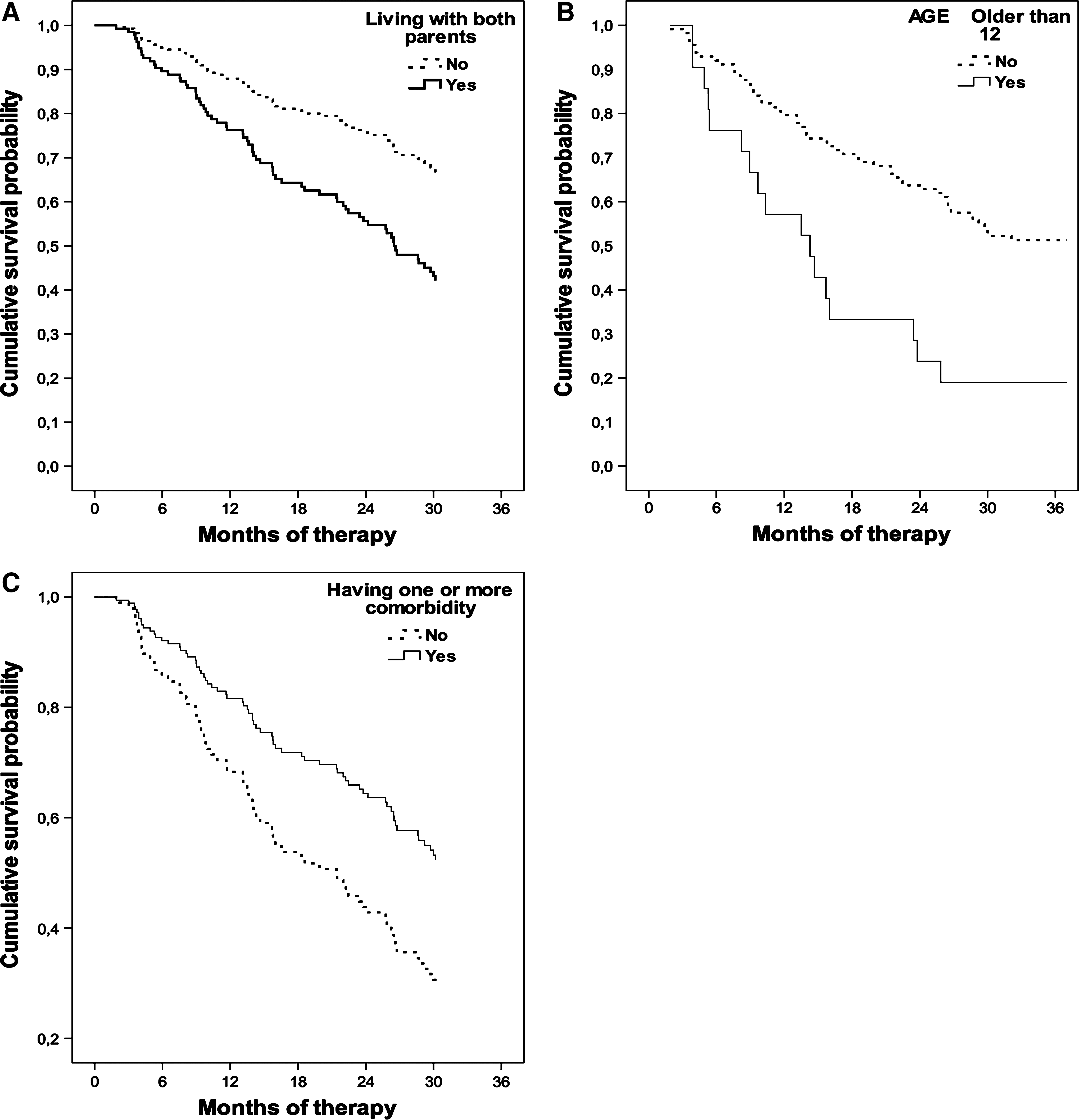
Effect of family structure (
Discussion
The results of the present study show that in an intensive monitoring system of care, after 36 months from first stimulant prescription, almost half (46%) of ADHD children and adolescents continue using medication with persistent significant response, whereas less than one quarter discontinued medication (on average after 15 months) due to functional remission. The remaining 30% of patients withdrew medication for other reasons, including poor compliance (about 15%).
Outcome subtypes
In the present sample, 24% of children/adolescents discontinued MPH due to symptomatic remission: Remission was strongly predicted by older age at medication onset and absence of associated disorders. Symptom remission has been reported in subgroups of ADHD children and adolescents treated for at least 1 year with atomoxetine (Buitelaar et al. 2007). In the MTA study, about 30% of children under intense medication management (predominantly MPH; Med and Comb subgroups) discontinued medication for this reason and maintained the significant clinical improvement observed after 14 months (Jensen et al. 2007).
Only 20 patients out of 134 (15%) stopped medication due to poor adherence. This rate of low adherence was similar to rates reported in studies with an intense psychoeducational component. In general, noncompliance rates with stimulant medication are estimated to be between 20 and 65% (Swanson 2003). In families with high levels of knowledge about ADHD and frequent clinical evaluation (at least every 4 months during the first year of treatment), adherence varied between 74 and 80% (Schachar et al. 1997; Corkum et al. 1999), but decreased to 52–56% after 3 years and to 46% after 5 years of less intensive care (i.e., annual evaluation). In patients with intensive medication management of the MTA study (Med and Comb), the adherence rate was 90% during the first 14 months (monthly visits with at least 20 min of psychoeducation), decreasing to 70% during the following years (annual evaluation) (Jensen et al. 2007).
After 36 months, the majority of patients were still taking medication with good compliance (i.e., attending monthly visits for refilling the prescription). Both the legal limitations and the high parent motivation required to undertake the complex procedures needed to receive MPH (possible selection bias) as well as the intensive system of care provided by the clinic may explain this high rate of persistence. Patients were diagnosed accurately and medication was carefully titrated and monitored over time, with significant educational support by clinicians. During each visit, efficacy, tolerability, and safety of the drug were evaluated and discussed with the family; children/adolescents were supported and motivated to continue therapy. Several other factors, however, appear to predict treatment persistence 36 months after starting medication. The Cox proportional hazards model analysis showed that young age, single-parent or foster family setting, co-morbidity, and female gender were predictors of persistence with therapy. Previous studies indicate younger age (Schirm et al. 2001; Miller et al. 2004; Marcus et al. 2005), white race (Marcus et al. 2005), ADHD combined subtype (Barbaresi et al. 2006), male gender, and initial prescription from a psychiatrist (Miller et al. 2004) as factors associated with greater persistence. The exclusion of 28% (53 out of 187) of the original sample (i.e., no medication after the first test dose) may have contributed to the high compliance observed in the studied sample.
Outcome predictors
In our sample, older age was a predictor for stopping medication because of both poor compliance and symptoms remission. It is common clinical experience that ADHD symptoms decrease in adolescence (Weiss et al. 1971; Faraone et al. 2006), and so does compliance in partial-responder adolescents (Firestone 1982; Brown et al. 1985; Johnson 1993; Thiruchelvam et al. 2001; Swanson 2003; Charach et al. 2004; Miller et al. 2004; Faraone et al. 2007). Usually, parents make treatment decisions for younger children; older children are more likely to refuse medication (Sleator et al. 1982). In fact, parent influence may decrease with time, and, as children reach preadolescence, they will discontinue the stimulant medication. The following have been cited as reasons for discontinuation: Forgetfulness, stigma, adverse effects feelings such as “I'm not my real self,” feared brain damage, losing funny side, “I don't need it,” or incompatibility with misused substances are common reasons for nonadherence (Charach et al. 2008).
Co-morbid disorders, ODD in particular, have also been reported as mediators of poor compliance (Thiruchelvam et al. 2001; Charach et al. 2004). In the present study, both family structure and co-morbidity were predictors of continuing medication, ODD being the more frequent co-morbidity (71%). This apparent contradiction could be explained, considering the particular characteristics of children with ODD and of their response to therapeutic interventions. It is well known that having associated disorders such as ODD and CD make prognosis worse (Barkley et al. 2004; Barkley et al. 2006). In fact, in the presence of an intensive system of care, as in the present study, patients could need longer therapy than those without co-morbidity. The lack of proper family support (i.e., living with only one parent, with only grandparents or in foster care) could lead to a scarce availability of educational strategies, making medication the main treatment (see also Brownell et al. 2006 and Bokhari et al. 2005, for controversial effects of socioeconomic status). It has also been suggested that the environment can play a crucial role in the effects of ADHD medication on ODD symptoms. Kolko and colleagues (Kolko et al. 1999) showed that MPH appears to improve symptoms of hyperactivity and impulsivity in a traditional classroom setting without significant effects on symptoms of oppositionality, whereas in a structured program of therapeutic, educational, and recreational activities, subjects appeared to improve with MPH treatment in both their hyperactive/impulsive and oppositional symptoms.
According to other studies (Firestone 1982; Brown et al. 1985), low patient IQ has been reported as a moderator or mediator of poor compliance; in the present study, although low IQ was a predictor of decreased efficacy over time, it did not appear related to poor compliance. The decrease of stimulant efficacy with time also appeared related to urban residence. The small number of patients showing reduced efficacy does not allow a clear interpretation of these findings.
Finally, it has been suggested that adherence to stimulant treatment may be correlated with both higher baseline ADHD symptom severity and greater treatment response (Charach et al. 2004; Charach and Gajaria 2008). Because availability of medication was limited, in the present sample MPH was prescribed only to very severe cases (no differences in ADHD symptom severity at baseline among groups were observed). In this clinical condition, putative determinants of clinical severity such as co-morbidity and sociodemographic variables, rather than severity by itself, appear to be predictors of both outcome and adherence.
Safety considerations
The results of the present study suggest that MPH is well tolerated in the long term. Fifty-four patients (40%) reported at least one side effect; they were usually very mild and transient. Only 5 patients (4%) stopped because of significant adverse effects after 4–29 months of medication. It has to be taken into account that of 187 children who received the first dose of MPH at the clinic, only 134 (71.6%) subjects started long-term medication; in 14 of them, dysphoria/irritability, logorrhea, persistent involuntary movement, or overfocusing were the reasons for not starting. Studies on long-term safety are still few (Gillberg et al. 1997; MTA Cooperative Group 1999). The incidence of side effects during short-term treatment with stimulants has been reported to be as low as 4–10% and usually mild and transient (Barkley et al. 1990). Schachar and colleagues (Schachar et al. 1997), however, showed that 15% of children treated with MPH terminated treatment because of side effects; for half of them, the side effects appeared after 2–3 months of medication. In a 5-year follow-up of stimulant use, Charach and colleagues (Charach et al. 2004) reported that stimulants continued to cause adverse effects for up to 5 years; 68% of patients reported at least one side effect, usually loss of appetite.
Limitations
Specific limitations are important when considering the present results. First, the study was based in a relatively homogeneous cultural, ethnic, and geographical context, with an unusual legal setting (i.e., lack of market availability of stimulants). For these reasons, the results may not generalize to more diverse settings or other populations. The fact that our clinic was the only source of stimulant medication in the region and one of the very few in the country made it possible to verify compliance and persistence accurately. Second, the retrospective design of the study, the small sample size, and the heterogeneity of specific groups also limit the generalizability of the study. Future studies with larger samples and a prospective design are needed to confirm and generalize these results.
Conclusions
Despite the above limitations, the results of the present study confirm that when a rigorous medication management strategy and an intensive system of care are used, the clinical outcome of ADHD is heterogeneous and adherence to medication may be modulated by different factors. Older age and absence of co-morbidity predict remission of ADHD symptoms after at least 1 year of medication. Younger age, poor family structure, and the presence of co-morbidity predict the need for continuing medication for at least 3 years. Accurate treatment planning (i.e., first dose test), taking into account family preference (i.e., drug holiday), also contributes to the high treatment adherence observed in the studied sample (Charach and Gajaria 2008).
Taken together, our data suggest that it is possible to identify a group of patients that will need long-term therapy that combines medications with intensive psychoeducational intervention. Although further studies in different health systems are warranted, our results strongly suggest that, in the long term, an accurate tailoring of clinical intervention (both pharmacological and educational) for the individual child or adolescent appears crucial for good outcome.
Disclosures
Dr. Zuddas has received research grants from Eli Lilly and Shire Laboratories; has been a speaker for Eli Lilly and Sanofi-Synthelabo; and has an advisory or consulting relationship with Eli Lilly, Shire Laboratories, UCB, and Astra Zeneca. Dr. Atzori holds a fellowship granted by Sardinian Regional Government (Master and Back 2007). Drs. Usala, Carucci, and Danjou have no financial ties or conflicts of interest to disclose.
Footnotes
Acknowledgments
The authors wish to thank the patients attending the Centre for Pharmacological Therapies in Children and Adolescent NeuroPsychiatry who made this study possible, and Dr. Madeleine Groom for reading the manuscript and providing helpful suggestions.
This work was supported in part by the the Sardinian Public Health Secretariat, (D.A.910/2007) and by the Agenzia Italiana del Farmaco (AIFA; Ricerca Indipendente 2006).