
Abstract
Background:
Previous Dutch studies showed increasing psychostimulant use, especially methylphenidate immediate-release (MPH-IR), between 1995 and 2003. In 2003 the extended-release (ER) formulation of MPH and in 2005 atomoxetine (ATX) were introduced in The Netherlands, which increased treatment options.
Objective:
The aim of this study was to describe the change in incidence of attention-deficit/hyperactivity disorder (ADHD) drugs and the prescription profiles of patients younger than 45 years starting treatment with these medicines between 2001 and 2006.
Methods:
Data were obtained from Dutch community pharmacies as collected by the Foundation for Pharmaceutical Statistics, covering 97% of all dispenses for prescription medicines to outpatients in The Netherlands.
Results:
The overall incidence of ADHD drugs use increased 6.5-fold from 2001 to 2006 in men as well as in women. The absolute incidence was highest among 6- to 11-year-old boys. The percentage of first-time MPH-IR users decreased from 98.3% in 2001 to 75.9% in 2006. Likewise, MPH-ER use increased from 0% in 2001 to 18.9% in 2006, and ATX use increased from 0% in 2001 to 3.9% in 2006. The new nonstimulant drug ATX was prescribed more often to adults if they had been previously treated with selective serotonin reuptake inhibitors (SSRIs), benzodiazepines, or antipsychotics. Youngsters <17 years initiated on ATX were often previously treated with antipsychotics or clonidine/guanfacine.
Conclusion:
These findings demonstrate an increase in incidence in use of ADHD drugs between 2001 and 2006 in The Netherlands. The major proportion of all treated patients comprised boys, 6–11 years old; most of them were treated with MPH-IR. In a few years time, the use of extended-release drugs as part of all ADHD drug prescriptions increased considerably, despite the lack of full reimbursement of these extended-release drugs. Psychostimulants and atomoxetine in children, adolescents, and adults are probably used to address different treatment needs.
Introduction
In the last decade, many different aspects of ADHD have been studied worldwide, and concerns have been raised about the increase in diagnosing ADHD, the rise in stimulant use for the treatment of ADHD, and the lack of follow-up research on long-term effects of these drugs. In many countries, the use of stimulants for the treatment of ADHD has increased substantially over the previous two decades (Robison et al. 1999; Zito et al. 2000; Miller et al. 2001; Schirm et al. 2001; Reid et al. 2002; Vinker et al. 2006; Zito et al. 2007; Winterstein et al. 2008). An increase is not only found among school-aged children (Robison et al. 1999), but also among preschoolers (Zito et al. 2000; Zito et al. 2007) and adults (Robison et al. 2005; Castle et al. 2007). In The Netherlands, this increase was reported by several pharmacoepidemiological studies among children younger than 18 years, conducted between 1995 and 2003 (Schirm et al. 2001; Hugtenburg et al. 2004; Faber et al. 2005). Schirm et al. (2001) found an increase of the prevalence of immediate-release stimulants of 1.5/1000 in 1995 to 7.4/1000 in 1999. Between 1995 and 2001, the use of all psychotropic medication among boys and girls younger than 18 years doubled, largely due to use of immediate-release stimulants by 5- to 14-year-old boys (Hugtenburg et al. 2004). Also, Faber et al. (2005) found a two-fold increase in prevalence of immediate-release stimulants use from 6/1,000 in 1998 to 12/1,000 in 2002. Until 2003, short-acting stimulants like methylphenidate immediate-release (MPH-IR, Ritalin) and dexamphetamine (Dexedrine) were available for the treatment of ADHD. In 2003, MPH extended release (MPH-ER, Concerta) and in 2005 atomoxetine (ATX, Strattera), a nonstimulant, as long-acting medication for the treatment of ADHD were introduced to the Dutch market. Both new medicines are, like MPH-IR, approved for use in children 6–18 years old with ADHD. ATX is also approved for adults, although only for those patients who have been previously treated with ATX during childhood or adolescence. In the United States, there was a dramatic increase in use of extended-release drugs after their introduction, especially in the pediatric (0–19 years), but also in the adult (>20 years), population between 2000 and 2005 (Castle et al. 2007).
To our knowledge, no studies in The Netherlands have assessed the effect of the introduction of these new treatment options on the use of ADHD medication. Little is known about the extent and patterns of use of ADHD medication in adulthood. Therefore, the objective of this study was to assess trends in the incidence of ADHD drug use in The Netherlands in the period 2001–2006 and in the prescription profiles of ADHD drug users.
Methods
Setting
Data were obtained from the Foundation for Pharmaceutical Statistics (Stichting Farmaceutische Kengetallen, SFK). As of 1990, SFK has been collecting dispensing data from a growing number of community pharmacies in The Netherlands. In 2001, the catchment area of SFK consisted of 1,629 community pharmacies in both rural and urban areas all over The Netherlands, representing 90.7% of the total number of Dutch pharmacies. In 2006, coverage had increased to 92% the total number of Dutch pharmacies and 97% of the Dutch population (
Study medication and population
We identified all patients born after 1960 (i.e.,<45 years of age) that have been dispensed at least one prescription between January 2001 and December 2006, for drugs approved for use in the treatment of patients with ADHD (MPH-IR and MPH-ER, ATX, dexamphetamine). From here on, we will refer to these drugs as “ADHD drugs.” Information about the prescribed medication contained patient identification (anonymous), dispensing date, number of units dispensed, and prescribed daily dose. For the present study, only incident users of an ADHD drug were included, where incident use was defined as having no ADHD drug dispensed in the prior 6 months. All patients were required to have at least 6 months of history in the SFK database prior to this prescription date.
Data analysis
For each year between 2001 and 2006, we calculated the incidence of ADHD drug use per 10,000 inhabitants by dividing the number of incident users per calendar year by the midyear population size of the corresponding year. The number of incident users per calendar year was corrected for the actual number of pharmacies in The Netherlands using a multiplication factor. Furthermore, the midyear population size of the corresponding year was corrected for the coverage provided by community pharmacies in The Netherlands. Data about number of inhabitants was provided by Statistics Netherlands (
For each patient, we assessed the use of other psychotropics during the 6 months prior to ADHD treatment initiation. Drugs of interest were antipsychotics (typical and atypical), antidepressants (tricyclic, selective serotonin reuptake inhibitors [SSRI]), clonidine/guanfacine, drugs used in addictive disorders, lithium, benzodiazepines, and antiepileptic drugs (AEDs).
Differences with respect to psychotropics used prior to ADHD drugs between 2001 and 2006 were tested by means of a chi-squared test. We tested for differences by means of a chi-squared test between age groups, type of ADHD drug, and use of psychotropics, used prior to the start of that specific ADHD drug in 2005 and 2006. By that time, the newer extended-release ADHD drugs had been introduced. Differences were considered significant at p < 0.05 (two-tailed).
Results
We identified 738,978 prescriptions for psychostimulants for 62,098 unique patients, of whom 34,335 (55%) were incident users. The overall incidence of ADHD drug use among males and females aged <45 years increased 6.5-fold from 47.5/100,000 (95% confidence interval [CI], 45.5–49.5/100,000) in 2001 to 309.6/100,000 (95% CI, 306.1–313.2/100,000) in 2006. This increase was the same in men and women, although the absolute incidence was 2.7-fold higher among men (68.6/100,000; 95% CI, 65.3–72.0/100,000) in 2001 to 447.4/100,000 (95% CI, 441.7–453.7/100,000) in 2006) than among women (25.6/100,000; 95% CI, 23.6–27.8/100,000) in 2001 to 167.7/100,000 (95% CI, 164.0–171.5/100,000) in 2006). A five-fold increase in incidence is found among MPH-IR users for all ages (46.7/100,000; 95% CI, 44.7–48.7/100,000) in 2001 to 234.6/100,000 (95% CI, 231.5–237.7/100,000) in 2006). The absolute incidence in 2006 was highest among boys aged 6–11 years (1,457.1/100,000; 95% CI 1, 426.7–1,489.2/100,000). The (overall) increase in incidence was lowest among children <6 years (2.9 times; 2001 20.9/100,000, 95% CI, 17.3–25.1/100,000 and 2006 59.7/100,000, 95% CI, 55.1–64.4/100,000).
After introduction of extended-release ADHD drugs, the percentage of MPH-IR incident use compared to extended-release drug use declined between 2001 and 2006. Especially male and female adolescents were likely to be initiated on MPH-ER (Figs. 1, 2, and 3). Between 2001 and 2006, the relative percentage of MPH-IR initiations compared to all initiations decreased from 99.6% to 60.1%, although the absolute number of starters of MPH-IR increased during the whole study period. The relative percentage of MPH-ER increased to 33.2% and of ATX to 6.1% (data not shown).
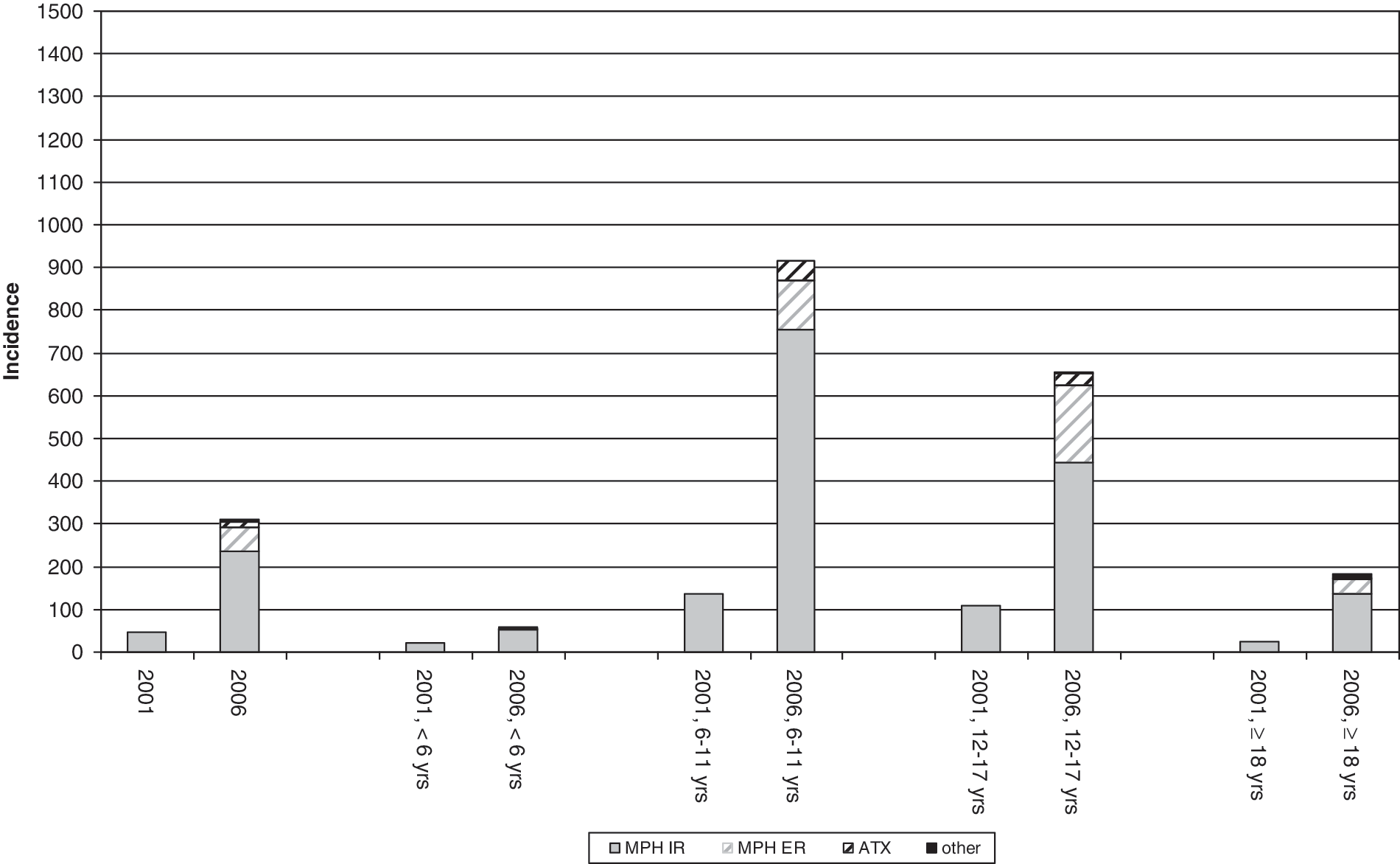
Overall incidence of attention-deficit/hyperactivity disorder (ADHD) drug use per 100,000 inhabitants in The Netherlands in 2001 and in 2006. MPH-IR = Methylphenidate immediate-release; MPH-ER = methylphenidate extended-release; ATX = atomoxetine.

Incidence of attention-deficit/hyperactivity disorder (ADHD) drug use per 100,000 men in The Netherlands in 2001 and in 2006. MPH-IR = Methylphenidate immediate-release; MPH-ER = methylphenidate extended-release; ATX = atomoxetine.

Incidence of attention-deficit/hyperactivity disorder (ADHD) drug use per 100,000 women in The Netherlands in 2001 and in 2006. MPH-IR = Methylphenidate immediate-release; MPH-ER = methylphenidate extended-release; ATX = atomoxetine.
The characteristics of the patients initiated on ADHD drugs are shown in Table 1. Use of any psychotropic medication prior to the start of MPH or ATX was highest among adults (41.5%), and mainly comprised antidepressants (25.4%, of which SSRIs 17.0%), and benzodiazepines (23.9%). Use of antipsychotics (10.4%) and clonidine/guanfacine (5%) was highest among children younger than 6 years. Table 2 shows the psychotropics used during the 6 months prior to the start of MPH-IR and MPH-ER and ATX in 2005 and 2006 after introduction of the extended-release medicines. Adults received the highest percentage of other psychotropics, mainly SSRIs and benzodiazepines, before starting an ADHD drug. Among youngsters, aged 0–17 years, clonidine/guanfacine and typical and atypical antipsychotics were used significantly more often before starting ATX. Patients starting on ATX had a higher prevalence of use of almost all other psychotropics compared to MPH-IR and MPH-ER starters (p < 0.05).
Abbreviations: ADHD = Attention-deficit/hyperactivity disorder; TCA = tricyclic antidepressant; SSRI = selective serotonin reuptake inhibitors; AEDs = antiepileptic drugs.
Abbreviations: ADHD = Attention-deficit/hyperactivity disorder; MPH-ER = methylphenidate extended-release; MPH-IR = methylphenidate immediate-release; ATX = atomoxetine; TCA = tricyclic antidepressant; SSRI = selective serotonin reuptake inhibitors; AEDs = antiepileptic drugs.
Discussion
This study showed a considerable change from 2001 to 2006 in the incidence and the pattern of prescribing ADHD drugs in The Netherlands. A large increase in incidence of psychostimulant prescription as found in other (inter)national studies was confirmed by our study and was associated with gender and age (Robison et al. 1999; Zito et al. 2000; Miller et al. 2001; Schirm et al. 2001; Reid et al. 2002; Hugtenburg et al. 2004; Faber et al. 2005; Robison et al. 2005; Vinker et al. 2006; Castle et al. 2007; Zito et al. 2007; Winterstein et al. 2008). Incidence increased most in boys, but also in females, young children, and adults. A recent Dutch study by van Dijk et al. (2008) confirmed a rise in ADHD drug prescription and diagnosing between 2002 and 2007 in boys and girls. Most patients were male in this study. Safer et al. (1996), Schirm et al. (2001), Vinker et al. (2006), and Castle et al. (2007) also concluded that there is an increase in use and prescription rate of stimulants among girls and women. The rapid growth in treatment with stimulants among girls is probably caused by better recognition of ADHD mainly attention-deficit disorder (ADD) symptoms in girls by parents, teachers, and health-care professionals and higher diagnostic rates (Kooij and de Noord 2007). Rising prescriptions of ADHD drugs to the very young children are of public concern (Zito et al. 2007). In our study, however, the increase in incidence was lowest among children <6 years Prior to the start of psychostimulants in these young children, we found a high percentage of (off-label) prescriptions of typical antipsychotics, supposing a need for a psychopharmacological intervention due to severe behavioral symptoms in these youngsters. Recognition and referral increased in adults by a greater awareness among themselves and health-care professionals, as well as the development of diagnostic tools, medication guidelines, and treatment opportunities (Kooij 2003; Weiss and Murray 2003; Bren 2004). A meta-analysis of Faraone et al. (2006) showed that the persistence of ADHD from adolescence to adulthood (age 25) was almost 15% for the strict Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association 1994) criteria. Although in partial remission, two-thirds of the adult ADHD patients showed clinical impairment.
The prescription of MPH-ER and ATX was mainly due to the large increase in prescriptions of all ADHD drugs in our study. The relative decrease in use of MPH-IR, although the absolute numbers of prescriptions increased, was also found in the United States between 1996 and 2005 (Habel et al. 2005; Castle et al. 2007). The rapid increase of prescriptions of extended-release drugs can be explained by perception of advantages by either patients, parents, or doctors over MPH-IR with respect to less rebound effects, once-a-day administration, less stigmatization at school, or reduced potential for drug misuse (Lage and Hwang 2004; Marcus et al. 2005; Banaschewski et al. 2006) or other side effects and 24-hour coverage of ADHD symptoms by ATX. Substance abuse is a well-known co-morbid disorder in adolescents and adults with ADHD (Kooij and de Noord 2007). Immediate-release stimulants are at a greater risk to be misused, suggesting that MPH-IR should not be prescribed in drug abusers or an at-risk population (Banaschewski et al. 2006). Both male and female adolescents in our study, who go to secondary school at the age of 12 years in The Netherlands, were more likely to use MPH-ER compared to other ages and may benefit from these advantages. Use of MPH-ER is associated with a greater continuity of treatment than immediate-release formulations in youth (Lage and Hwang 2004; Marcus et al. 2005) and adults (Olfson et al. 2007). Scientific evidence, full reimbursement, but also marketing efforts, are as influential in this respect (Layton et al. 2008). In The Netherlands, MPH-ER and ATX in general are not fully reimbursed despite the lobbying efforts of patient pressure groups and health-care professionals to persuade government, health-care insurers, and Members of Parliament. Therefore, prescriptions seem to be restricted to those who actually can afford this particular medication.
ATX was prescribed more often to children and adolescents when they had a patient history of antipsychotic or clonidine/guanfacine use. Antipsychotics in general are not recommended for the treatment of ADHD. Clonidine and guanfacine are third-line agents in the treatment of ADHD (Multidisciplinaire Richtlijn ADHD 2005). This suggests that ATX is used as a last resort. Is has been described in literature that newly introduced drugs are often prescribed to specific group of patients who, for example, did not respond well enough or with unpleasant side effects to the so called “old established drugs.” They are also prescribed to those who may benefit less from drugs in general or to patients as first-line drug because of side effects and risk profile (Egberts et al. 1997; Layton et al. 2008). Use of antipsychotics, SSRIs, and benzodiazepines prior to the initiation on ATX in adults suggests a change in diagnosis of those patients toward ADHD or using it as a last resort or the presence of other more severe co-morbid disorders. This is in line with findings of van Brunt et al. (2006), who found that ATX was prescribed more often as treatment initiation to adults with ADHD with a prior diagnosis of bipolar disorder, alcohol dependence, previous use of antipsychotics, or antidepressants compared to stimulants.
There are several limitations in this study. We did not have any information on the indication of ADHD drug use. Although MPH is the first choice pharmacotherapeutical intervention in the treatment of ADHD for children, adolescents (Multidisciplinaire Richtlijn ADHD 2005), and adults (Kooij 2003; Spencer et al. 2005), it can also be prescribed to adults for somatic problems such as a delirium or during the palliative phase of a somatic disorder (Donker et al. 2005; Gagnon et al. 2005). Results of the study can also be affected by the impossibility to analyze the data of dexamphetamine. Dexamphetamine is only available as compounded capsules prepared in a pharmacy, and its prescription cannot be traced through the SFK. Little is known about the influence of studies or guidelines on ADHD drug treatment published in professional journals, (inter)national conventions, or marketing strategies of pharmaceutical companies on the prescribing behavior of health-care professionals or the perception on ADHD symptoms and medication of patients, parents, or teachers (Layton et al. 2008). These factors may contribute to a more tolerant attitude toward ADHD drugs. Data for this study were obtained from a subset of 745 pharmacies having complete medication data during the study period. It seems unlikely this has resulted in selection bias because reasons for pharmacies not having a complete medication history are likely to be administrative only.
Conclusion
Between 2001 and 2006, a large increase was observed in the prescription rates of ADHD drugs in The Netherlands, not only in children and adolescents but also in adults. Shortly after their introduction and despite the high costs, MPH-ER and ATX conquered an important share of the market. Clinicians, patients, and parents quite often seem to make a choice for extended-release drugs or nonstimulant ADHD drugs. The economic implications of not only the rise of the prescriptions of ADHD drugs but also of untreated ADHD should be subject of future research. More research about factors that influence choices between immediate- or extended-release drugs is necessary. More research on efficacy and safety of ADHD drugs in adults and preschoolers is needed too. We only analyzed data of adults from 18 to 45 years of age. It would be interesting to extend this study to elderly persons, because ADHD symptoms can even occur up to the age of 75 years (Kooij et al. 2005).
Footnotes
Disclosures
E. van den Ban has lectured for and received reimbursement for travel to a convention from Janssen-Cilag BV; has done scientific research for (no personal grant), lectured for, is on the advisory board of, and has been reimbursed for travel to a convention by Lilly Nederland BV; is on the advisory board and has been reimbursed for travel to a convention by UCB Pharma BV; and has lectured for Eurosept BV (no personal grant). P. Souverein, H. Swaab, H. van Engeland, R. Heerdink, and T. Egberts report no relationships with pharmaceutical companies.
The division of Pharmacoepidemiology & Pharmacotherapy, which employs P.S. and T.E., has received unrestricted funding for pharmacoepidemiological research from GlaxoSmithKline, Novo Nordisk, the private–public-funded Top Institute Pharma (