
Abstract
Objective:
The aim of this study was to examine global functioning, health-related quality of life (HRQOL), and clinical outcome in children and adolescents with bipolar I disorder, schizophrenia, or schizoaffective disorder following ziprasidone treatment.
Methods:
Sixty-three subjects (aged 10–17 years) received open-label ziprasidone, titrated from 10 to 40 mg twice a day (b.i.d.) (low-dose group) or from 20 to 80 mg b.i.d. (high-dose group); fixed doses were used until week 3, followed by flexible doses for 6 months. The Children's Global Assessment Scale (CGAS) characterized functional impairment at baseline and following treatment. The Child Health Questionnaire (CHQ) assessed HRQOL at baseline.
Results:
Baseline CHQ showed greater impairment in psychosocial functioning than in physical health. Baseline mean CGAS scores were substantially below normal (i.e., <70), indicating functional impairment. Improvement in CGAS scores occurred as early as the first week of treatment. The low correlations between both CHQ and CGAS and the efficacy measures at baseline indicate that these scales measure different constructs. Nevertheless, there was good correlation between improvements in the CGAS and changes in Brief Psychiatric Rating Scale-Anchored (BPRS-A) and Young Mania Rating Scale (YMRS) during ziprasidone treatment.
Conclusion:
CHQ and CGAS scales may be useful together with standard efficacy measures for children and adolescents with these disorders.
Introduction
Children and adolescents with mood and psychotic disorders (bipolar disorder [BPD], schizophrenia, schizoaffective disorder) often exhibit impaired daily functioning. In fact, the Diagnostic and Statistical Manual of Mental Disorders, 4th edition Text Revision (DSM-IV-TR) criteria for all three disorders requires disruption in functioning, whether in social or occupational spheres (American Psychiatric Association 2000). A measure of pediatric functioning, the Children's Global Assessment Scale (CGAS), was developed to provide a global measure of level of functioning in children and adolescents similar to the Global Assessment of Functioning (GAF) for adults (Shaffer et al. 1983). Studies that have included the CGAS in pediatric patients with BPD have found impairment at baseline in the moderate to severe range (DelBello et al. 2002; Barzman et al. 2004; Pavuluri et al. 2005; Tillman and Geller 2007). In general, these studies report a significant gain in functioning, indicated by an increase of approximately 15 points in CGAS scores following treatment with an atypical antipsychotic.
HRQOL is the term that is generally used to refer to that part of an individual's quality of life that is related to that person's health status (Wilson and Cleary 1995). It may include aspects such as the capacity to attend work (or school in the case of children), to interact socially, and to function physically or emotionally. HRQOL can thus be seen as the subjective or perceived well-being on multiple areas of life including physical, mental, and social domains (Coons et al. 2000). HRQOL falls outside the realm of more conventional efficacy measures, such as the Young Mania Rating Scale (YMRS) (Young et al. 1978) and the Brief Psychiatric Rating Scale (BPRS) (Overall and Gorham 1962), that are often used as the primary efficacy end points to assess change in symptom severity. Although there has been some investigation in youth with attention-deficit/hyperactivity disorder (ADHD) (Perwien et al. 2006), few studies have examined HRQOL in children and adolescents with bipolar mania, schizophrenia, or schizoaffective disorder. One small study examined the effects of treatment with divalproex or quetiapine on the HRQOL in adolescents diagnosed with a bipolar manic or mixed episode (Rademacher et al. 2007) using the Child Health Questionnaire (CHQ) (Landgraf et al. 1999) to assess HRQOL. At baseline, subjects had lower scores on the subscales of the CHQ assessing psychosocial health than those measuring physical health. Gains were observed for many of the psychosocial subscales by day 28 of treatment.
The current study used post hoc analyses of the CGAS and the CHQ to examine impairment in functioning and HRQOL, respectively, in children and adolescents with schizophrenia, schizoaffective disorder, or BPD. The CGAS was also measured following open-label treatment with ziprasidone for up to 6 months. This study included these measures as exploratory measures to: (1) better characterize the HRQOL and functioning of these subjects at the time of study entry; (2) examine the relationship between these measures and ratings of symptom severity; and, in the case of the CGAS, (3) explore the relationships between symptom improvement and functioning following open-label treatment with ziprasidone for up to 6 months.
Methods
Study design
Ten study sites screened 82 subjects (inpatients or outpatients), of which 63 entered the study. The 27-week trial comprised a 3-week randomized, fixed-dose period (period 1), followed by a 24-week, open-label, flexible-dosing period (period 2) to assess the safety and tolerability of ziprasidone in children and adolescents. Scheduled visits occurred at screening, baseline, and during period 1 (day 4 and weeks 1, 2, and 3) and period 2 (weeks 4, 8, 12, 18, and 27). The study design and changes in symptom ratings have been reported previously (DelBello et al. 2008).
Briefly, children and adolescents (aged 10–17 years) with a diagnosis of BPD I, either manic or mixed episode (n = 46), and a YMRS score ≥17 or with a diagnosis of schizophrenia or schizoaffective disorder (n = 17) and a total BPRS-Anchored (BPRS-A) score ≥35 and ≥4 on at least one of the BPRS-A items for unusual thought content, hallucinations, suspiciousness, or conceptual disorganization were eligible for study participation. Main exclusions were substance-induced psychotic disorder, recent prior treatment with clozapine, depot antipsychotic or monoamine oxidase inhibitor, a perceived risk of suicide or homicide, or any serious unstable medical or neurologic illness.
Informed assent and written informed consent were obtained from all study participants and legal guardians, respectively, prior to study participation.
Concomitant medications
Concomitant stimulants, antidepressants, and mood stabilizers were prohibited during period 1 but permitted during period 2. Benzodiazepines were allowed for the relief of anxiety, agitation, or insomnia. The use of benztropine and/or propranolol was permitted. The washout period for prior antipsychotics was at least 24 hours, and approximately four half-lives were required for other prohibited medications.
Psychosocial assessments
The CGAS is an adaptation of the adult version of the Global Assessment Scale and is similar to the GAF (Shaffer et al. 1983). It is a single item scored 1–100 to rate functioning and degree of impairment due to symptoms. As with the GAF, descriptors appropriate for children and adolescents are provided for each 10-point range. Clinicians were instructed to rate the CGAS, taking into account clinical interviews with both parents and children and to record the lowest level of general functioning over the past month. The CGAS was completed at baseline, day 4, and weeks 1, 2, 3, 12, and 27.
The CHQ scale is a measure of both a child's physical, emotional, and psychosocial well-being, as well as the relative burden of disease on the parents and family (Landgraf et al. 1999) and is considered a measure of HRQOL. The CHQ is suitable for use in children aged ≥5 years and measures the child's well-being over the past 1 month. The CHQ was completed by a parent (or legal guardian) at baseline. The 50-item written questionnaire scoring yields 11 subscales, 4 individual items, and 2 global summary scores known as the Physical and Psychosocial Component Scores. The CHQ scoring algorithm calculates a norm-based score for each participant in the clinical trial. This score enables the comparison of the observed scores to a representative sample of community-based children aged 5–18 years drawn from the general U.S. population. The normalized scores for these analyses were based on age. To compute the normed scores, subjects were stratified by age into three groups: 11–12 years, 13–15 years, and 16–18 years. No corrections were made for the child's gender or the parent characteristics due to the small sample size in this trial.
Efficacy assessments
The YMRS (Young et al. 1978) (bipolar subjects only) and the BPRS-A (Overall et al. 1962) (schizophrenia and schizoaffective subjects only) were administered at screening, baseline, all scheduled visits during period 1, and weeks 12 and 27 during period 2. Raters were instructed on the use of these clinician-rated instruments, and the CGAS, prior to study initiation.
Statistical analyses
Cronbach α was calculated for subscales on the CHQ. The percentage of subjects scoring below their same-age peers on components of the CHQ at baseline was summarized by age group. Mean values and changes from baseline for the CGAS were summarized by dose group at day 4, and weeks 1, 2, 12, and 27. Effect sizes (Cohen d) were calculated for the change in the CGAS through period 1. Monte Carlo simulations were used to estimate the 95% confidence intervals (CIs) for the effect sizes for both observed cases (based on week-3 visit window of days 18–24) and for those subjects with at least one postbaseline CGAS assessment falling within a study visit window (last observation carried forward [LOCF]). Some subjects were not included in these LOCF analyses because they fell outside the study visit window. An exploratory mixed-model, random regression analysis examined changes in CGAS scores over time with age, gender, diagnosis, and dose groups entered as possible predictors. Models including interaction terms for each of these baseline predictor variables (singly and jointly) with CGAS trajectories over time were evaluated. Likelihood ratio tests (p < 0.20) were used to select the explanatory variables to be retained in the final model. Correlations (Pearson r) between the CGAS and CHQ scores and change in rating scale scores were calculated.
Results
Subjects
Twenty-three subjects were enrolled in the low-dose group and 40 subjects were enrolled in the high-dose group (Table 1). Forty-six subjects had a diagnosis of BPD I, 7 schizophrenia, and 10 schizoaffective disorder (mean duration of diagnosis 1.2 and 4.1 years for low-dose and high-dose groups, respectively). Sixteen subjects were aged 11–12, 25 were aged 13–15, and 21 subjects were aged 16–18 years.
Abbreviation: SD = Standard deviation.
During period 1, 25 patients (40%) discontinued study participation. Reasons for discontinuation included adverse events (AEs) (19 patients), lack of response (3 patients), and lost to follow-up or withdrawal of consent (2 patients). Many patients who discontinued due to AEs in period 1 were unable to tolerate the maximum dose. Patients who discontinued in period 1 had the option to participate in period 2 where flexible dosing was permitted. Fifty-six patients entered period 2.
Child Health Questionnaire
Each age group scored below norms on the CHQ Psychosocial Component Scale. For the Physical Component Scale, 60% and 62% of subjects in the two older age groups were at or above peer norms. In the youngest age group, 60% scored below the norm for same-age peers. Deficits relative to same-age peers were observed in several psychosocial subscores, including family activities, impact on parent time, impact on parent emotions, mental health, self-esteem, and behavior (Fig. 1). Within the constraints of the small sample sizes, the effects were consistent across age groups. Similar patterns were seen across the diagnostic groups. Subscales assessing constructs related to physical health revealed less impairment than those dealing with psychosocial health. Internal consistency (Cronbach α) results for the subscales on the CHQ for the entire sample were generally in keeping with those reported in the manual (Landgraf et al. 1999), ranging from 0.70 to 0.87.
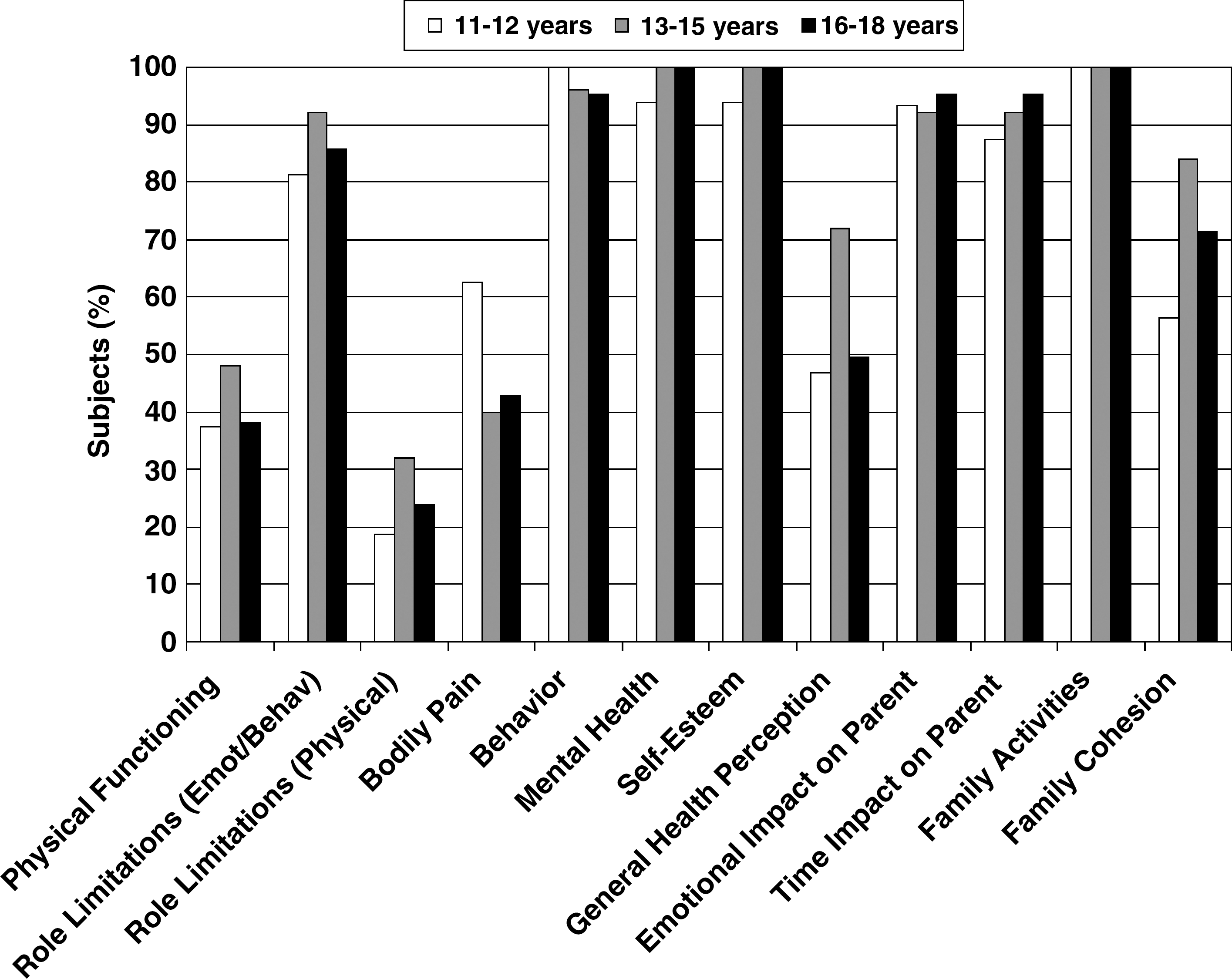
Proportion of subjects in different age groups scoring below their same-age peers on Child Health Questionnaire (CHQ) subscales at baseline.
Children's Global Assessment Scale
The mean baseline mean CGAS scores (±standard deviation [SD]) were 41.7 ± 9.9 for the low-dose group and 39.0 ± 10.0 for the high-dose group. The mean increase in CGAS score from baseline to week 3 was 14.4 ± 13.7 for the low-dose group and 17.4 ± 15.4 for the high-dose group. At baseline, no subject scored ≥70 on the CGAS (≥70 = normal functioning). By the end of week 3, 5 subjects scored ≥70. The effect size for the CGAS change from baseline to the end of period 1, collapsing across all diagnoses and both dose groups, was 1.35 (n = 59; 95% CI = 0.97–1.78, LOCF) and 1.65 (n = 39; 95% CI = 1.22–2.19, observed cases).
Symptoms and functioning
Table 2 presents the correlations for the CGAS and two CHQ component summary scales (Physical and Psychosocial) with the rating scale scores at baseline. Figure 2 shows the relationships among improvements in CGAS, BPRS-A, and YMRS scores over the 27-week course of the trial.
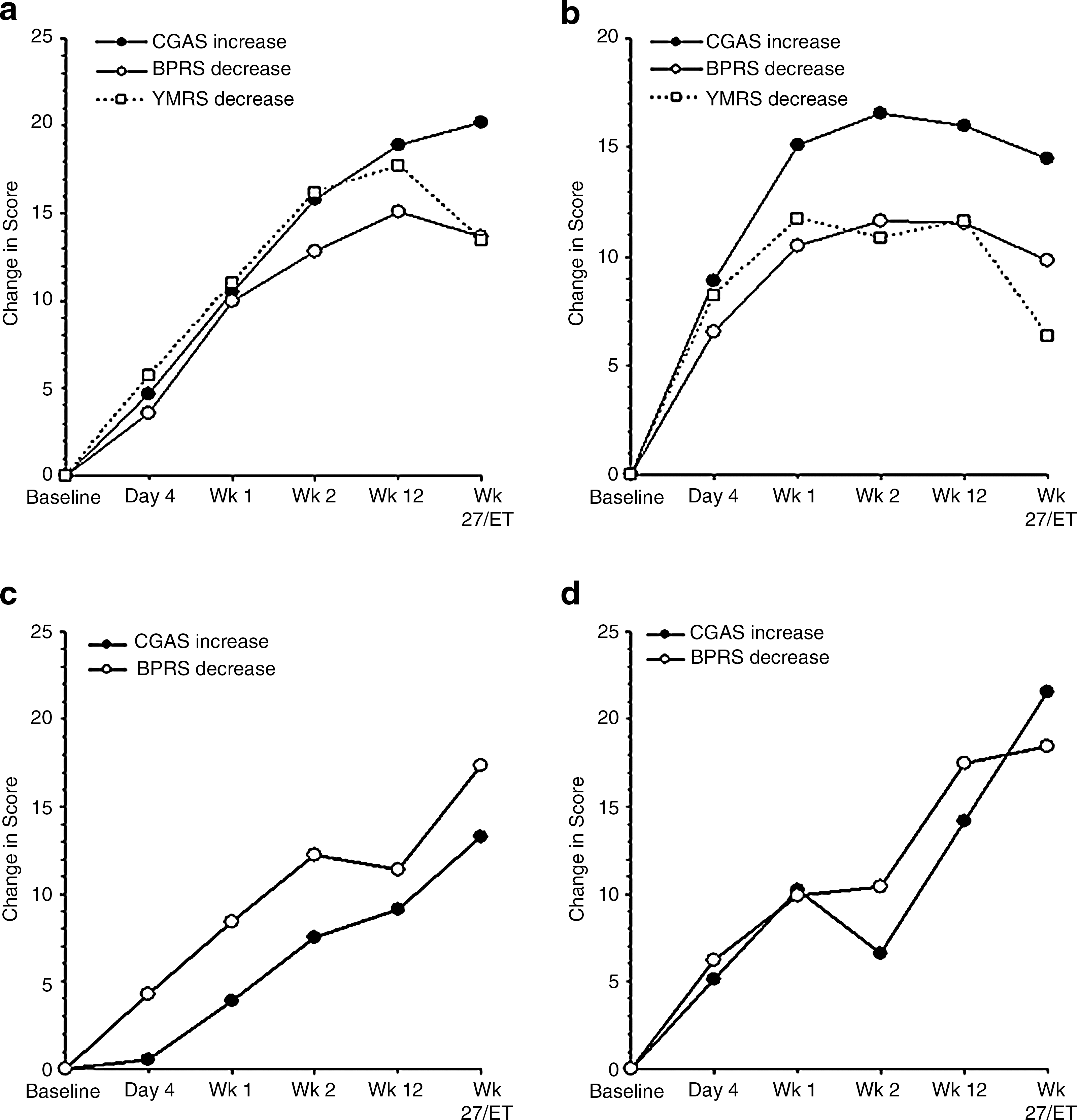
Children's Global Assessment Scale (CGAS), Brief Psychiatric Rating Scale-Anchored (BPRS-A), and Young Mania Rating Scale (YMRS) score changes over time. (
No correlations were significantly different from zero.
Abbreviations: GCAS = Children's Global Assessment Scale; CHQ = Child Health Questionnaire; YMRS = Young Mania Rating Scale; BPRS-A = Brief Psychiatric Rating Scale-Anchored.
There were no statistically significant correlations between baseline CGAS, CHQ Psychosocial or Physical Summary Component scores, and baseline YMRS or BPRS-A values (Table 2). There were also no significant correlations between baseline CGAS, CHQ Psychosocial or Physical Summary Component scores, and subsequent changes in the YMRS or BPRS-A scores. However, there was a correlation between change from baseline on the CGAS and the change in YMRS total score (−0.53, p < 0.01) or BPRS-A total score (−0.56, p < 0.05).
The model selection process for the exploratory mixed-model, random regression analysis resulted in a final model with diagnosis group-by-intercept and gender-by-diagnosis-by-slope terms as significant (p < 0.20) predictors of CGAS change over time. This model showed that intercepts differed by diagnosis, with bipolar subjects scoring higher at baseline. Rates of change were similar for all subjects except bipolar females, who showed greater gains more rapidly (Fig. 3).
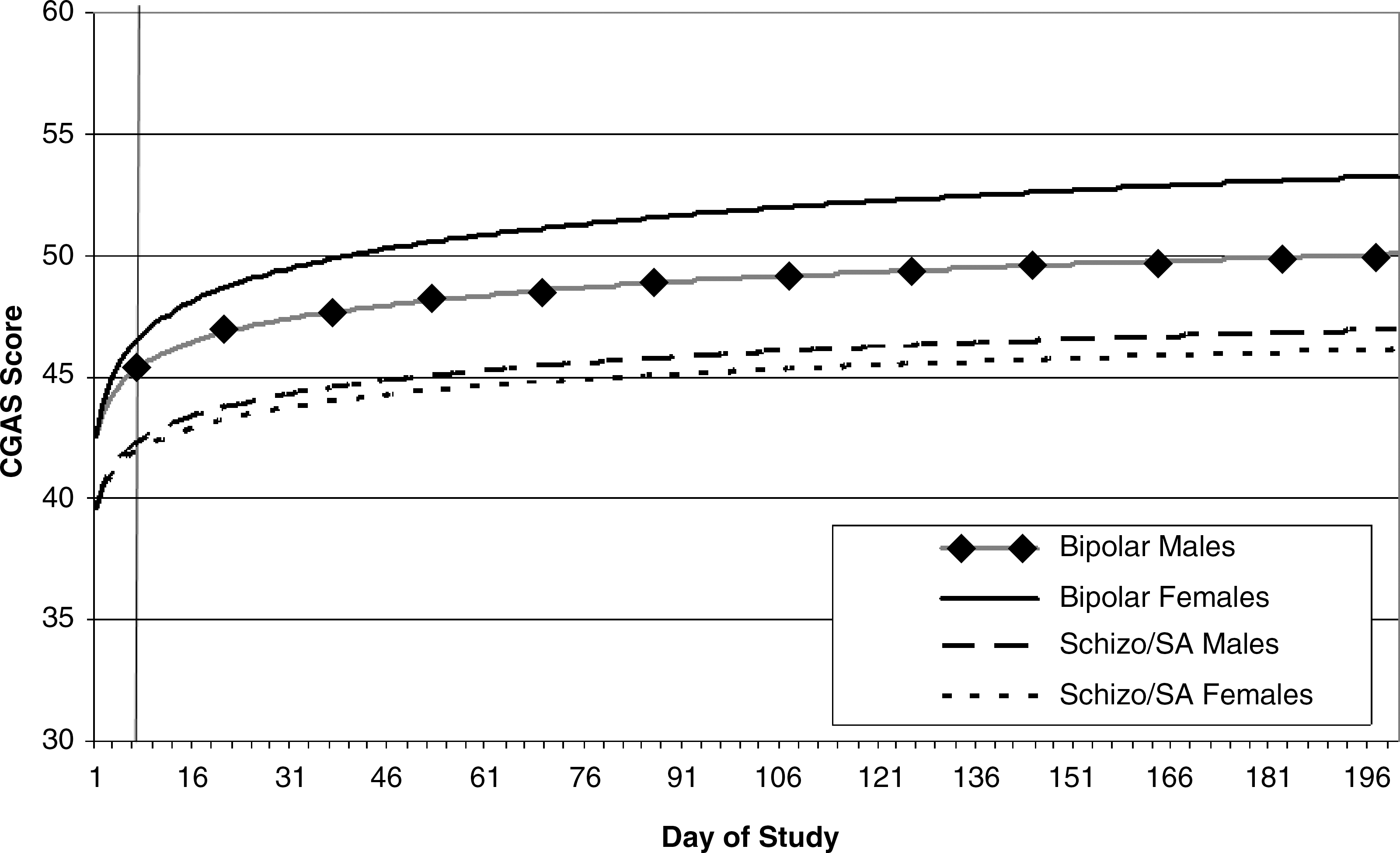
Exploratory mixed-model, random regression analysis: Final model with diagnosis and gender as predictors (p < 0.20). CGAS = Children's Global Assessment Scale; schizo = schizophrenia; SA = schizoaffective.
Discussion
The present study was conducted as part of a ziprasidone safety and tolerability trial and was a post hoc secondary analysis of exploratory end points to assess functioning and HRQOL in children and adolescents with BPD, schizophrenia, and schizoaffective disorder. As expected, subjects in this sample had substantial impairment in these domains at baseline.
Overall, greater impairment was observed on scales related to psychosocial functioning than for physical health, a pattern previously reported in adolescents with BPD (Rademacher et al. 2007). This difference between psychosocial and physical health reflects the clinical nature of these conditions, which have a high psychiatric burden while leaving physical functioning relatively intact. Across all three diagnoses in this study, parents reported adverse impacts on their time, emotions, and family activities due to their child's disorder, as indicated by these domains on the CHQ.
The CGAS was used to characterize the baseline level of functioning and to provide longitudinal assessment of drug benefit. The baseline means on the CGAS were notably lower than the recommended cut-off for normal functioning (score ≥70), indicating that subjects in all diagnostic groups demonstrated a high degree of impairment in several areas with inability to function in at least one area.
During treatment with ziprasidone, both dose groups achieved gains in functioning (CGAS) that paralleled symptom improvement as demonstrated by the efficacy measures (YMRS and BPRS-A), with most improvement in psychosocial functioning occurring early in treatment. Both the baseline means and the changes in response to treatment were consistent with findings from other trials of atypical antipsychotics in these populations (DelBello et al. 2002; Barzman et al. 2004; Pavuluri et al. 2005; Tillman et al. 2007).
The effect sizes for the change in functioning in both diagnostic groups were generally large, indicating potentially clinically meaningful improvement. Improvement in functioning was evident by the end of week 1 and was maintained over follow up. Though none of the subjects scored in the normal range on the CGAS at baseline, 5 subjects did so by the end of week 3.
Baseline CHQ and CGAS scores showed fairly low correlations with baseline scores on the symptom rating scales. Although higher levels of symptoms tended to be associated with greater impairment in functioning (e.g., on the CGAS), these correlations were not statistically significant. Thus, it appears that these two scales assess different constructs than the efficacy measures. However, there were parallel improvements over time in the CGAS and efficacy (YMRS and BPRS-A) measures, supporting the view that symptomatic improvement and improved functioning are related. While the results from this trial fill a gap in the literature, the raters in this trial were not blind to treatment. Open, unblinded trials such as this have a tendency to produce larger effects than blinded studies, and this may have impacted the results observed.
This study did not distinguish between inpatients and outpatients. Data on inpatient or outpatient status at the time of the assessment for this trial were not captured in the database, so we are not able to make comparisons. We note this as a limitation of the study. However, it also increases the generalizability of our findings.
The mixed-model, random regression analysis results showing that bipolar subjects have higher levels of functioning at baseline and that female bipolar subjects responded more rapidly are intriguing. The liberal p value used in building this model was in keeping with the exploratory nature of this analysis. However, the results should be confirmed in a larger study.
In summary, overall functioning and HRQOL are important aspects of functional recovery in youth with BPD and schizophrenia, but are not measured by current clinical assessment scales. In contrast, the CHQ and CGAS scales measure these domains. The CHQ and CGAS scores revealed clear deficits in these populations at baseline, and the CGAS demonstrated sensitivity to change over time in response to treatment with ziprasidone. Substantial gains were evident by week 1 and were maintained over time. These tools are useful supplements to standard symptom rating efficacy measures in clinical trials examining the use of antipsychotic medications for children and adolescents with psychotic and bipolar disorders.
Footnotes
Disclosures
Dr. DelBello has received research support from AstraZeneca, Eli Lilly, Johnson & Johnson, Shire, Janssen, Pfizer, Bristol-Myers Squibb, Repligen, Martek, Somerset, National Institute on Drug Abuse (NIDA), National Institute of Mental Health (NIMH), National Institute on Alcohol Abuse and Alcoholism (NIAAA), NARSAD, and the Thrasher Foundation. She is on the lecture bureau of Bristol-Myers Squibb, AstraZeneca, and France Foundation and has received fees for consulting, advisory boards, or honoraria from AstraZeneca, GlaxoSmithKline, Eli Lilly, France Foundation, Kappa Clinical, NIDA, Pfizer, and medical communications media. Drs. Stewart, Versavel, and Keller are or were employees of Pfizer. This study was supported by funding from Pfizer Inc. Editorial support was provided by J. Stamford, Ph.D., of PAREXEL and was funded by Pfizer Inc.