
Abstract
Objective:
The aim of this study was to evaluate the safety and efficacy of extended release carbamazepine (CBZ-ER) monotherapy in the treatment of pediatric bipolar disorder (BD).
Method:
This was an 8-week, open-label, prospective trial of CBZ-ER monotherapy (788 ± 252 mg/day) to assess the effectiveness and tolerability of this compound in treating pediatric bipolar spectrum disorders. Assessments included the Young Mania Rating Scale (YMRS), Clinical Global Impressions–Improvement scale, Children's Depression Rating Scale, and Brief Psychiatric Rating Scale. Adverse events were assessed through spontaneous self-reports, vital signs weight monitoring, and laboratory analysis.
Results:
Of the 27 participating children with BD, 16 (59.%) completed the study. CBZ-ER treatment was associated with statistically significant, but modest, levels of improvement in mean YMRS scores (−10.1 ± 10.2, p < 0.001) with end-point mean YMRS score (21.8 ± 12.2) suggesting a lack of complete resolution of mania. CBZ-ER treatment also resulted in significant improvement in the severity of depressive, attention-deficit/hyperactivity disorder, and psychotic symptoms. With the exception of 2 participants who discontinued due to skin rash, CBZ-ER was well tolerated with marginal increase in body weight (0.8 ± 2.5 kg, p = 0.04) and was not associated with any abnormal changes in laboratory parameters.
Conclusions:
Open-label CBZ-ER treatment was beneficial for the treatment of BD in children. Future controlled trials are warranted.
Introduction
Although the atypical antipsychotics (risperidone, olanzapine, aripiprazole, and quetiapine) have been increasingly used in the treatment of adults and youth with BD in recent years (Frazier et al. 2001; Keck et al. 2003; Tohen et al. 2003; Biederman et al. 2005; DelBello et al. 2006; Perlis et al. 2006), these treatments have also been associated with substantial adverse effects, especially weight gain, glycemic dyscontrol, dyslipidemia, and prolactinemia. This state of affairs calls for the further evaluation of additional safe and effective treatments for pediatric BD.
The antiepileptic agent carbamazepine (CBZ) has shown to be efficacious in the treatment of BD in adults with minimal propensity toward metabolic syndrome (Keck et al. 1992; McElroy and Keck 2000; Weisler et al. 2004; Weisler et al. 2005). CBZ is a tricyclic compound structurally related to imipramine. Although the precise mechanism by which CBZ exerts its therapeutic effects remains unknown, it has been suggested that its activity may be related to increased brain concentrations of γ-aminobutyric acid (GABA) by potentiating GABA receptors α1, β2, and γ2 subunits (Granger et al. 1995). Although earlier controlled trials of immediate-release CBZ (CBZ-IR) in adults were effective in the treatment of acute mania (Keck et al. 1992), most of these trials were either small or confounded by the concomitant use of other psychotropic agents. On the other hand, later trials of the extended-release form of CBZ (CBZ-ER) in adult populations with BD report efficacy in treating both mania and depression, including mixed state (Weisler et al. 2004; Weisler et al. 2005). The mood-stabilizing effect of CBZ, especially in those adults with mixed state, which is the typical presentation of the pediatric-onset BD, suggest that this medication may be well suited to treat the pediatric population with BD (Wozniak et al. 1995; Post et al. 1996).
Initial clinical evidence from case reports and uncontrolled trials suggests that, although CBZ-IR may be effective in the management of BD in the pediatric population (Garfinkel et al. 1985; Evans et al. 1987; Woolston 1999; Kowatch et al. 2000; Davanzo et al. 2003; Kowatch et al. 2003), it is associated with significant gastrointestinal distress and thus not well tolerated (Garfinkel et al. 1985; Evans et al. 1987; Stuppaeck et al. 1990; Post et al. 1996; Solomon et al. 1996; Weller et al. 2002).
Alternatively, CBZ-ER decreases the need for frequent administration and minimizes the daily fluctuations in serum concentration of CBZ (Canger et al. 1990; Stevens et al. 1998; Konsil et al. 2002), which has been shown to contribute to improved tolerability and treatment compliance in adult BD populations (Mirza et al. 1998; Miller et al. 2002; Ketter et al. 2004; Miller et al. 2004; Weisler et al. 2004; Ficker et al. 2005; Weisler et al. 2005). To date, there is no empirical evidence for the efficacy and tolerability of CBZ-ER in the treatment of BD in the pediatric population.
The main goal of this open-label pilot study was to evaluate the safety, tolerability, and effectiveness of CBZ-ER in the treatment of pediatric BD. We hypothesized that CBZ-ER would be effective and well tolerated in this population.
Methods
Subjects
This study was approved by the Human Research Committee at Massachusetts General Hospital. All subjects and parents/guardians provided written informed consent and assent after the study procedures, and possible side effects were fully explained.
Subjects were outpatients of both sexes, 6–12 years of age, with a diagnosis of for BD I, BD II, or BD not otherwise specified (NOS) with significant severity of current manic, hypomanic, or mixed symptoms on the Young Mania Rating Scale (YMRS) (total score of at least 20).
All diagnoses were established by clinical interview of the children and their guardians by an expert clinician supported by structured diagnostic interview using the Schedule for Affective Disorders and Schizophrenia for School-Age Children–Epidemiologic version (Orvaschel and Puig-Antich 1987) administered to the parent of the child. A diagnosis of BD I was based on the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association 1994) diagnostic criteria that require subjects to meet criterion A, an extreme and persistently elevated, expansive, or irritable mood for a period lasting at least 1 week, plus criterion B, manifested by three (four if the mood is irritable only) of seven symptoms during the period of mood disturbance. BD II was defined according to the DSM-IV as hypomania (an abnormal mood lasting at least 4 days), and BD-NOS was defined as a severe manic mood disturbance that did not meet either time criteria (an abnormal mood lasting at least 2 days or for shorter duration but is recurrent and severely impairing) or had fewer elements in criterion B (only required 2 items for elation and 3 for irritability).
Eligible children were required to have a YMRS (Youngstrom et al. 2002; Young et al. 1978) total score of ≥20 at baseline to enroll in the treatment trial. Rating scales were completed by board-certified or board-eligible child and adolescent psychiatrists who were trained to a high level of interrater reliability in weekly rater meetings. The intraclass correlation score for interrater reliability on the YMRS was 0.81.
We excluded subjects with any serious, unstable medical illness, including hepatic, renal, gastroenterologic, respiratory, cardiovascular, endocrinologic, neurologic, immunologic, or hematologic disease. Subjects with DSM-IV substance (except nicotine or caffeine) dependence within the past 6 months or who were judged to be at serious suicidal risk were also excluded from participation. No patient was entered into the study if adequately stabilized on an antimanic therapy. Mood stabilizers, anticonvulsants, and other neuroleptic therapy were not allowed during this study. Antidepressants were exclusionary to the study.
Administration of study medication
CBZ-ER was initiated at 200 mg/once daily and the dose was increased by 100 mg in the first 2 weeks and thereafter by 200 mg weekly per clinician judgment based on tolerability and response to a maximum dose of 1,200 mg/day, not to exceed either by body weight 35 mg/kg or serum concentration of >12 μg/mL.
Administration of concomitant treatments
Given the strong overlap of pediatric BD with attention deficit hyperactivity disorder (ADHD), methylphenidate hydrochloride, dextroamphetamine sulfate, and mixed amphetamine salts were allowed during the study if, in the clinician's judgment, it was in the best interest of the patients to continue this treatment or if the patient did not wish to stop stimulant treatment and only if the patient had been on a stable dose for at least 30 days. Three subjects enrolled in the study were receiving concomitant stimulant therapy. Nonpharmacological treatments such as individual, family, or group therapy were allowed if they were in place prior to participation in the trial, provided the status of the therapy regimen remained unchanged throughout the course of the trial.
Clinician-rated assessment scales
Severity of symptoms of mania was assessed weekly with the YMRS, as described above. Depression and psychotic symptoms were assessed at baseline, midpoint, and end point with the Children's Depression Rating Scale (CDRS) (Poznanski et al. 1979) and Brief Psychiatric Rating Scale (BPRS) (Lachar et al. 2001), respectively. To assess clinically significant severity and improvement relative to baseline, we used the National Institute of Mental Health (NIMH) Clinical Global Impressions–Severity (CGI-S) and –Improvement (CGI-I) scales (National Institute of Mental Health 1985). CGI severity and improvement were assessed separately for depression, mania, and ADHD. The score for the CGI-S ranges from 1 (normal, not at all ill) to 7 (among the most extremely ill patients). The score for the CGI-I ranges from 1 (very much improved) to 7 (very much worse).
Safety assessment
Safety was assessed at each visit using spontaneous reports of treatment-emergent adverse events, changes in vital signs, and laboratory measures. Blood pressure and weight were recorded at each visit. Electrocardiogram (ECG), electrolytes, liver function tests, and glucose levels were obtained at baseline and posttreatment. CBZ serum levels and complete blood count with differential were monitored at each weekly visit
Definition of clinical response
Response was defined by having either a 30% reduction in symptoms according to the YMRS at end point or by having been judged as “much improved” or “very much improved” on the CGI-I for mania (≤2).
Statistical analysis
Analyses were intention to treat (ITT). A mixed-effects model, repeated-measures approach was used to account for missing data in our longitudinal assessments of safety (i.e., weight and vital signs) and efficacy. Continuous and categorical data were tested with analysis of variance (ANOVA) and Pearson's c2, respectively for nonlongitudinal data (i.e., demographics at baseline, prevalence of adverse effects or response at end point, etc). Statistical significance was determined at p < 0.05.
Results
The 27 children enrolled in the study were 9.1 ± 1.9 years of age and predominantly male (70%, n = 19). Out of 27 subjects that enrolled in the study, 82% (n = 22) met the lifetime diagnostic criteria for BD I, 11% (n = 3) met the criteria for BD II, and 7% (n = 2) met the criteria for BD-NOS. At the time of participation, 67% (n = 18) were experiencing mixed episode (significant symptoms of co-occurring major depressive disorder), 22% (n = 6) were in manic episode, and 11% (n = 3) were in hypomanic episode.
All subjects were diagnosed with a bipolar spectrum disorder by clinical evaluation and had YMRS scores greater than 20. At study entry the mean YMRS score was 31.9 ± 6.4. Subjects also met lifetime diagnostic criteria for depression (74%, n = 20), ADHD (85%, n = 23), and psychosis (11%, n = 3) on structured diagnostic interview. Of the 27 subjects enrolled, 16 (59%) completed the 8-week course; dropouts were due to adverse effect of skin rash (n = 2), worsening severity of mania (n = 3), lack of efficacy (n = 3), loss to follow up (n = 2), or difficulties in meeting the study schedule (n = 1). At study end point, the mean dose of CBZ-ER was 788.2 ± 252.2 mg/day with a mean CBZ serum level of 6.6 ± 3.5 μg/mL (range: 0.5–12.3 μg/mL).
Figure 1 shows the adjusted weekly YMRS score. Mixed regression analysis demonstrated a statistically significant improvement from baseline after 2 weeks of treatment with further significant improvement for completers at week 8 (Fig. 1). Consistent with the high rate of drop out due to lack of efficacy or adverse effects, end-point (last observation carried forward, LOCF) analysis of YMRS scores suggested a statistically significant but modest response, however. CBZ-ER was also associated with a statistically significant improvement in the symptoms of both depression and psychosis as reflected by the change from baseline to end point in the mean scores of CDRS (34.8 ± 10.9 versus 26.9 ± 11.6; p = 0.001) and BPRS (40.1 ± 9.9 versus 30.0 ± 6.8; p < 0.001), respectively (Table 1). At study end point, 52% (n = 14) of subjects had a 30% reduction in baseline YMRS scores and 44% (n = 12) had a 50% reduction in baseline YMRS scores. A total of 34% (n = 9) of the participants achieved remission of mania symptoms as suggested by a YMRS score <12.

Change in Young Mania Rating Scale (YMRS) scores over 8 weeks of extended-release carbamazepine trial. There is a significant reduction in symptoms over 8 weeks of therapy (χ2 (8) = 285.3, p < 0.00001). *p < 0.001 versus baseline.
Abbreviations: CDRS = Children's Depression Rating Scale; BPRS = Brief Psychiatric Rating Scale.
As shown in Fig. 2, 33% of subjects were rated on CGI-I as “much improved” or “very much improved” at study end point on the symptoms of mania, 43% of children demonstrated improvement in symptoms of depression, and 62% demonstrated improvement in ADHD symptoms (Fig. 2). Last, the rate of antimanic response based on the a priori definition of response, i.e., either a 30% reduction in YMRS at end point or CGI-Mania Improvement of ≤2 was 63% (n = 17).
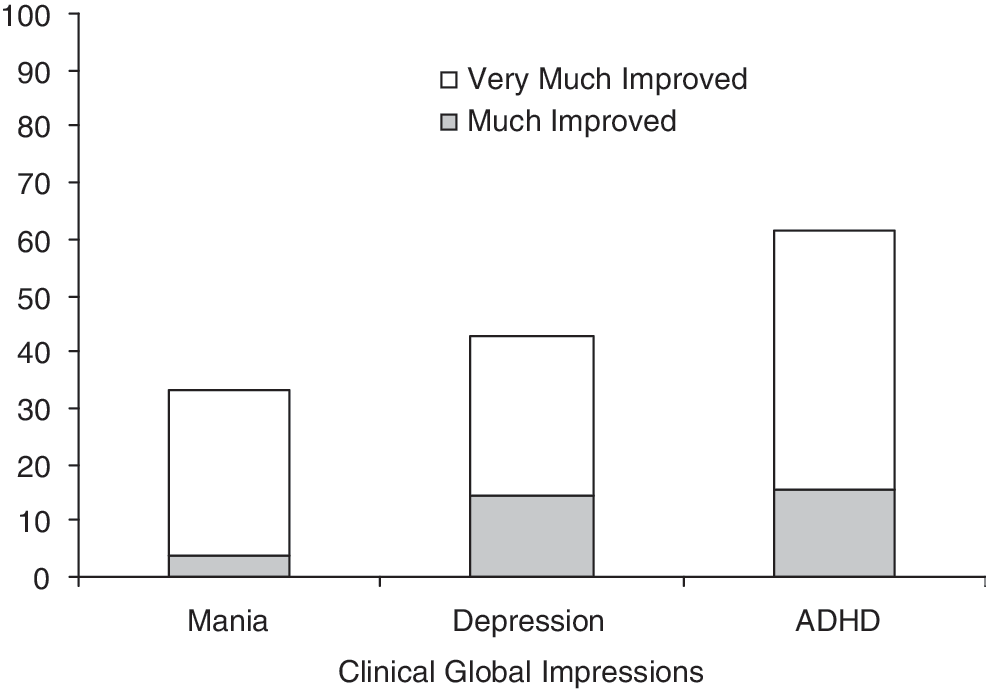
Clinical Global Impressions rated improvement in mania and psychiatric co-morbidity with extended-release carbamazepine trial.
Vital signs, weight, and electrocardiogram (ECG) parameters are presented in Table 2. There was a small but statistically significant prolongation in PR and QRS intervals from baseline to end point (PR interval from 130.4 ± 16.2 to 142.1 ± 14.6, p < 0.001; QRS interval from 81.2 ± 8.9 to 82.3 ± 8.9, p = 0.04), but no other statistically significant changes were observed in ECG parameters, blood pressure, or pulse (Table 2). With the exception of an increase in posttreatment platelet count in 1 participant, there were no abnormal laboratory values. Similarly, all the pre- and posttreatment platelet values were with in normal limits with the exception of 1 participant in whom the posttreatment platelet count increased from normal pretreatment count of 337,000 per cubic millimeter to an abnormal count of 540,000 per cubic millimeter. There was a statistically significant, but clinically modest, increase in weight of 0.8 ± 2.5 kg from baseline to end point.
degrees of freedom for weight, blood pressure and pulse (1,20) but for all other variables (1,9) due to missing data at endpoint.
Bazzett's Correction.
Abbreviations: bpm = beats per minute; ECG = electrocardiogram.
Adverse effects associated with CBZ-ER monotherapy are presented in Fig. 3. The most commonly reported adverse effects were headache (23%), gastrointestinal complaints (18%), cold symptoms (15%), sedation (15%), dizziness (8%), aches and pains (8%), and insomnia (4%). There were no serious adverse events reported during the course of the study. However, 2 subjects had to be discontinued from the study due to the development of skin rashes. An 8-year-old girl developed a generalized maculopapular, nonpruritic rash on 200 mg/day of CBZ-ER (serum level 4.9μg/mL). Another 7-year-old boy developed generalized pruritic petichiae on his legs and trunk on a CBZ-ER dose of 300 mg/day and was treated with oral benadryl. In both cases, rash developed within 2 weeks of exposure to CBZ-ER, did not involve mucosa, was nonprogressive in nature, and resolved within 1 week of discontinuing CBZ-ER. None of the participants in the trial developed serious rash (life-threatening, requiring hospitalization, Stevens–Johnson syndrome, or erythema multiforme).

Adverse effects associated with extended-release carbamazepine trial.
Discussion
This was a prospective, 8-week, open-label treatment trial of CBZ-ER monotherapy for the treatment of mania in 27 children with BD. Subjects participating in this study were predominently young (9.1 ± 1.9 years old) males (70%) with BD I (82%) experiencing significant symptoms of mania (YMRS 31.9 ± 6.4) and concurrent symptoms of depression (67%) and ADHD (82%). Intent to treat analysis showed that subjects improved significantly, albeit modestly, from baseline to end point in symptoms of mania as measured by rating scales and clinical global impression. In addition, CBZ-ER monotherapy was also associated with significant improvement in depression, ADHD, and psychotic smptoms. Although treatment with CBZ-ER was not associated with meaningful weight gain or prolongation of QTc interval, neurologcal and gastrointestinal adverse effects were common. These results suggest that CBZ-ER may be an effective and relatively well-tolerated treatment for children with BD and support the need for future controlled trials of this compond in the treatment of pediatric BD.
The overall antimanic response after 8 weeks of CBZ-ER monotherapy was generally less than robust compared to the rates of response observed with some atypical antipsychotics using similar protocols. For instance, in an open-label trial of aripiprazole for the treatment of pediatric BD, we reported 95% antimanic response rate on outcome measures using methodology identical to this trial (Biederman et al. 2007). Our findings documenting a moderate antimanic response to CBZ-ER are consistent with reports on modest antimanic effects of CBZ in pediatric and adult BD populations (Kowatch et al. 2000; Weisler et al. 2006). Kowatch and colleagues (Kowatch et al. 2000) conducted a 6-week open-label trial of CBZ-IR, lithium, and divalproex sodium in 42 children and adolescents with BD I or BD II, mixed or manic episode, and reported response rates of 53% for divalproex sodium and 38% for lithium and CBZ-IR monotherapy. These investigators also noted that the rate of response observed in the CBZ-IR group was higher on the YMRS criterion of ≥50% reduction from baseline (38%) than on the CGI improvement subscale score of 1 or 2 criterion (31%). Relatively similar patterns of response rates of mania on YMRS and CGI were observed in our study (YMRS ≥50% response in 44%, CGI 1 or 2 response in 33%). Similarly, the onset of response on CBZ-ER in the present study was also consistent with the onset reported after 2 weeks of CBZ-IR monotherapy in an adult population with BD (Vasudev et al. 2000).
It is not clear if the modest antimanic response rates were due to the participating population that was predominantly BD I versus BD II. This is noteworthy because there is some evidence from adult BD trials that CBZ-IR is more effective for the treatment of BD II than BD I (Kleindienst and Greil 2000). Modest antimanic response could also be a result of short duration of treatment trial that may not have allowed for optimal treatment response. Kowatch and colleagues (Kowatch et al. 2003) noted that all children who responded well to CBZ therapy in the acute phase continued to experience positive responses in the extension phase of the trial, suggesting that youths with BD may continue to experience an antimanic response with CBZ beyond the 8-week duration of our trial.
For the majority of subjects in our study, treatment with CBZ-ER was well tolerated at the mean dose of ∼788 (±252) mg/day, achieving a mean serum level of 6.6 (±3.5) μg/mL; this mean CBZ serum level achieved in this trial was within the therapeutic range of 4–12 μg/mL. In the present trial, participants who were considered responders, as per an a priori definition of response, achieved antimanic response on a mean CBZ serum level of 6.34 ± 3.4 μg/mL (range, 0.6–12.3 μg/mL). All the participants who completed the trial achieved end-point mean CBZ serum level: 7.08 ± 2.9 μg/mL (range, 0.6–12.3 μg/mL) were responders with the exception of 1 participant, who was considered a nonresponder with an end-point CBZ serum level of 7.7 μg/mL while receiving the maximum permitted dose of CBZ-ER (1,200 mg/day).
In general, mean values of all safety laboratory tests, including liver enzymes and platelet and leukocyte counts, remained within normal limits throughout the trial. The observed changes in values of the various safety laboratory parameters examined following CBZ-ER treatment were not clinically significant. It is particularly noteworthy that in acute treatment with CBZ-ER weight gain, although statistically significant, was minimal and clinically insignificant. Lack of clinically significant weight gain during the course of 8-week CBZ-ER monotherapy trial is particularly encouraging as compared to equally insignificant weight gain reported by the previous CBZ trials of briefer duration (3–6 weeks long) (Kowatch et al. 2000; Weisler et al. 2006). The adverse events reported in the present study were mostly mild to moderate. Headache was the most frequent adverse effect reported by one fourth of the participants (23%) followed by complaints of gastrointestinal distress (18%), sedation (15%), and dizziness (8%). The adverse effects reported in the present trial were remarkably similar to the incidence and frequency profile of adverse effects reported by the aforementioned CBZ-IR trial conducted by Kowatch and colleagues (Kowatch et al. 2000) in a pediatric population. The only exception was gastrointestinal distress, which was reported at a lower rate with CBZ-ER in our study (46% vs. 18%).
However, nearly half of the participating population (41%) dropped out of the trial. Two of the participating subjects (7%) dropped out due to adverse effects because they developed skin rash early in the treatment with CBZ-ER. The skin rashes developed within the first 2 weeks of the trial and resolved completely upon discontinuation of CBZ-ER. Of the 6 subjects who dropped out due to lack of response (half of them [n = 3, 11%] due to lack of efficacy and other half due to worsening severity of mania), 2 at the time of discontinuation had subtherapeutic serum CBZ levels (<0.5 μg/mL, 2 μg/mL). Although high, these rates of dropout are consistent with the high rates (42% dropout) reported in previous pooled results from controlled CBZ-ER trials of adult BD, including their rate of dropout due to adverse effect or lack of efficacy (10%), which are also close to the rates reported in this study (Weisler et al. 2006).
ECG parameters following treatment with CBZ-ER were within normal limits despite a statistically significant increase in the PR and QRS intervals following CBZ-ER treatment. Although statistically significant, these values were within in normal limits and were not associated with any cardiac symptoms in the participants. Furthermore, although CBZ therapy is associated with the risk of developing thrombocytopenia (platelet count <150,000 per cubic millimeter), platelet counts were increased in one half of the participants (56%) and decreased in the other (41%). These observed changes in the platelet counts were within normal range with an exception of asymptomatic abnormal increase in the posttreatment platelet count (540 th/cumm) in one participant.
In contrast to the modest overall antimanic effects of CBZ-ER, relatively stronger improvements were also observed in depression (43% on CGI-I and on CDRS [p = 0.001]), ADHD (62% on CGI-I), and psychotic symptoms (on BPRS p < 0.001). The antidepressant effects observed in this open-label trial suggests that CBZ-ER may have efficacy in treating the dysphoric component of the mixed manic state that characterizes pediatric-onset BD (Wozniak et al. 1995). The observed antidepressive response associated with CBZ-ER treatment in the present trial is consistant with the substantial evidence available from previous controlled trials indicating that CBZ-ER may be efficacious in improving the depressive symptoms of mixed episodes in adult populations with BD (Weisler et al 2004; Weisler et al. 2005).
Equally important is the observation that treatment with CBZ-ER may have significant anti-ADHD effects, considering that very high rates of ADHD co-morbidity are associated with pediatric BD (Biederman et al. 1996; Wozniak et al. 1997) and their treatment with traditional anti-ADHD agents has higher risk of exacerbating mania (Koehler-Troy et al. 1986; Schmidt et al. 1986; Soutullo et al. 2002). In the present trial, co-morbidity with ADHD was present in more than three fourths of the participants (85%), and the observed anti-ADHD response was consistent with the recent reports of risperidone suggested to be effective in treating ADHD symptoms in populations of youths with and without BD (Aman et al. 2004; Correia Filho et al. 2005; Biederman et al. 2008). Notably, in youths with BD, the anti-ADHD effect observed with CBZ-ER is superior to the modest anti-ADHD response observed with risperidone in a trial conducted at our center using similar methodology (Biederman et al. 2008). However, the high response rate of ADHD symptoms reported in the present trial on CGI-I could partially be attributed to the response in the overlapping symptoms shared between ADHD and mania (for instance, distractibility, motoric hyperactivity, and talkativeness). Future trials designed to address this issue may confirm our observation.
Although antipsychotic agents are often preferred for the treatment of the psychotic features in mania, scant information is available on the efficacy of of antiepileptic class of mood stablizers in the treatment of psychotic symptoms in individuals with BD (McElroy et al. 1996). In the present study, the psychotic features that in particular responded to CBZ-ER were grandiosity present in 67% of the participants (p < 0.001) and, to a lesser extant, suspiciousness (with a trend toward statistical significance, p = 0.062) present in 22% of the participants. Our findings of significant improvement in psychotic symptoms are consistent with the effectiveness of CBZ reported in BD adults with psychotic symptoms (Vasudev et al. 2000). The results of this study need to be considered in light of its methodological limitations. This was an open study; therefore, the assessments were not blind to treatment. Because the CBZ-ER dose titration parameters in the present trial were flexible and guided by tolerability and response and not by the serum levels of CBZ, this may have resulted in modest antimanic response on a mean serum level of CBZ that was toward the lower end of the theraputic range. It is possibile that forced titration of CBZ-ER to a higher serum level might be well tolerated and result in a more robust antimanic response. Half of the participants (52%) in the present trial were receiving concurrent psychotherapy, and, although a higher proportion of nonresponders were receiving concurrent psychotherapy than responders (80% vs. 35%), the possibility of antimanic response due to concurrent psychotherapy cannot be ruled out. Last, although reports of adverse effects were common in our data, our assessment of adverse effects relied exclusively on spontaneous reports by subjects and their parents.
Conclusions
This is the first open-label trial to evaluate the efficacy and tolerability of CBZ-ER in children with BD. Results showed modest antimanic effects and a somewhat better antidepressive and antipsychotic response to CBZ-ER monotherapy. In short-term monotherapy, CBZ-ER was well tolerated by children with BD. Although the overall adverse-effect profile was similar to that reported for CBZ-IR in youths with BD, the adverse effect of gastorintestinal distress occurred at a lower rate with CBZ-ER. Drop-out rates were high and were predominantly due to lack of response. Cognizant of our findings from this short-term, open-label trial that CBZ-ER treatment in children with BD is well tolerated, is not associated with clinically significant weight gain or glycemic dyscontrol, and has modest antimanic response along with significant antidepressant and anti-ADHD effect, we conclude that CBZ-ER may prove to be effective either as a monotheraputic mood-stablizing agent or in combination with other antimanic agents for the treatment of BD in children. Although firmer conclusions regarding the role of CBZ-ER in the treatment of pediatric BD await results from controlled clinical trials, open studies such as this represent an essential step in a rational drug development program aimed at pediatric BD. Further systematic research comparing CBZ-ER to placebo, mood stabilizers, and other atypical antipsychotics is needed to fully assess the short- and long-term safety and efficacy of this compound in the treatment of youths with BD.
Footnotes
Disclosures
Gagan Joshi, M.D., received a Ethel DuPont Warren Fellowship Award 2005–2006 and a Pilot Research Award from the American Academy of Child and Adolescent Psychiatry 2005, and awards from McNeil Pediatrics (CME sponsored by SynerMed Communications), Bristol Myers Squibb (Site PI for Multi-centered Trial), and Glaxo Smith Kline (Site PI for Multi-centered Trial). Dr. Joshi is a member of the national advisory board for Shire and is a subinvestigator for clinical trials sponsored by Shire, Johnson & Johnson, Pfizer, Merck, Cephalon, McNeil, Eli-Lily, Abbott, Novartis, Bristol Myers Squibb, Organon, Otsuka, Takeda, and New River Pharmaceuticals. Janet Wozniak, M.D., is the author of Is Your Child Bipolar, published May, 2008, by Bantam Books; is a speaker for the Primedia/MGH Psychiatry Academy; and is on the Advisory Board/Consulting for Pfizer and Shire. Her spouse John Winkelman, M.D., Ph.D., is on the Speakers Bureau for Boehringer-Ingelheim, Cephalon, GlaxoSmithKline, King, Sanofi-Aventis, Sepracor, and Takeda; is on theAdvisory Board/Consulting for Axon Labs, Boehringer-Ingelheim, GlaxoSmithKline, Jazz Pharmaceuticals, Luitpold, Novartis, Neurogen, Novadel Pharma, Pfizer, UCB (Schwarz) Pharma, Sepracor, and Takeda; and receives research support from Boehringer-Ingelheim, GlaxoSmithKline, UCB (Schwarz) Pharma, and Sepracor. Eric Mick, Sc.D., has received research support from McNeil Pediatrics, Ortho-McNeil Janssen Scientific Affairs, Pfizer, Shire Pharmaceuticals, and the National Institute of Mental Health (NIMH); and has an advisory and or consulting relationship with and Shire Pharmaceuticals, Pfizer, and Validus Pharmaceuticals. Robert Doyle, M.D., is on the Advisory Boards of Novartis, McNeil, Janssen, and Shire; is on the Speakers Bureau for Novartis, McNeil, Janssen, Shire, and Bristol Myers Squibb; and CME for Danemiller Foundation, Primed, Neuroeducational Institute, CME Outfitters, Ephikacy, and Phase Five Communications. Paul Hammerness, M.D., has been a speaker for, received research funds or participated in CME activities/professional talks supported byAbbott, Eli Lilly & Company, Forest Research Institute, Ortho-McNeil-Janssen, and Shire; has also received research funds from Elminda Ltd.; has also participated, as an investigator, in research studies in the past 2 years funded by Bristol Myers Squibb, Cephalon, Eli Lilly, GlaxoSmithKline, Johnson & Johnson, McNeil, New River, Novartis, Organon, Otsuka, Pfizer, Shire, and Takeda; and has also received honoraria from Reed Medical Education(a company working as a logistics collaborator for the MGH Psychiatry Academy). The education programs conducted by the MGH Psychiatry Academy are supported through Independent Medical Education (IME) grants from pharmaceutical companies co-supporting programs along with participant tuition. Commercial entities supporting the MGH Psychiatry Academy are listed on the Academy's website,
This study was an investigator-initiated project funded by Shire Development, Inc. (with principal investigator Joseph Biederman, M.D.). Additional contributions were from the Pediatric Psychopharmacology Council Fund and the Norma Fine Pediatric Psychopharmacology Fellowship Fund.