
Abstract
Objective:
The aim of this study was to identify the “real-life” prevalence of psychotropic medications in children and adolescents in Germany and related behavioral and emotional problems. Data from the nationwide representative National German Health Interview and Examination Survey for Children and Adolescents (KiGGS) were analyzed.
Method:
A total of 17,450 subjects aged 0–17 years from 167 communities were examined as part of the KiGGS in Germany between 2003 and 2006 to determine their use of antidepressants, antipsychotics, anxiolytics, and sedatives within the 7 days prior to being interviewed. Medication use was assessed by a medical doctor who conducted a computer-assisted personal interview (CAPI) with the parents, and related emotional and behavioral problems were assessed using the Strength and Difficulties Questionnaire (SDQ).
Results:
The overall prevalence for these medications was moderate (4.81/1000; 95% confidence interval [CI], 3.70–6.26), but prevalence varied across the different classes of drugs (sedatives > antipsychotics > antidepressants > anxiolytics). Rates of off-label use were high for antipsychotics and antidepressants. About 30% of the medication, especially sedatives, was used without prescription. Subjects using psychotropic medication obtained higher scores in the screening for emotional or behavioral problems than the total sample, but 40% of the children did not show abnormal scores.
Conclusion:
The indication for antipsychotics was mostly behavioral symptomatology, while antidepressants were used for a wide variety of symptoms. The high proportion of children and adolescents using psychotropic medication with normal scores in the emotional and behavioral screening was remarkable. It cannot be determined whether in these cases low scores were related to improvement in symptoms or whether medication was being misused.
Introduction
It is difficult to derive from health insurance data information the de facto use of medication, duration of use, as well as co-medication, particularly in relation to self-medication with “over-the-counter” (OTC) drugs. Medication that is prescribed but never used or used irregularly because of poor compliance or adherence is not detectable in these samples (Hack and Chow 2001; Hwang et al. 2003). Conclusions about indicated use, misuse, overprescribing, or undersupply of psychotropic medication should be drawn with caution if epidemiological data or prescribing data are not linked with the diagnoses or psychopathology of the users. The assessment of medication use in epidemiological surveys of children and adolescents has not, to our knowledge, been accompanied by screening for psychiatric symptoms, except in studies investigating special samples (Schmid et al. 2008). The use of measures for assessing children's psychopathology and emotional and behavioral problems, such as the Strengths and Difficulties Questionnaire (SDQ) (Goodman 1997), could clarify indications for the use of psychotropic medication. The SDQ is a useful, brief, reliable, and valid parent report measure (Goodman 2001), and its scores are correlated with other measures of psychopathology (Muris et al. 2003).
The aim of this paper was to determine prevalence rates and off-label use of psychotropic medication, specifically antidepressants, antipsychotics, anxiolytics, and sedatives in children and adolescents in Germany. Emotional and behavioral problems and psychopathological patterns of the users of psychotropic medication will be determined using the National German Health Interview and Examination Survey for Children and Adolescents (KiGGS) dataset, which provides a unique opportunity to link data from the pharmacoepidemiological assessment with the psychopathological screening of the children and adolescents and with parent reports about indication. All of the data on psychotropic medications that we report below refer to the following groups: Antidepressants, antipsychotics, anxiolytics, and sedatives. Data on stimulants and similar medication will be reported elsewhere.
Methods
Sample
The KiGGS study is a nationwide, representative, cross-sectional health interview and examination survey involving a total of 17,641 children and adolescents aged 0–17 years (mean 9.02, standard deviation [SD] 5.07). Participants were examined physically and tested. Parents, adolescents, and the children themselves when aged above 11 years, completed an extensive self-administered questionnaire, including psychological and social test instruments. The data were collected from May, 2003, to May, 2006, in 167 representatively selected sample points all over Germany (Kamtsiuris et al. 2007). The rate of participation was 66.6%. It was the aim of the KiGGS study to obtain, for the first time in Germany, conjunctive data on physical, psychological, and social health issues for the entire age range from 0 to 17 years. Socioeconomic status (SES) was classified using the Winkler Index for social strata into the categories “low,” “middle,” and “high” (Winkler and Stolzenberg 1999).
Measures
Psychotropic medication
Information about the use of any medication by children and adolescents within the last 7 days, the duration of use, and indication, as well as any improvement in symptoms achieved, was assessed by a computer-assisted personal interview (CAPI) with the accompanying parent (Knopf 2007). In our analysis, we used the data on psychotropic medication with the following Anatomic Therapeutic Chemical (ATC) Classification System codes: N06A and N06C (antidepressants and compound preparations), N05AA-N05AL and N05AX (antipsychotics), N05B (anxiolytics), and N05C (sedatives) (DIMDI 2004). Concomitant medication was examined, regardless of whether it belonged to one of the classes described above or to another type of psychotropic medication (e.g., stimulants) or whether it was administered based on another nonpsychiatric indication. Off-label use was defined as use without license for indication and/or age. Self-medication was defined as every use of a substance without a prescription from a physician or naturopath. No data on use of medication were available for 191 children and adolescents. These subjects were excluded from analysis. In 3 cases, data on duration of use and improvement were missing.
Psychopathological screening
The SDQ (Goodman 1997) is a short screening tool composed of 25 items, containing five different subscales measuring emotional problems, conduct problems, hyperactivity–inattention, peer problems, and prosocial behavior. Its psychometric properties are satisfactory to good (Goodman 2001). Each item of the SDQ is scored on a 3-point Likert scale. Aggregating all subscales except the scale on prosocial behavior yields the total difficulties score (TDS). It can be stratified into three classes: Abnormal (17–40 points), borderline (14–16 points), or normal (0–13 points) and indicates a global rating for emotional or behavioral problems within the last 6 months. In Table 1, we refer only to the TDS as an indicator of psychopathological symptoms due to the small number of participants using psychotropic medication. In the KiGGS Study, the SDQ was completed by parents of children and adolescents aged 3–17 years (Holling et al. 2007).
Missing SDQ-TDS: n = 8.
Missing SES: n = 7.
Abbreviations: SDQ = Strengths and Difficulties Questionnaire; SES = socioeconomic status; CI = confidence interval; SDQ-TDS = Strengths and Difficulties Questionnaire–total difficulties score.
Statistical analyses
For all drug classes under study, we calculated the prevalence defined as the proportion of reported medications used within the last 7 days per enrolled 1000 subjects. To generate representative results at the national level, survey weights were developed to be applied throughout statistical analyses (Kurth et al. 2008). Results were weighted for deviations in the net sample in relation to the general population (as of December 31, 2004) for age, sex, regional aspects (eastern vs. western Germany), and nationality (German vs. non-German). Weighting mainly resulted in correction for differences in age structure and disproportionately higher sample sizes in eastern vs. western Germany. All percentage values were weighted; absolute numbers were not weighted. Data about off-label use were not weighted and are presented in absolute numbers.
All statistical analyses were performed using SPSS software version 16.0. Analyses were performed using the complex samples option of SPSS to account for the sampling differences. Chi-squared tests were used to analyze the association between SES (low, middle, and high) and medication (groups: were no use of psychotropic medication and use of psychotropic medication). Differences in proportions and in means were evaluated using 95% confidence intervals. Non-overlapping confidence intervals were considered to be significant.
Results
General results
Parents reported the use of psychotropic medication (antidepressants, antipsychotics anxiolytics, and sedatives) within the last 7 days for 82 of the 17,450 children (Table 1). The prevalence of psychotropic medication was 4.81/1000 (95% confidence interval [CI], 3.70–6.26). Of the total of 14,589 drugs used by the minors in the study, 87 drugs belonged to the class of psychotropic medication (Knopf et al. 2007). Nearly half of these psychotropic medications were sedatives, whereas almost one third of all psychotropic medications were antipsychotics. The drug-treated prevalence was as follows: Antipsychotics, 1.09/1000; antidepressants, 0.71/1000; anxiolytics, 0.44/1000; and sedatives, 2.73/1000 (Table 1). The prevalence of psychotropic medication in general increased with age and peaked in the age group of 11- to 13-year-old children (prevalence/1000: 1.77 in 0–2 year olds, 2.59 in 3–6 year olds, 4.56 in 7–10 year olds, 8.02 in 11–13 year olds, 6.26 in 14–17 year olds). The parents of 53 boys (out of 8880) and of 29 girls (out of 8570) reported the use of psychotropic medication. More than 4 out of 5 (n = 18/22) users of antipsychotic medication were boys, which was a statistically significant difference in sex. Two out of 3 sedative users (n = 28/42) were boys, whereas 3 out of 4 (n = 9/13) antidepressant users were girls (Table 1) (no statistically significant difference). There was no statistically significant difference in SES between children and adolescents with and without psychotropic medication or between children and adolescents with abnormal TDS with and without psychotropic medication. The highest proportion of low SES was found in the group of subjects using antipsychotics, whereas the highest proportion of families with high SES was found in the antidepressant and sedative groups. Results are shown in Table 1.
Co-medication and self-medication
A total of 50 children and adolescents used further medication in addition to antipsychotic/antidepressant/anxiolytic/sedative medication; these were mostly medications for respiratory infections (ATC R), metabolic and nutritional systems (ATC A), and from class ATC N, but not from ATC N05 or N06. Some had taken as many as seven medications in the last 7 days. Combinations of psychotropic medications were two antipsychotic preparations (3 subjects), an antidepressant and an antipsychotic (1 case), or an antidepressant with a sedative (1 case). Five subjects received stimulants concomitantly with antipsychotics. None of the subjects using sedatives used concomitantly an anxiolytic, an antipsychotic, or a stimulant (ATC N06BA). In total, 65.3% of all psychotropic medication was prescribed by a physician; only 4.9% was prescribed by a naturopath. All other drugs, notably about 50% of the sedatives, were purchased without a prescription and taken as self-medication.
Off-label use and parent-reported indications for substance classes
With respect to stated indication and age, more than a third (32/87) of all drugs taken were used off-label. The rate of off-label use was highest for antipsychotics (16/25), followed by antidepressants (7/13) and sedatives (9/12). It was zero for anxiolytics. Parents reported a broad variety of symptoms in their children, which they named as the indication for the use of psychotropic medication. Six preparations could not be given on- or off-label status because of imprecise statements by parents. Indications for antipsychotics as stated by the parents varied widely and included tic disorder and behavioral problems (specifically, aggression or hyperactivity/attention deficit). None of the participants used them for symptoms associated with schizophrenic disorders. Tiapride was generally used for tic disorder. The other second-generation antipsychotics (SGA) used by study participants were olanzapine and risperidone. Low-potency antipsychotics were used by 7 minors. Antidepressants were not used exclusively to treat depressive disorders. Of these subjects who indicated the use of antidepressants, 3 younger subjects used imipramine for enuresis. Three of the other participants reported on-label use of a preparation (fluvoxamine for obsessive-compulsive disorder; St. John's Wort [SJW] for anxiety or problems with concentration). All anxiolytics were used for seizures or for allergic skin reactions. Some of sedatives were homeopathic formulations for treating hyperactivity, which are licensed in Germany. The other major group of preparations comprised valerian preparations for sleep disorders or restlessness. In one case, off-label melatonin was also used with the indication of sleep disorder.
Parent-reported behavioral and emotional symptoms
A high proportion (39.6%) of the children and adolescents using psychotropic medication did not show abnormal scores in the SDQ (Table 1). TDS and subscale scores in subjects with psychotropic medication were significantly higher than in those without psychotropic medication, except for the strength scale: Scores on the scale measuring prosocial behavior were significantly lower in subjects using psychotropic medication (Fig. 1). Stratified analyses of the SDQ and the various classes of the medication revealed that subjects who used anxiolytics and sedatives most frequently achieved normal TDS and SDQ-subscale scores, whereas users of antidepressants and antipsychotics were more likely to obtain abnormal TDS scores and SDQ-subscale scores (Table 1). Differences between users and nonusers of psychotropic medication in TDS and subscale scores were significant across all drug classes (except for the users of anxiolytics), but between drug classes, differences were not significant, possibly due to small group numbers resulting in large confidence intervals (Fig. 2).

*SDQ: Total number of participants without psychotropic medication, available SDQ, and available SDQ of users of psychotropic medication.
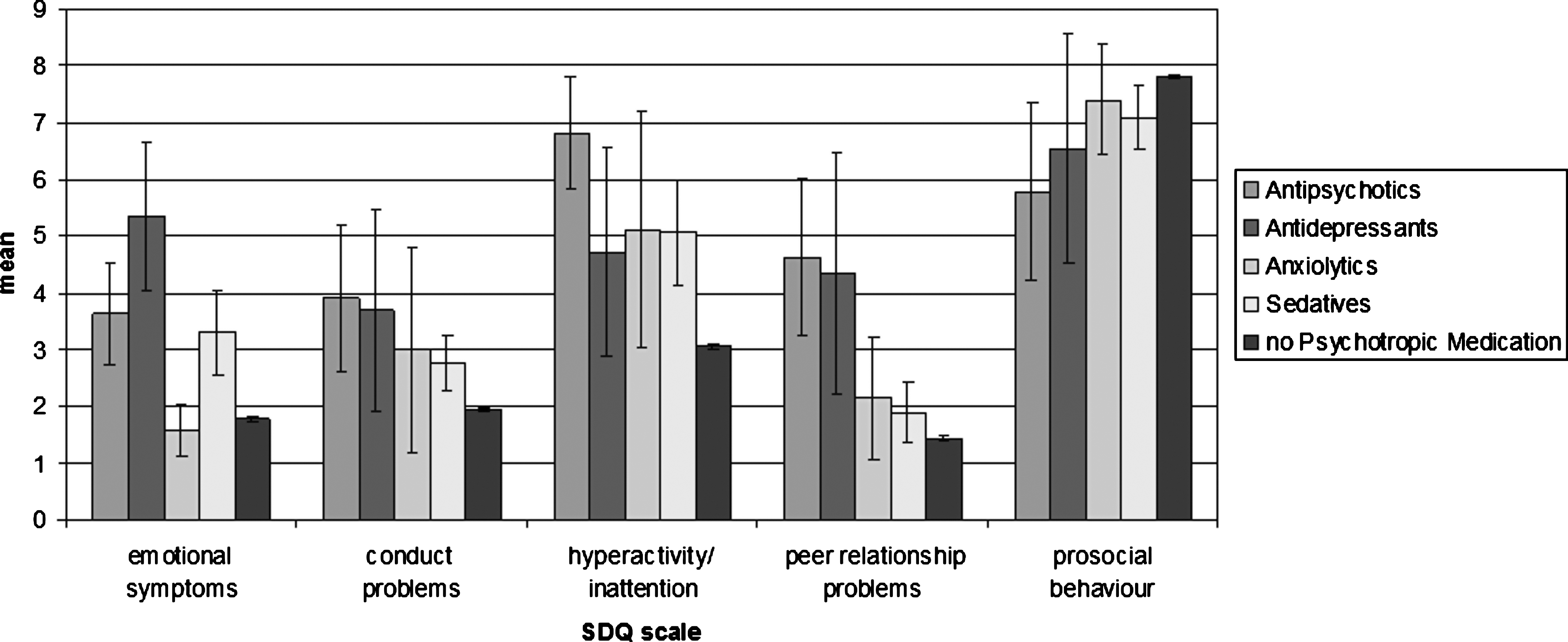
SDQ mean scores and use of psychotropic medication: Means of subscales related to drug classes. Mean and CI (95%). SDQ = Strengths and Difficultures Questionnaire; CI = confidence interval.
Duration of medication use and parent-reported improvement of symptoms
Sedatives, the most frequently used class of drug in our sample, were generally used for a short period (53.5% >1 week, 16.8% >1 month). Antipsychotics (86.6%) and antidepressants (56.5%) were used in most cases for longer periods (>1 month to ≥1 year). In all, 31.2% of the parents reported a great improvement in their children's symptoms due to the medication and 58.0% a partial improvement. In all drug classes, reported rates of nonresponding to medication were rather small (0% for antidepressants and anxiolytics, 5.6% for antipsychotics, 7.4% for sedatives).
Discussion
There is no evidence of widespread use of antipsychotic, antidepressant, anxiolytic, and sedative medication by children and adolescents in Germany. Previous reports about national differences are supported by these results, and, compared with studies of children based on health insurance samples, a 1-week prevalence in our study is low (Zito et al. 2006; Volkers et al. 2007). Other inclusion criteria (most studies included youths of up to 19 years old, and prevalence increases between the age of 18 and 19 years) and the use of a point-prevalence (last 7 days) might explain the differences (Harrison and Britt 2005; Zito et al. 2006; Volkers et al. 2007). In contrast to adults, prevalence for anxiolytics was low and there was no sign of misuse, but surprisingly sedatives were the most preponderant of all psychotropic medications. Next to homeopathic and anthroposophic preparations for hyperactivity (Zappelin®), valerian preparations were the sedatives used most frequently. This mirrors the growing trend to use nonsynthetic psychotropic medications, especially in children (Cala et al. 2003). Also in antidepressants, nearly a third comprised herbal preparations of SJW. This trend toward herbal/anthroposophic psychotropics was related to an excessive self-medication in sedatives, but this was not the case for antidepressants. About 30% of psychotropic medication was used without prescription. Physicians need to be aware of these concomitant medications.
Making up a third of all used antidepressant medication, the proportion of tetracyclic antidepressants was lower than in previous studies and, for the first time, a higher rate of use of SGAs in children and adolescents in Germany emerged. The off-label rate in our sample exceeded the quantity known to be used in outpatients in general pediatrics (Bucheler et al. 2002). The high rate of off-label use of antipsychotics reflects the increased use of second-generation preparations, none of which was licensed for young people at the time of the study, except risperidone for behavioral use in mentally retarded children.
The highest prevalence for antipsychotics in male subjects aged 11–17 years corresponds to the typical sex distribution for antipsychotics being used to treat behavioral symptoms (Cooper et al. 2004; Alacqua et al. 2008). However, the high proportion of older male adolescents prescribed antipsychotics for behavioral symptoms is inconsistent with the assumed course of disruptive disorder and a decline of symptoms with increasing age. Discontinuation due to side effects is common (Alacqua et al. 2008), but in our study, stated adherence both in users of antidepressants and users of antipsychotics was high and most of the subjects used the medication for a long period.
Low SES is a predictor for behavioral and emotional problems in children and adolescents and for an elevated risk of psychiatric problems (Holling et al. 2007), but it was not a factor influencing the risk of using psychotropic medication. Subjects using psychotropic medication can be considered to correspond to a clinical sample, for which an up to four-fold elevated risk for high or abnormal scores in screening instruments can be expected (McCann et al. 1996; Schmid et al. 2008). Even if SDQ scores do not correspond to psychiatric diagnoses, diagnoses generated by the SDQ show a moderate to high agreement with clinically assessed diagnoses and can indicate emotional or behavioral problems (Mathai et al. 2002; Mathai et al. 2004). Consistent with this, those participants in the KiGGS who used psychotropic medication obtained significantly higher means in the SDQ-TDS as well as in subscales; subjects using antipsychotics and antidepressants obtained a higher proportion of abnormal or borderline scores. However, contrary to our expectations, about 40% of the children and adolescents using psychotropic medication did not obtain an abnormal score in the SDQ-TDS. Abnormal scores in the subscales measuring hyperactivity and peer problems among subjects using antipsychotic medication would support the hypothesis of behavioral symptom treatment. Even if the indication for use of the antidepressant given by the parents was not depression, about 70% of children and adolescents with antidepressant medication obtained abnormal scores in the SDQ subscale for emotional problems (Fig. 2). The users of different classes of psychotropic drugs are distinct from each other in their SDQ scores, but without statistical significance. No clear specific pattern of distribution of the SDQ scores in relation to the class of psychotropic medication was observed in our study.
The study is based on a representative nationwide sample and assessed complete medication use, including nonprescribed self-medication of children and adolescents. Furthermore, a psychopathological screening was conducted. These are clear strengths of the study compared with data derived, e.g., from health insurance information. Even though the number of identified subjects is small (and CIs are large), due to the study's design, the results remain representative.
A limitation of the study design—a survey where participants were asked to visit the survey office—is that a relevant group of users of psychotropic medication, e.g., severely ill adolescents with schizophrenia, were unlikely to participate. Therefore, the prevalence for antipsychotics may be moderately higher. Diagnoses or indications were not validated by a diagnostic examination by psychiatrists or experienced staff. All symptoms and indications were reported by the parents of the participants. The use of parent assessment is common in identifying psychopathology in child and adolescent psychiatry, but, in some cases, parents may not be a reliable source of information. Some misdiagnoses or false indications may be included in the sample, as well as some cases where the use of medication is not detected because of missing responses. The clinical efficacy of the medication was not rated by independent assessors. Indicated adherence to, or persistence with, prescriptions was not validated by further examinations. Use of medication may have influenced the low rate of psychopathological symptoms as assessed in the SDQ: Some of the children and adolescents using medication may have already obtained therapeutic benefit from it. Antipsychotic and antidepressant medications were generally used for a longer period, and recipients may not have continued to present with an abnormal SDQ-TDS. However, the high proportion of normal SDQ scorers among psychotropic medication users could also be a sign of inappropriate use of psychotropic medication.
Conclusion
Prevalence of the real use of psychotropic medication by children and adolescents in Germany assessed by a direct survey is low. Even though children using antipsychotics and antidepressants obtained a high rate of abnormal scores in a psychopathological screening (SDQ-TDS) and subjects using psychotropic medication had elevated scores in the difficulties subscales of the SDQ and lower scores in the strength scale, 40% attained no clinically relevant scores on the SDQ. The parent-reported high efficacy of medication might explain the high proportion of normal SDQ scores in our sample, but the normal scores could also indicate a remarkable proportion of children and adolescents using medication without a correlate of psychopathology.
Disclosures
Michael Koelch is an employee of the University Hospital of Ulm and this research was done without conflict of interest. He has received research grants in the last 5 years from BMFFSJ, Schweizer Bundesamt für Justiz, Eli Lilly International Foundation, Boehringer Ingelheim, and Europäische Akademie; was clinical investigator in trials of Eli Lilly, Astra Zeneca, and Janssen-Cilag; and received travel grants or payments for lectures by Janssen-Cilag, University of Rostock, DGKJPP, UCB, and various nonprofit organizations. Anja Prestel, Hanneke Singer, and Ferdinand Keller are employees of the University Hospital of Ulm and have no conflicts of interest or financial ties to report. Joerg M. Fegert has received unrestricted research grants from state and national governmental organizations and from the Volkswagen Foundation, Eberhardt Foundation, Eli Lilly Foundation, Janssen, and Celltech/USB. He has been involved in clinical trials with Janssen, Medice, Lilly, and Astra Zeneca; serves on a DSMB for Pfizer; and has received travel grants from or served as a consultant for Aventis, Bayer, Bristol-MS, J&J, Celltech/USB, Lilly, Medice, Novartis, Pfizer, Ratiopharm, Sanofi-Synthelabo; VFA & Generikaverband, the Vatican, National Institute of Mental Health (NIMH), AACAP, DFG, EU, and European Academy. Robert Schlack, Heike Hoelling, and Hiltrud Knopf are employees of the Robert Koch Institute have no conflicts of interest or financial ties to report.