
Abstract
Background:
Methylphenidate (MPH)-related adverse events are well characterized. Their predictors and their relationship with therapeutic effects are less well understood. Here we examine these issues in relation to two long-acting formulations.
Method:
Comparison of Methylphenidates in the Analog Classroom Setting (COMACS) was made in a large (n = 184) placebo-controlled trial comparing Equasym XL®/Metadate CD®, Concerta®, and placebo (PLA) using a Laboratory School protocol. Therapeutic effects were measured using direct observation, scores on a simple math productivity task and parent ratings. Parents also completed the Barkley Stimulant Side Effect Rating Scale (BSSERS).
Results:
The BSSERS had six factors: Emotionality, sleep/appetite, disengaged, dizzy, uninterested, and aches. Treatment effects were seen only for emotionality (which improved) and sleep and appetite (which worsened). Adverse events were not predictable from personal and clinical characteristics of patients. Sleep/appetite adverse events were not associated with therapeutic effects. Improvements in attention-deficit/hyperactivity disorder (ADHD) and emotionality were correlated.
Discussion:
The results support a narrow conceptualization of MPH adverse events with problems restricted to appetite and sleep. These effects were not predictable on the basis of available information and may be due to an underlying mechanism rather distinct from those determining therapeutic effects.
Introduction
Despite the apparent importance of understanding the causes and clinical relevance of these common MPH adverse events, they have seldom been studied in depth. Whereas researchers conducting clinical trials are obliged to enquire about and systematically record all such events that occur during a trial, the relationships with therapeutic effects and between different adverse events are rarely investigated.
The evidence as to whether adverse events are dose dependent is mixed. For instance, Stein et al. (2003) found evidence that insomnia and appetite loss were found only at higher doses in a randomized, controlled, dose–response study. This evidence was consistent with the notion that adverse effects may be determined by dose-sensitive pharmacological processes in a somewhat similar way to therapeutic effects. There was also evidence for an increase in the severity as dose was increased in the Multisite Multimodal Treatment Study of Children with Attention-Deficit/Hyperactivity Disorder (MTA) dose titration study (Greenhill et al. 2001a). In contrast, Karabekiroglu et al. (2008), in an open-label prospective study, found no dose-related adverse events. Furthermore, these authors looked at a range of possible predictors of adverse events and found that only the presence of co-morbid conduct problems was related to an increased risk of such effects. In a similar way, in a retrospective study, Weber et al. (2003) found no correlation with daily dose and that co-occurring emotional symptoms predicted higher levels of adverse effects. Putative genetic predictors of adverse reactions have been identified. For instance, McGough et al. (2006) demonstrated that an increased risk of irritability and social withdrawal was associated with variants of genes related to the dopamine receptor system. Stein et al. (2005) found that side effects varied as a function of the DAT1 polymorphism, while Leddy et al. (2009) found this genotype to be a moderator of the effect of drug treatment on food intake.
In the light of the scant information about the predictors of MPH adverse reactions, the current paper addresses the following questions. First, what is the relationship between different types of adverse events? Are there distinctive patterns of adverse reactions to MPH with some ADHD patients, for example, having problems with sleep while others have no problems in these areas of functioning but do have problems with both irritability and increased emotionality? These questions were addressed by examining the patterns of co-variation between parent-reported ratings of different types of adverse effects using principal component analysis. Second, can adverse events be predicted by personal characteristics (such as age and sex) and clinical factors (such as the presence of co-morbidity)? There has been a considerable degree of interest in the predictors of therapeutic response to MPH on the grounds that identifying those factors that predispose to a good response may make it possible to target therapies more accurately (see, for instance, Jensen et al. 1999; Owens et al. 2003). Given the importance of minimizing adverse reactions in establishing the optimal dose of MPH, it seems equally important to explore whether there are any predisposing characteristics within the child or their particular presentation that determine the profile of adverse events.
Finally, we examine the extent to which the magnitude of therapeutic effect of MPH is related to the levels of adverse events. Do those patients with the best therapeutic response also show the highest levels of adverse events? Are there patients who have a good therapeutic response but no adverse events? If adverse effects are produced by the same pharmacological processes that operate for therapeutic effects, one might expect that the best response is associated with the largest increase in adverse events. However, it is also possible that the dose–response curves for these two effects are dissociable from each other, with some subjects being sensitive to the therapeutic effects at lower doses than those that are required for adverse events to occur, whereas for others the converse is true. Here we also focus on two more specific questions. First, whether the relationship between adverse and therapeutic effects differs as a function of the source of information; i.e., we make a comparison of parents' subjective ratings as the index of therapeutic change versus a more independent and objective laboratory classroom scores. One might expect parental ratings of therapeutic effects to be affected by other factors besides change in ADHD symptoms. For instance, it is possible that where adverse effects are judged to be present this may feed into an overall judgement of reduced efficacy on the part of parents, creating an artificial and misleading lessening of the medication effect. Second, we were also interested in testing whether the relationship between therapeutic response and adverse events was dependent on the time of day at which measures were taken. In particular, we were interested in testing whether therapeutic effects as measured at the end of the day are related to evening and night-time situated adverse effects, such as insomnia and reduced appetite.
The analysis is based on data from the Comparison of Methylphenidates in the Analog Classroom Setting (COMACS) study (see Methods section). Four papers have been published so far using data from the COMACS study. The primary analysis of COMACS (Swanson et al. 2004) confirmed the above pharmacodynamic (PD) predictions for effects across the day. A secondary analysis (Sonuga-Barke et al. 2004) found that when patients were compared across dosing strata, to approximately match their immediate release (IR) components, then the Equasym XL®/Metadate CD® (EQXL-MCD) advantage in the early part of the day over Concerta® (CON) was minimized. A third paper reported sex differences, with girls showing a faster onset of action in the early day followed by a shorter duration of action (Sonuga-Barke et al. 2007) when other factors were controlled, and the effects of the two formulations were combined. A fourth paper explored individual differences in the PD of the formulations using growth mixture modeling and highlighted the existence of distinctive PD patterns defining subgroups of patients (Sonuga-Barke et al. 2008).
Methods
The COMACS study was a multicenter, randomized, crossover trial comparing two long-acting MPH formulations with distinctly different dosing profiles, EQXL-MCD and CON, against placebo (PLA) using a laboratory classroom-based instrument to study treatment effects across the day. The formulations are distinctive in their profile of MPH release, leading to different durations of action (EQXL-MCD is designed to have approximately an 8-hour action, whereas CON is designed to have a 12-hour action). Furthermore, with equivalent daily doses (and assuming early morning dosing), one would expect EQXL-MCD to have a larger effect in the earlier part of the day (given its higher IR dose element; 30% vs. 22%) and CON to have a larger effect in the evening given its larger extended release (ER) dose element.
Patients
Six- to 12-year-old children, receiving treatment with doses of MPH between 10 and 60 mg/day (5–20 mg per administration, one to three times a day) were recruited for the multisite COMACS trial. The subjects were screened and enrolled by the principal investigator at each study site. Children were deemed otherwise healthy on the basis of an extensive medical history and physical examination. Diagnosis of ADHD was confirmed by a clinical research interview carried out by a trained interviewer. Children were excluded if they had an intelligence quotient (IQ) below 80 or the inability to follow or understand study instructions. Other exclusion criteria included severe mental disorder (e.g., psychosis, bipolar illness, pervasive developmental disorder, severe obsessive compulsive disorder, or severe depressive disorder), extreme aggressive behavior or destruction of property, marked anxiety, tension, or agitation. Co-morbid psychiatric diagnoses were established at the screening visit by reference to Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association 1994) criteria (see Swanson et al. 2004 for details). A total of 184 patients (48 female) entered the trial. Eighty-two percent of the patients met criteria for ADHD combined type, 15% met criteria for inattentive type, and the remaining 3% met criteria for hyperactive/impulsive type. Approximately 25% of the children had a co-morbid condition (e.g., anxiety and oppositional defiant disorder). At prescreening, 54% of patients were on the three times a day (t.i.d.) equivalent formulation of CON and 23% on the twice a day (b.i.d.) equivalent formulation of EQXL-MCD. The remainder were taking IR formulations. Children provided signed assent, and their legal guardians signed an institutional review board–approved consent form to participate in the study.
Design
COMACS was a 10-site, double-blind, placebo-controlled, crossover study comparing three treatment conditions: EQXL-MCD, CON, and PLA. Dose-level assignment was made according to the prestudy clinically titrated daily dosing regimen for MPH and remained at that level for the study duration. Children treated with low doses (<20 mg/day) of MPH were randomized to receive a daily dose of EQXL-MCD 20 mg, CON 18 mg, or PLA; those treated with medium doses (>20 mg/day to 40 mg/day) were randomized to receive EQXL-MCD 40 mg, CON 36 mg or PLA; and children treated with high doses (>40 mg/day) were randomized to receive EQXL-MCD 60 mg, CON 54 mg, or PLA. Each of the three treatments was administered for 7 days (in the assigned sequence) without an intervening washout period, and the PD assessment was conducted on the seventh day of each treatment.
Assessment
Laboratory classroom assessment
For full details of the laboratory school assessment used in the COMACS trial, see Swanson et al. (2004). Outcomes were the Swanson, Kotkin, Atkins, M-Flynn, Pelham (SKAMP) scale giving ratings of deportment and attention, and a measure of productivity on a simple math task (Permanent Product Math Test [PERMP]) (Swanson et al. 1998).
Parent rating of ADHD symptoms
Parents of the children also completed the Swanson, Nelson & Pelham scale (SNAP version IV) (Swanson 1992), which has 39 items derived from the DSM criteria for ADHD and opposition defiant disorder (ODD). Parents responded on a Likert scale rating the presence of these symptoms. Making use of only the DSM-IV symptoms, the scale yielded ADHD-related factor scores for inattention and hyperactivity-impulsivity. The SNAP scales were administered twice during each treatment week on days 3 and 6. SNAP ratings on day 6 were used in the current analysis as these were completed after a longer period of exposure to the drug.
Parental ratings of adverse events
The Barkley Stimulant Side Effect Rating Scale (BSSERS) (Barkley et al. 1990) was also administered on day 6 of each treatment week and completed by the child's parent or guardian. This is a 17-item scale of commonly reported adverse events thought to be associated with ADHD, including insomnia, appetite, physical symptoms such as head and stomach aches, and emotionality and irritability on a scale of zero to nine (0 = no adverse event; 9 = very serious or frequent adverse event).
Initial data treatment
Missing data were handled on a case-by-case/analysis-by-analysis basis to maximize the power for each individual test. There was no replacement of missing data, but for each case missing values for SKAMP and PERMP were accommodated where possible by excluding them from the calculations of mean scores for a particular variable (e.g., morning or evening response), so that only patients with missing data for a whole period or condition were excluded from the analysis. For all analyses for each measure, our primary outcome is the treatment response calculated by subtracting PLA scores from active drug scores (either CON or EQXL-MCD) on the SNAP, SKAMP, PERMP, and BSSERS measures. For the purposes of the analysis, the laboratory classroom day data from the SKAMP and PERMP was partitioned into four segments to reduce the number of tests carried out: First thing (0 hours), morning (1.5–4.5 hours), afternoon (6.0–7.5 hours), and evening (12 hours). This approach was justified because preliminary analysis found no differences in patterns of correlations between different individual testing points within the morning and afternoon periods. Statistical significance was adjusted to control for multiple testing.
Results
The structure of co-variation between different adverse-events: Can they be seen as a single entity?
To explore the structure of covariation between different adverse events, we ran a principal component analysis on all the items on the BSSERS. For this analysis, differences were calculated for each item between PLA and active drug treatments (to capture treatment-related rather than ADHD-related effects). To simplify the analysis, the combined treatment effects for the CON and EQXL-MCD were used. Six independent factors were identified with eigenvalues over 1. Table 1 reports item-to-factor loadings with a varimax rotation (i.e., items with scores of over 0.4). The factor loadings were interpretable and were labeled: factor 1, emotionality; factor 2, sleep/appetite; factor 3, disengaged; factor 4, euphoric/dizzy; factor 5, uninterested; factor 6, aches.
Note: adverse-effect scores were derived by taking placebo scores from active drug scores and then taking the mean for the two active drugs.
Abbreviation: BSSERS = Barkley Stimulant Side Effect Rating Scale.
Did levels of adverse events differ between PLA and active drug conditions on the six derived BSSERS factors?
Factor scores were calculated by using items loading above 0.4 with cross-loading items (i.e., those correlating with more than 1 factor) being excluded. Scores were z-transformed before aggregation. All items loading above 0.4 were given equal weighting. The data were submitted to a two-way analysis of variance (ANOVA) with treatment condition (EQXL-MCD vs. CON) and dose as the between subject factors. There was a highly significant effect of dose on the sleep/appetite factor scores (F[2,174] = 5.12; p = 0.007); the higher the dose, the more adverse effects reported. The dose effect for the other factor scores did not reach significance (p values <0.98, >0.06). All subsequent analyses included dose level as a factor. Figure 1 shows the mean score for the six factors. There was no overall effect of formulation (F[1,172] = 0.01; p = 0.972), with both EQXL-MCD and CON giving similar overall scores for adverse events. There was a very significant effect of factor score (F[5,860] = 11.52; p < 0.001). This effect was largely accounted for by major differences in the effects of treatment on adverse events in the sleep/appetite domains.
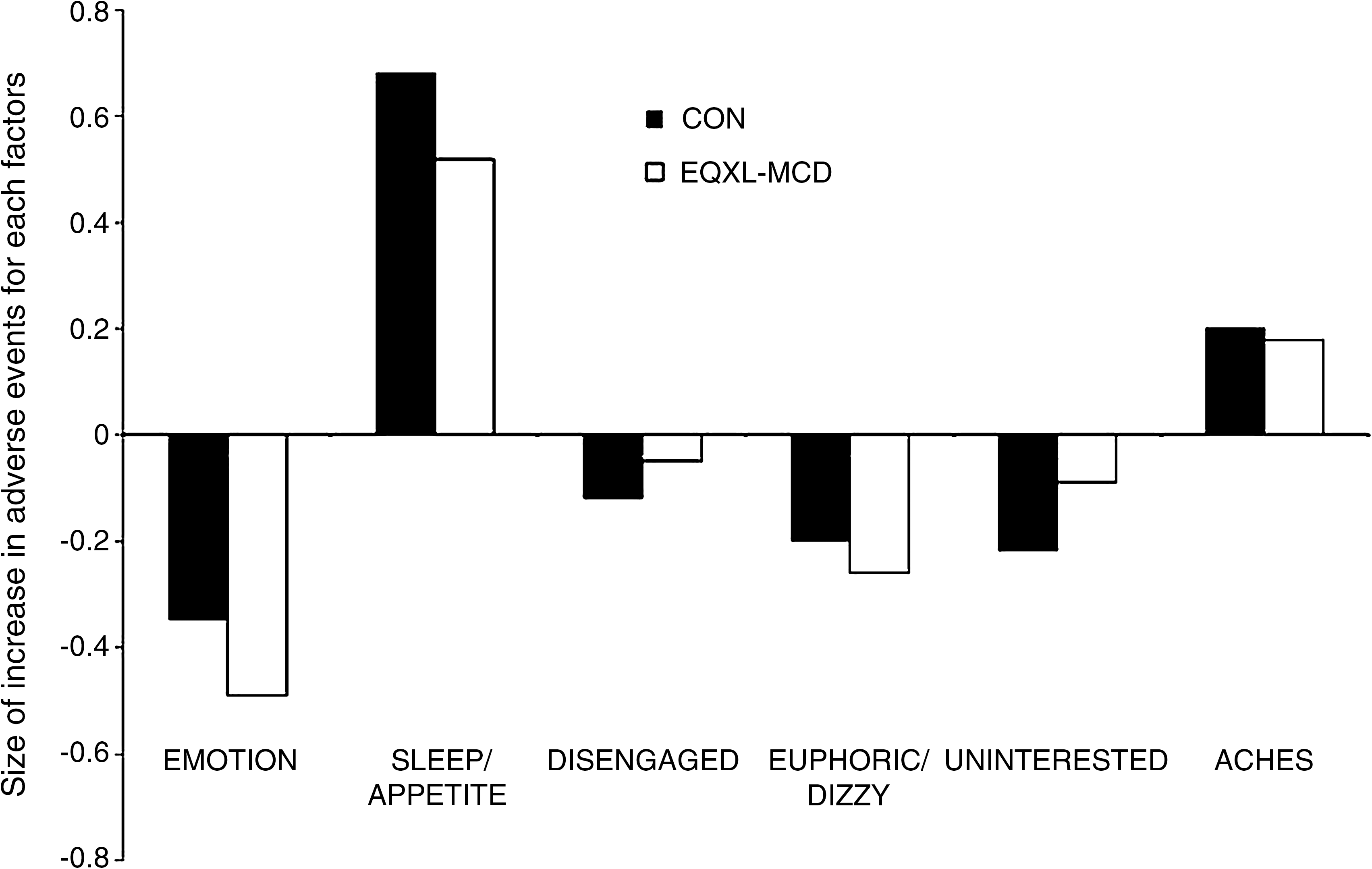
The differential effects of EQXL-MCD and CON in the different adverse-effect domains. EQXL-MCD = Equasym XL®/Metadate CD®; CON = Concerta®. Note: Negative scores represent reduction in ratings.
Single-sample t-tests were performed to see if effects deviated significantly from zero (i.e., no effect). These showed that sleep problems/poor appetite were significantly worse overall on active drug as compared to PLA (t CON [175] = 5.17; p < 0.001; t EQXL-MCD [173] = 3.41; p = 0.001). In the emotion domain, symptoms of anxiety and tearfulness improved significantly on active drug as opposed to PLA (t CON [175] = 2.31; p = 0.022; t EQXL-MCD [173] = 3.18; p = 0.002). The treatment effects for the other factors failed to reach significance (p > 0.054 < 0.69). The interaction between formulation and adverse-event factor was not significant although there was trend in this direction (F[5,806] = 2.83; p = 0.095). CON had a somewhat less beneficial effect in terms of reduction of emotional symptoms and a somewhat more detrimental effect with regard to sleep and appetite problems, although these effects did not reach significance individually (p > 0.220). When appetite/sleep-related items were entered individually the results remained the same for item 1 (insomnia and trouble sleeping; p = 0.005) and item 6 (decreased appetite; p < 0.001). There was no effect for item 2 (nightmares).
Although there are no validated cut offs for the BSSERS to estimate the absolute levels of adverse events reported in this domain, we used a cut-off score of 4 or more on each item. Using these cut offs, 32.37% of patients' parents reported insomnia and trouble sleeping on CON, 30.64% on EQXL-MCD, and 21.97% on PLA. For decreased appetite the figures were 37.57% (CON), 31.79% (EQXL-MCD), and 19.65% (PLA). The equivalent rates for emotional items were; irritable, 31.40%, 30.23%, and 44.77%; sad/unhappy, 16.96%, 14.04%, 12.87%; prone to cry, 19.08%, 14.45%, 21.97; anxious, 21.39%, 19.08%, 34.68%. Thus, reductions were found specifically with irritable (p = 0.001) and anxious (p < 0.001). There were no other differences between the two formulations in any other adverse-effect domain. All of the reported effects were unaffected by dose level assignment.
Can adverse-events be predicted by personal and clinical characteristics?
To examine this, we restricted the analysis to those two adverse event domains showing significant PLA-active treatment differences in the above analyses—emotionality and sleep/appetite problems. These were included as the outcome variables in multiple regression analyses. Age, sex, height, weight, and whether or not patients had co-morbid ODD or anxiety, as the most common co-morbidities in this sample, were included as predictors. For sleep/appetite problems (combined CON and EQXL-MCD scores), neither the overall model (R 2 = 0.014; F[5,171] = 0.47; p = 0.795) nor any individual predictor accounted for a significant proportion of the variance in adverse-effects (b < 0.12; p > 0.10). The same was true for the emotion domain (R 2 = 0.015; F[5,171] = 0.54; p = 0.745; b < 0.10; p > 0.25). There were no differences in these patterns of effects at the different dose assignment levels.
To what extent are adverse-events correlated with measures of therapeutic response? Do these correlations vary as a function of the type of rating and the time of day they are made?
Table 2 presents the correlations between side-effect scores in the two domains showing significant PLA–active treatment differences and the measures of therapeutic response taken during the COMACS trial (SNAP, SKAMP, and PERMP). There were no a priori grounds for expecting adverse events and therapeutic effects to be correlated differently for the two MPH formulations; thus, the scores for the two formulations were aggregated for this analysis. Preliminary analysis supported this view. Overall there was limited evidence that adverse events were related to therapeutic effects. Only SNAP ratings showed significant statistical effects and then largely in relation to emotionality; where ADHD symptoms were rated as being improved, so too were emotional effects. Only SNAP inattention scores were correlated with ratings of sleep/appetite problems. Taking account of multiple testing, there was no significant correlation between the laboratory classroom measures (SKAMP and PERMP) and adverse event ratings.
Note: Correlations are based on the differences between placebo and active drugs combined for the two formulations of methylphenidate. Boldface signifies significant effects after controlling for multiple testing.
Abbreviations: BSSERS = Barkley Stimulant Side Effect Rating Scale; SNAP = Swanson, Nelson & Pelham scale; SKAMP = Swanson, Kotkin, Atkins, M-Flynn, Pelham scale; PERMP = Permanent Product Math Test.
Discussion
The current results provide a number of important insights into the nature of side effects of MPH in the treatment of ADHD. First, items on the BSSERS clustered in meaningful and interpretable ways. On the face of it, this means that MPH adverse events are not a unitary construct and that different children are affected in different ways on different dimensions. Nevertheless, sleep and appetite problems, items most commonly found to be exacerbated by MPH, did form a single factor. Children who showed sleep-related adverse-events also showed appetite-related adverse-events. Furthermore, it was for this factor, and only this factor, that adverse events were significantly raised in the active treatment compared to the PLA arm. This pattern of results appears to diverge somewhat from some previous reports demonstrating adverse effects across a broader range of domains measured in the current study. However, it has been suggested that apparent effects in these domains may reflect pretreatment levels of impairment in ADHD-related domains more than they do the adverse effects of MPH; that is, they are not adverse effects of MPH per se, but rather characteristics of the disorder. Furthermore, if this were the case, then finding that sleep and appetite effects load on the same factor may be simply because these are the two actual adverse effects of the drug and they therefore share variance; there is no reason to suppose that they should be related to areas of functioning unaffected by MPH.
Second, while sleep and appetite problems significantly increased as a function of treatment, those on the emotionality scale significantly decreased. This replicates a recent finding by Karabekiroglu et al. (2008), who found that in an open-label trial “irritability,” “proneness to cry,” “anxiety,” “nail biting,” and “euphoria” all significantly decreased from baseline after 15 days of MPH treatment. Greenhill et al. (2001a) also found a similar effect. These effects are consistent with the literature that sees these items as baseline characteristic of ADHD (Efron et al. 1997) and also with previous evidence for the therapeutic benefits of MPH on emotional liability (Waxmonsky et al. 2008). While strictly speaking these beneficial effects on emotionality are side effects, in the sense that they are not the intended treatment target, they are not adverse events as typically understood. This suggests the need for a reformulation of the instruments currently used to measure adverse events. The question of whether the effects of MPH are directly pharmacological or rather a secondary effect of the core therapeutic changes in ADHD symptoms cannot be addressed on the basis of the available data.
Third, within the limitations of these exploratory analyses, there were no statistical significant differences between the two formulations on any factor. However, there was a trend toward an interaction between domain and formulation. EQXL-MCD demonstrated somewhat smaller effects on sleep-related adverse effects and somewhat greater improvements in emotional problems than CON, although these individual effects did not reach significance. Assuming that the sleep/appetite effects are pharmacological effects that are related to the serum level of MPH at any particular time, one would predict that CON's longer duration of therapeutic action should be mirrored also by side effects in the latter part of the day. Inasmuch as residual levels of MPH may remain in the evening and at bedtime, one might therefore predict more side effects of this nature with longer- rather than shorter-acting preparations. In this sense, the data are certainly of interest and warrant further study in randomized, controlled trials powered to show significant effects in terms of sleep/appetite adverse events. In this, we could test the crucial question of whether adverse events, like therapeutic effects, can be predicted on the basis of MPH plasma levels. Do MPH formulations with different profiles of action across the day also have different profiles of adverse events across the day? More specifically, are formulations with shorter durations of action across the day associated with reduced evening-related adverse events in the appetite and sleep domains?
Fourth, adverse-event scores were not predictable on the basis of the background or clinical characteristics available. This finding mirrors, in some ways, the largely unsuccessful attempts that have been made to predict therapeutic effects of MPH. It has not been possible to consistently identify those factors that might allow treatments to be targeted more effectively to those individuals who will benefit the most. In the same way, it would be useful to tailor treatments toward those individuals who will suffer the least adverse effects. We were unable to identify any factors at the level of the clinical presentation or the physical characteristics of the patients that provided a basis for such developments.
Fifth, adverse events (sleep/appetite) were, in general, not either positively or negatively related to therapeutic effects. Those who benefited most from medication in terms of symptom reductions were not those who have the most adverse events or vice versa. In this sense, different mechanisms and processes may be operating for the positive and negative effects of medication. In contrast, there were relatively strong associations between positive side effects (the reduction of emotional problems) and ratings of ADHD symptoms improvements, providing further support for drawing a distinction between the mechanisms underpinning the positive and negative effects of MPH.
There were a number of limitations of the current study. First, and most significantly, the study only included patients who were already being successfully treated with MPH. This means that severe and marked adverse events are unlikely to be seen in this study, and it is possible but that the lack of effects on BSSERS factors other than sleep/appetite may occur more readily in medication-naïve patients. The trial was also underpowered for detecting rare events that could be severe. Furthermore, if this were to be the case, we may find a different underlying structure of side effects with all items correlating more closely. Second, it is important to recognize that this was a secondary analysis of a study powered to show the nonequivalence between the two MPH formulations in terms of efficacy and not in terms of adverse events. Adverse events will show smaller effects than therapeutic effects, and a properly powered study is required to provide definitive answers. Third, measures of adverse events were derived only from parent ratings and not from direct observations of behavior.
There is an ongoing debate as to the most appropriate way to elicit and record side effects (Greenhill et al. 2001b). The use of questionnaire measures such as BSSERS that provide a more systematic assessment of adverse events have been called for (Levine and Schooler 1992). However, such measures are inevitably prone to bias, and more objective measures using, for instance, polysomnography/sleep diaries and food intake charts will add considerably to future studies of this kind. Also there may have been significant side effects that were not measured by the BSSERS, and so findings are limited to those covered by the BSSERS items. Finally, although we have explored the PD of therapeutic response to MPH using the laboratory classroom, measurement in that setting did not explore the temporal structure of adverse events. It may be that adverse events are greater in the morning (soon after dosing) than in the afternoon or in the evening, and it is possible that these effects mirror changes in the pharmacokinetics (PK)/PD relationship.
In summary, the current results support a rather narrow conceptualization of MPH adverse events with problems restricted to appetite and sleep, the most common effects reported in other studies. MPH had positive effects on emotionality that were correlated to therapeutic effects in relation to ADHD symptoms. No predictors of MPH adverse events emerged, and these were not, on the whole, associated with clinical response in terms of ADHD symptom reduction. Future research should explore the pharmacological basis of MPH adverse events and also their PD relationship to MPH PK.
Footnotes
Disclosures
Edmund Sonuga-Barke is currently a consultant for Shire pharmaceutical and UCB-Pharma; has in the last 3 years received grant funding from Janssen Cilag, UCB-Pharma, and QB-tech; has recently served on the advisory boards for Shire pharmaceuticals, UCB-Pharma, and Flynn Pharma; and has spoken at events sponsored by UCB-Pharma, Shire Pharmaceuticals, and Janssen Cilag. David Coghill is currently a consultant for Shire Pharmaceutical; has in the last 3 years received grant funding from Shire Pharmaceutical and Eli Lilly; has recently served on the advisory boards for Shire Pharmaceuticals, UCB-Pharma, Eli Lilly, Pfizer, and Flynn Pharma; and has spoken at events sponsored by UCB-Pharma, Eli Lilly, Flynn Pharma, and Janssen Cilag. Jim Swanson is or has been a consultant for Elli Lilly & Co, McNeil, Shire, Cephalon, Celltech, UCB, and Novartis; he has received grant funding from McNeil, Shire, Cephalon, Celltech, UCB, and Novartis; he has received speakers fees from McNeil, Shire, Cephalon, Celltech, UCB, and Novartis. Tim Wigal has since January, 2008, received research support and consulting honoraria from Eli Lilly, McNeil, Otsuka, and Shire. In the past 10 years, he has received research support, consulting honoraria, and/or speaker's bureau from the following pharmaceutical companies: Celltech, Cephalon, Eli Lilly, Janssen, McNeil, Novartis, Otsuka, and Shire. He has no stock or equity interests. In addition Tim Wigal has or currently received funding from the National Institute of Mental Health (NIMH), National Institute of Child Health and Human Development (NICHD), and National Institute on Drug Abuse (NIDA). Marc DeBacker is a full-time employee of UCB-Pharma.