
Abstract
Objective:
The effects of a promising pharmacological treatment for attention-deficit/hyperactivity disorder (ADHD), atomoxetine, were studied on executive functions in both ADHD and reading disorder (RD) because earlier research demonstrated an overlap in executive functioning deficits in both disorders. In addition, the effects of atomoxetine were explored on lexical decision.
Methods:
Sixteen children with ADHD, 20 children with ADHD + RD, 21 children with RD, and 26 normal controls were enrolled in a randomized placebo-controlled crossover study. Children were measured on visuospatial working memory, inhibition, and lexical decision on the day of randomization and following two 28-day medication periods.
Results:
Children with ADHD + RD showed improved visuospatial working memory performance and, to a lesser extent, improved inhibition following atomoxetine treatment compared to placebo. No differential effects of atomoxetine were found for lexical decision in comparison to placebo. In addition, no effects of atomoxetine were demonstrated in the ADHD and RD groups.
Conclusion:
Atomoxetine improved visuospatial working memory and to a lesser degree inhibition in children with ADHD + RD, which suggests differential developmental pathways for co-morbid ADHD + RD as compared to ADHD and RD alone.
Clinical Trial Registry:
B4Z-MC-LYCK, NCT00191906;
Introduction
Stimulants are widely used in the pharmacological treatment of ADHD. Because stimulants affect the striatum, they show abuse and addictive potential (Volkow 2006). An effective alternative pharmacological treatment to methylphenidate (MPH) is the noradrenaline reuptake inhibitor atomoxetine, which shows no risk of abuse because its site of action is presumed to be in the prefrontal cortex and it does not increase dopamine in the nucleus accumbens (Bymaster et al. 2002). Although the effects of atomoxetine on ADHD symptoms have been promising and tested extensively, the effects of atomoxetine on executive functioning are less studied than those for MPH (Aron et al. 2003; Bedard et al. 2004; Kratochvil et al 2006).
As far as we know, no studies have been reported that have investigated the effects of atomoxetine on executive functioning in children with ADHD. Only in adults with ADHD does there exist some evidence for beneficial effects of atomoxetine on inhibition (Spencer et al 1998; Faraone et al. 2005; Chamberlain et al. 2006; Chamberlain et al. 2007). One aspect of inhibition, interference control, as assessed by the Stroop Color and Word task, has been shown to improve after 10 weeks of atomoxetine treatment in comparison to placebo (Spencer et al. 1998). Faraone et al. (2005) found weak evidence for an interference effect of atomoxetine in comparison to placebo in subjects who scored relatively poorly at baseline.
Improved inhibition in adults as assessed by Stop Signal Reaction Time (SSRT) has been reported by Chamberlain et al. (2006, 2007). In both studies, SSRT improved (became faster) following a single dose of atomoxetine (60 mg) in healthy male volunteers as well as in adults with ADHD compared to placebo. Atomoxetine, however, showed no beneficial effects on visuospatial working memory (Chamberlain et al. 2007). This was surprising because a substantial body of research suggests that noradrenaline manipulations in both animals and humans may affect component processes of working memory (Coull et al. 1995; Arnsten and Li 2005). The hypothesized role of noradrenaline has emphasized the maintenance of information in visuospatial working memory as measured by a delayed response task (Arnsten and Li 2005). Chamberlain et al. (2007) used the Cambridge Neuropsychological Test Automated Battery (CANTAB) Spatial Working Memory task, which requires manipulation of information in working memory and strategy implementation, possibly explaining the absence of effects of atomoxetine on visuospatial working memory.
In the present study, we focused on the beneficial effects of atomoxetine on the maintenance function of visuospatial working memory and inhibition in children with ADHD. Visuospatial working memory was measured by the Corsi Block Tapping test, a measure that taps on maintenance of information (Schellig 1997). Inhibition was assessed by SSRT (Oosterlaan et al. 1998). To establish whether atomoxetine has effects on ADHD symptomatology, a 28-day treatment period of atomoxetine was chosen.
No other study has yet tested the effects of medication in a co-morbid ADHD + RD or RD only groups. We tested the effects of atomoxetine in children with co-morbid ADHD + RD and children with RD only. In addition, improvements in visuospatial working memory and inhibition possibly lead to improvements in reading, as assessed by a lexical decision task, because working memory and inhibition are related to reading (Gijsel et al. 2004; Savage et al. 2007). Thus, the present study assessed the effects of atomoxetine on lexical decision. The outcome of the effects of atomoxetine in ADHD and RD may give indications of the validity of the hypothesized common etiology of ADHD and RD. For example, if atomoxetine is equally effective in children with ADHD and RD, this may suggest a common etiology (Willcutt et al. 2005). However, when atomoxetine treatment is differentially effective in children with ADHD only or RD only or ADHD and co-morbid RD, this indicates that co-morbid ADHD + RD is a different disorder than ADHD or RD alone (Purvis and Tannock 2000).
The first goal of the current double-blind, placebo-controlled, crossover study was to investigate the effects of atomoxetine in children with ADHD, ADHD + RD, or RD on visuospatial working memory and inhibition. A second goal was to study the effects of atomoxetine on reading in children with ADHD, ADHD + RD, or RD. To obtain more homogeneous groups, only children with the combined subtype of ADHD were enrolled. Participants with other co-morbid disorders other than RD and oppositional defiant disorder (ODD) were excluded.
Method
Participants
Children in the ADHD and ADHD + RD groups were recruited via six pediatric outpatient clinics in The Netherlands and one pediatric outpatient clinic in Belgium. Children in the RD group were recruited via advertisements, because these children were not regularly seen by pediatricians. A total of 16 children with ADHD, 21 children with RD, and 20 children with ADHD + RD completed the study. Figure 1 displays eligible patients and reasons for dropout. In addition, 26 normal controls, who were recruited in regular primary schools, participated. The sample consisted of 102 children aged 8–12 years. Any child who dropped out during the study was not entered in the analyses. Written informed consent was obtained from the parents and from the child if aged 12 years. The study was approved by the national research ethics committee in The Netherlands and the local research ethics committee of the participating sites.
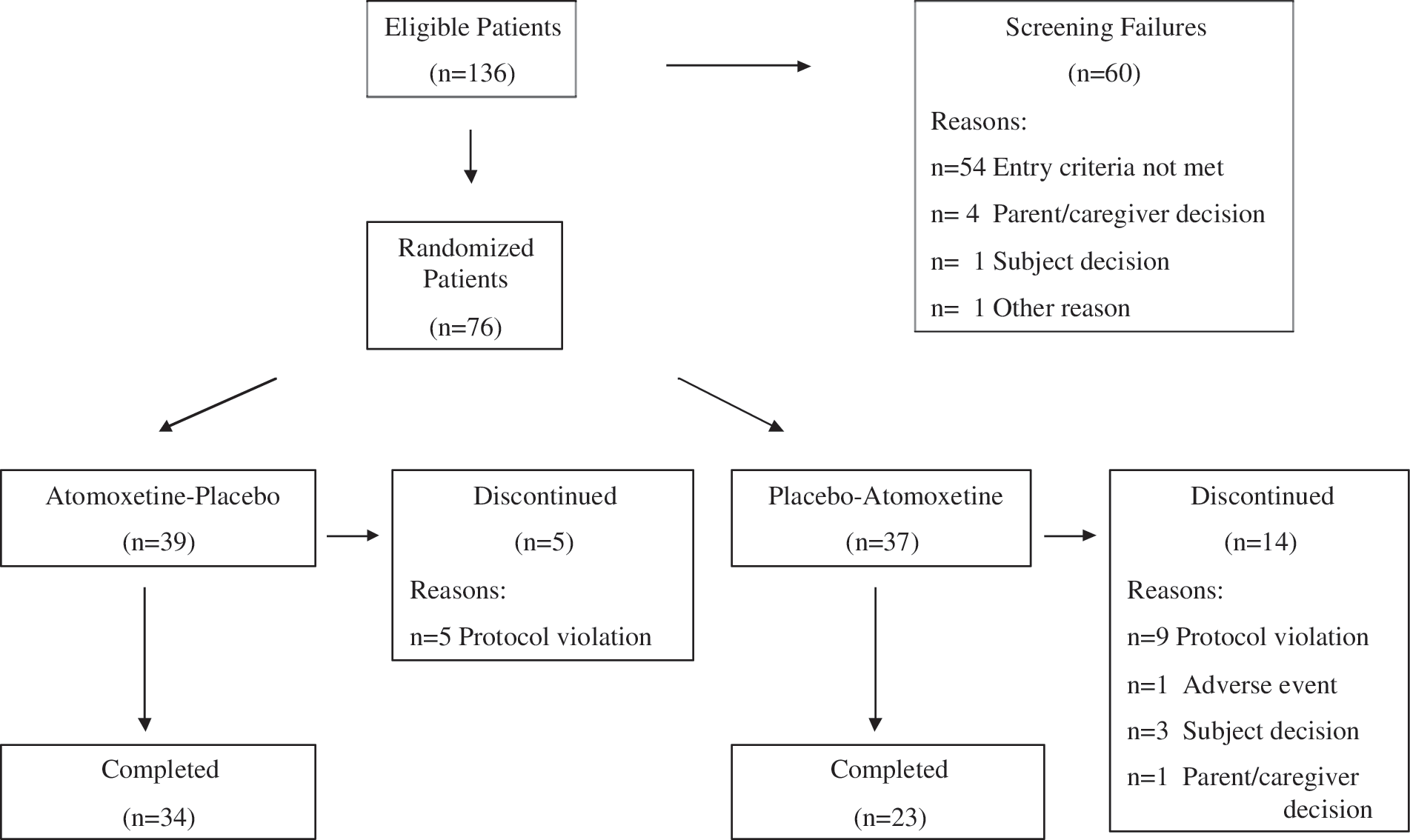
Patient flow diagram for the children that received treatment.
Study procedure
The study consisted of two periods: Period I was the washout period, if children were already on medication, and the screening phase, in which informed consent was obtained and potential eligibility determined. Eleven children in the ADHD group and 4 children in the ADHD + RD group received MPH prior to this study. Period 1 had a duration of 1–62 days. In Period II, the children with ADHD, ADHD + RD, and RD were randomly assigned to the two treatment orders: Placebo–atomoxetine or atomoxetine–placebo. Each treatment (placebo or atomoxetine) lasted 28 days and was interspersed by a washout period of 14 days. The (neuro)psychological measures were administered on the day of randomization and immediately after the 28-day periods. Normal controls performed the neuropsychological tests twice with an interval of 28 days.
Medication
Placebo and atomoxetine were dispensed in a double-blind fashion in identically appearing tablets, which contained 15, 25, 40, 50, 60, or 80 mg of atomoxetine or lactose for the placebo pills. Dose was based on the child's weight and was initiated at approximately 0.6 mg/kg per day for the first 7 days. The dose for the next 21 days was 1.2 mg/kg per day (mean dose = 1.11 mg/kg per day (standard deviation [SD] = 0.12 mg/kg per day); range = 0.85–1.33 mg/kg per day). Atomoxetine and placebo were administered once daily in the morning or twice daily when children were unable to tolerate a single dose. At each 28-day period, children returned their unused pills to assess compliance, which was determined as missing more than 2 consecutive days of full doses of medication or failing to take at least 80% of prescribed medication. One patient with ADHD + RD in the placebo period and 1 patient with RD in the atomoxetine period were noncompliant. One patient in the ADHD only group was noncompliant in both 28-day periods. Normal controls did not receive medication.
Screening measures
All participants were screened for the presence of ADHD combined subtype (ADHD-C) with the Disruptive Behavior Disorder Rating Scale (DBD) (Pelham et al. 1992; Oosterlaan et al. 2000). The parent version of the Diagnostic Interview Schedule for Children (PDISC-IV) was administered (Ferdinand et al. 1998; Shaffer et al. 2000). The PDISC-IV is based on the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association 1994) and the International Classification of Diseases, 10th revision (ICD-10). A diagnosis of ADHD-C was made if: (1) Parent and teacher scores on both the Inattention and Hyperactivity/Impulsivity scales on the DBD fell at least in the subclinical range (≥90th percentile) and (2) criteria for ADHD-C on the PDISC-IV were met.
All children were thoroughly screened for the presence of RD using two technical word reading tests, namely the One Minute Test (OMT) (Brus and Voeten 1973) and the Pseudo-word Reading Test (PRT) (Van den Bos et al. 1999), and one text reading test, the Text Reading Test (TRT) (Visser et al. 1998). A diagnosis of RD was made if children had at least 15 months delay on at least two of the three reading tests. Normal controls, who met the criteria for ADHD-C or any other subtype of ADHD or RD, were excluded.
Exclusion criteria for all groups
Children were excluded if they met criteria for obsessive compulsive disorder (OCD), tic disorder (including Tourette's disorder), depression, or conduct disorder as assessed by the PDISC-IV. In addition, children were excluded if they obtained a raw score of 40 or higher on the Children's Depression Rating Scale (CDRS) indicating major depression (Poznanski and Mokros 1996). Furthermore, exclusion criteria were a prior or current diagnosis of pervasive developmental disorder (PDD), anxiety disorder, posttraumatic stress disorder (PTSD), and neurological disorders, such as epilepsy as assessed by clinicians.
Children with severe arithmetic deficits were excluded as defined by a delay greater than 20 school months on the Speeded Arithmetic Test (SAT) (De Vos 1992), and a score below the 3rd percentile on the Cognitive Subscales for Arithmetic (CSA) (De Clerq et al. 2002).
Children were excluded if their estimated intelligence quotient (IQ) was below 80, using four subtests of the Wechsler Intelligence Scale for Children, 3rd edition (WISC-III): Picture Arrangement, Arithmetic, Block Design, and Vocabulary (Sattler 1992).
Measures
ADHD symptomatology (ADHD-Rating Scale IV)
The ADHD Rating Scale-IV (ADHD-RS-IV) (DuPaul et al. 1998) was used to measure change in ADHD symptoms in the ADHD and ADHD + RD groups during the two 28-day treatment periods, as rated by the investigator with the parent as rating source. The ADHD-RS-IV consists of 18 items, with one item for each of the 18 symptoms of ADHD as listed in the DSM-IV. Each item is scored on a 0–3 scale, which indicates the frequency of ADHD symptoms in the child over the past week. Higher scores indicate more severe symptoms.
Neuropsychological measures
Visuospatial Working Memory (Corsi Block Tapping task)
The Corsi Block Tapping task was administered to examine visuospatial working memory (Schellig 1997). Nine blocks were displayed on a computer touch screen. A small cursor on the screen tapped a sequence of blocks, starting with a two-block sequence that could be increased to nine blocks. After a tone, the child had to retap the demonstrated sequence by touching the screen. The test stopped when the child failed to complete two trials of a block sequence. For each block sequence, there were two trials, which could be extended with one trial when the first or second trial was incorrect. The dependent variable was the total number of correct trials, Number Correct Sequences.
Inhibition (Stop Signal Paradigm)
The Stop Signal Paradigm was administered to measure response inhibition (Oosterlaan et al 1998; Lijffijt et al. 2005). In the first block of the task, children had to indicate the position of a cartoon airplane on a computer screen by pressing one of two spatially compatible response buttons. In the next five blocks, a cross was imposed on the cartoon airplane in 25% of the trials, which indicated that the child had to inhibit his response. Using a tracking mechanism, a 50% chance of response inhibition was established by decreasing or increasing the delay between the onset of the cartoon airplane and the cross, depending on performance of the child (Logan and Cowan 1984). SSRT can be determined by subtracting the mean delay time between the onset of the cartoon airplane and the cross from the mean reaction time (MRT) on cartoon airplanes. Latency and accuracy of the response execution process were also registered by MRT and number of errors (omission and commission errors), respectively (Band et al. 2003).
Lexical Decision making (Lexical Decision task)
A lexical decision task was administered to measure lexical decision skills (Meyer and Schvaneveldt 1971). Participants had to discriminate Valid Words from Pseudowords, which were presented individually on a computer screen. The practice block of 25 words was followed by 5 blocks of each 25 Valid Words and 25 Pseudowords presented in a pseudo-randomized manner.
The dependent variable was d′, which measured the accuracy by which subjects correctly discriminated Valid Words from Pseudowords, independent of response bias (Macmillan and Creelman 1991). The hit rate and the false-positive rate of each child were normalized by a probit function because responses were binomial. In addition to d′, the MRT of correctly discriminated Valid Words and Pseudowords was noted. The MRT for Valid Words reflects the latency of lexical decision, because Valid Words are hypothesized to be stored in the mental orthographical lexicon (Manis et al. 1996). The MRT for Pseudowords indicates the latency of the decoding process, because Pseudowords are not stored in the mental lexicon. Pseudowords must be decoded, letter by letter or by letter cluster, to determine what is written (Manis et al. 1996).
Data analysis
Seven data points for the visuospatial working memory task, the Corsi Block Tapping task, were randomly missing due to technical errors and were replaced by regression analysis (Tabachnick and Fidell 2007). The lexical decision task was not administered to 1 child, because this child had not received sufficient reading instruction to complete this task. Results did not change after removing noncompliant children; thus, these children were retained in the analyses for power reasons. To reduce the influence of extreme values, such values were replaced by the next most extreme value in the distribution plus one unit (Tabachnick and Fidell 2007).
The data were analyzed by the groups who received treatment (ADHD, ADHD + RD, and RD). To test for order effects of treatment, the dependent measures were subjected to analyses of variance (ANOVAs) with treatment as within-subject factor (baseline, placebo, and atomoxetine) and as between-subject factors, treatment order (placebo–atomoxetine or atomoxetine–placebo), and group. When treatment order was not significant, the dependent variables were subjected to an ANOVA with treatment as a within-subject factor and group as a between-subject factor. When an overall significant treatment effect and/or a treatment by group interaction were found, repeated contrasts were performed to compare placebo with atomoxetine. When the placebo–atomoxetine repeated contrast led to a significant group by treatment interaction, paired sample t-tests were performed per group to study the origins of the interaction. For these paired sample t-tests, the study-wide alpha level was adjusted for multiple comparisons. Because the baseline-placebo comparison was not the objective of this study, results of this comparison were left out of the results text. The interested reader is referred to Table 1. Group effects were tested with Tukey post hoc tests.
Follow-up paired t-tests tested for the effects of placebo as compared to baseline within each of the groups. Indicated groups showed significant effects in the baseline-placebo comparison p < .05.
Significant at p < 0.01.
Significant at p < 0.05.
One child was missing.
Abbreviations: SSRT = stop signal reaction time; MRT = mean reaction time; ADHD = attention-deficit/hyperactivity disorder; RD = reading disorder.
If a significant treatment order effect occurred (treatment by treatment order interaction, or a treatment by treatment order by group interaction), only data for the first 28-day medication period were analyzed. An ANOVA was conducted with visit (baseline and visit after the first 28-day medication period) as within-subject factor and treatment (placebo or atomoxetine) and group as between-subject factors. Order effects were limited to MRT Valid Words in the lexical decision task. The two orders (atomoxetine–placebo or placebo–atomoxetine) did not lead to differences with respect to baseline ADHD severity, reading, age, IQ, inhibition, visuospatial working memory, and lexical decision.
When the placebo–atomoxetine comparison was significant, the treatment groups were compared to normal controls to test whether normalization occurred. Scores for the medication groups on placebo and atomoxetine were compared to the scores of the second visit of normal controls to account for possible retest effects with univariate ANOVAs. Tukey post hoc tests were used to test the group differences further. Alpha was set at p < 0.05 for all comparisons except the paired sample t-tests.
Results
Group characteristics and results for the neuropsychological measures are provided in Table 2.
p < 0.05.
Scores for the second visit of the normal control group.
Abbreviations: ADHD = Attention-deficit/hyperactivity disorder; ADHD-RS-IV = Attention-Deficit/Hyperactivity Disorder Rating Scale IV; IQ = intelligence quotient; M = mean; MRT = mean reaction time; NC = normal controls; N.S. = not significant; RD = reading disorder; SD = standard deviation; SSRT = stop signal reaction time.
ADHD symptomatology (ADHD-RS-IV)
A significant treatment effect was found on ADHD symptoms as assessed by the ADHD-RS-IV (F[2,68] = 10.26, p < 0.001, ηp 2 = 0.23). A repeated contrast revealed that ADHD symptoms diminished, after taking atomoxetine compared to placebo (F[1,34] = 6.91, p < 0.013, ηp 2 = 0.16). Treatment effects for atomoxetine were comparable for children with ADHD and ADHD + RD, because no significant group by treatment interaction occurred in the placebo–atomoxetine comparison. No significant effect of group was found indicating that there was no significant difference in ADHD symptoms between the ADHD + RD and ADHD-only groups.
Neuropsychological measures
Visuospatial Working Memory (Corsi Block Tapping task)
Treatment significantly improved visuospatial working memory (F[2,108] = 20.52, p < 0.001, ηp 2 = 0.27). A repeated contrast showed that a larger Number Correct Sequences was completed with atomoxetine compared to placebo (F[1, 54] = 8.21, p = 0.006, ηp 2 = 0.13). Groups differed in visuospatial working memory (F[2,54] = 4.18, p = 0.02, ηp 2 = 0.13). Tukey post hoc tests revealed that the ADHD group had a lower Number Correct Sequences than either the RD or ADHD + RD groups (p = 0.02 and p = 0.05, respectively). No significant differences occurred between the ADHD + RD and RD groups (p > 0.10).
A significant treatment by group interaction was observed for visuospatial working memory (F(4,108) = 2.56, p = 0.042, ηp 2 = 0.08). A repeated contrast indicated differential group effects after taking atomoxetine compared to placebo (F[2,54] = 5.35, p = 0.008, ηp 2 = 0.16). Figure 2 shows that only children with ADHD + RD had a larger Number Correct Sequences following atomoxetine compared to placebo, which was confirmed by a significant paired sample t-test (p < 0.01). Paired sample t-tests for the other two groups were not significant, all p values > 0.10.
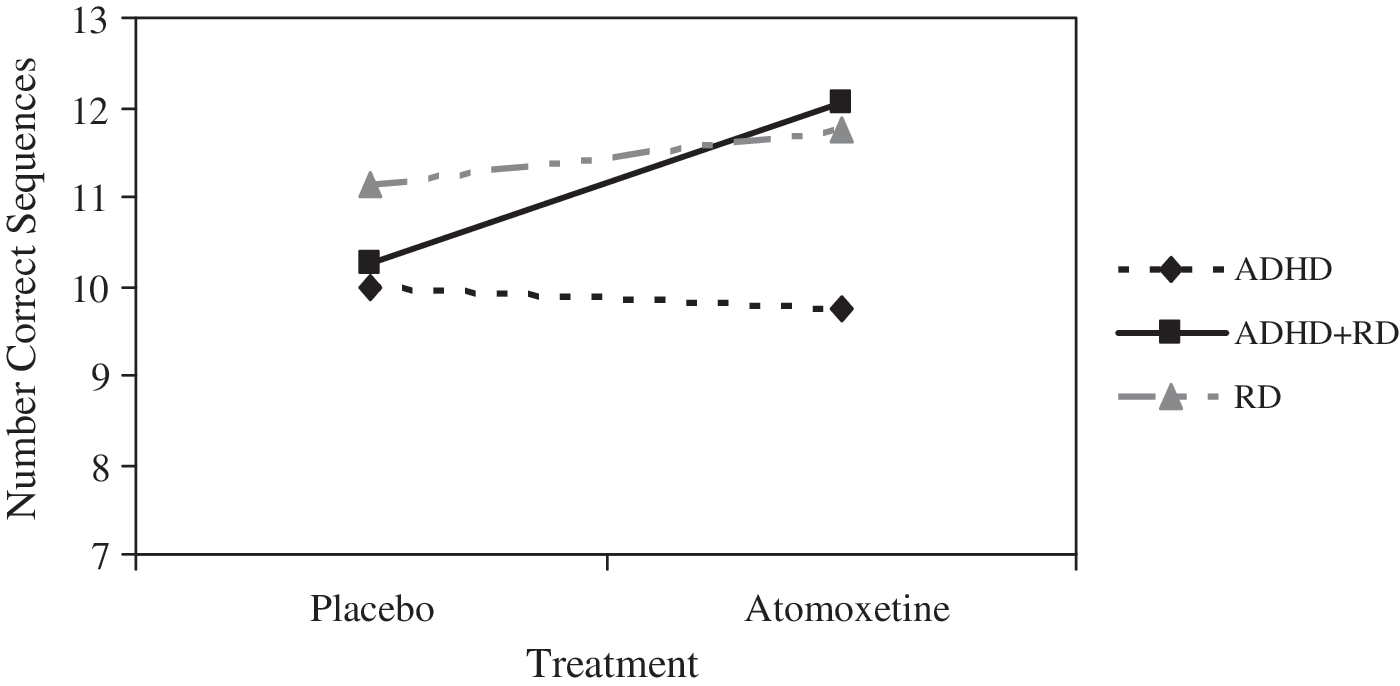
Number Correct Sequences per group and treatment. Number Correct Sequences improved only in the ADHD + RD group after taking atomoxetine in comparison to placebo. ADHD = Attention-deficit/hyperactivity disorder; RD = reading disorder.
Visuospatial working memory was poorer in children with ADHD compared to both the ADHD + RD and RD groups. Atomoxetine improved visuospatial working memory only in the ADHD + RD group.
Inhibition (Stop Signal Paradigm)
Inhibitory control (SSRT) was not affected by treatment nor were there significant group differences in inhibitory control. A significant treatment by group interaction was observed (F[4,108] = 2.48, p = 0.048, ηp 2 = 0.08). The contrast comparing atomoxetine to placebo marginally interacted with group (F[2,54] = 2.66, p = 0.07, ηp 2 = 0.09). Figure 3 shows that only children with ADHD + RD had faster SSRTs following atomoxetine compared to placebo, which was supported by a nearly significant paired sample t-test, p = 0.07. The paired sample t-test comparing SSRTs of the ADHD + RD and RD groups on placebo and atomoxetine were not significant (p > 0.10).
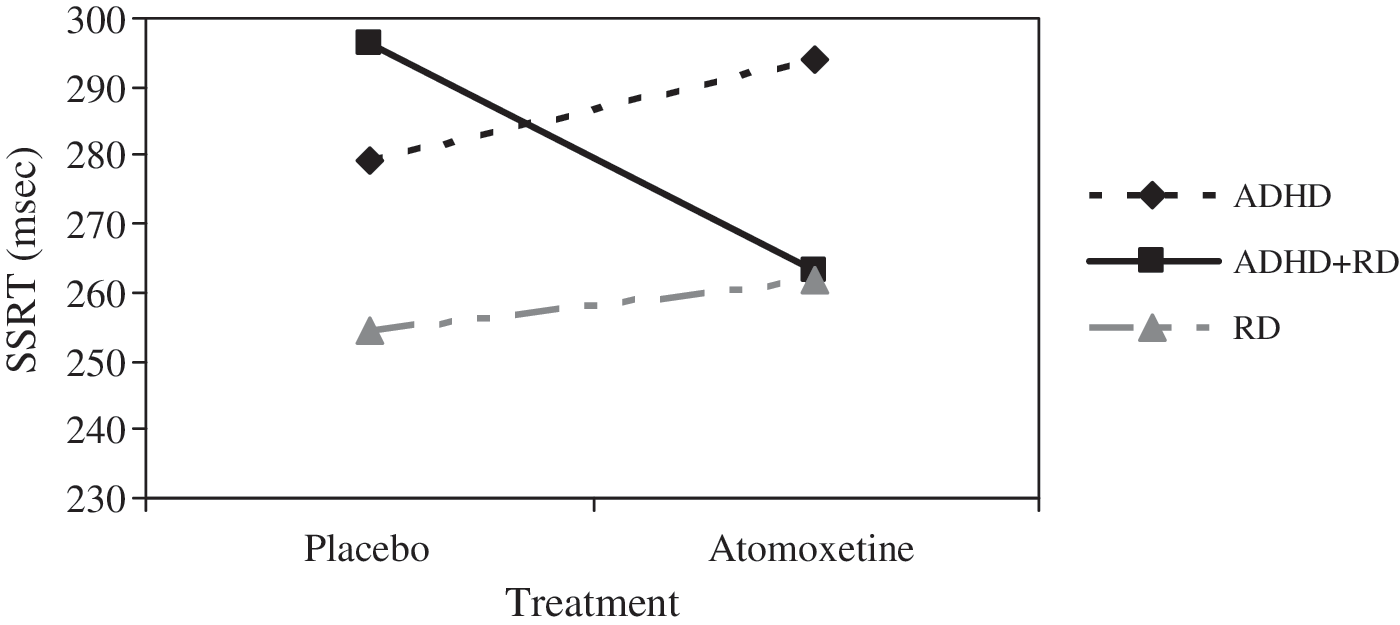
Mean SSRT per group and treatment. SSRT became faster only in children with ADHD + RD after taking atomoxetine in comparison to placebo. SSRT = stop signal reaction time; ADHD = attention-deficit/hyperactivity disorder; RD = reading disorder.
Speed of processing was significantly influenced by treatment (F[2,108] = 16.74, p < 0.001, ηp 2 = 0.23). The effects of treatment were due to a significant baseline-placebo comparison (see Table 1). Groups differed in MRT (F[2,54] = 3.93, p = 0.02, ηp 2 = 0.12). Children with RD had slower MRTs than children with ADHD (p = 0.02). MRTs of children with ADHD + RD fell between the MRTs of the RD group and ADHD group, but did not significantly differ from these two groups (p > 0.10). No significant group-by-treatment interaction was observed.
Accuracy was affected by treatment (F[2,108] = 6.39, p = 0.002, ηp 2 = 0.10), which was due to a significant baseline–placebo comparison (see Table 1). The group effect escaped conventional levels of significance (F[2, 54] = 3.05, p = 0.055, ηp 2 = 0.10). Tukey post hoc tests showed that children with RD made fewer errors than children with ADHD + RD (p = 0.006). The ADHD group did not significantly differ from the RD and ADHD + RD groups (all p values > 0.10). No significant group-by-treatment interaction was observed.
Some evidence for beneficial effects of atomoxetine on inhibition as assessed by SSRT was found in the ADHD + RD group, whereas atomoxetine did not impact the ADHD or RD groups in this test.
Lexical Decision (Lexical Decision task)
Lexical decision accuracy, as assessed by d′, was not significantly influenced by treatment. The group effect was marginally significant (F[2,53] = 2.85, p = 0.066, ηp 2 = 0.09). Children with ADHD + RD had lower d′ values than children with ADHD, although this group difference fell shy of significance (p = 0.057). No other significant group differences or group-by-treatment interactions were found.
MRT Pseudowords showed a significant treatment effect (F[2,106] = 3.14, p = 0.04, ηp 2 0 = 0.05). However, no significant differences were found between either the baseline and placebo or placebo and atomoxetine comparisons. No significant group differences were observed for MRT Pseudowords nor a group-by-treatment interaction occurred.
MRT Valid Words was affected by treatment order (F[2,49] = 4.18, p = 0.02, ηp 2 = 0.14). Therefore, only data for the baseline and the visit after the first 28-day medication period were analyzed. No significant effects were observed for treatment or group.
To summarize, accuracy and speed of lexical decision and decoding were not influenced by atomoxetine.
Normalization
To test whether performance normalized for variables that showed an effect of atomoxetine, performance on placebo and atomoxetine of the treatment groups was compared to the performance of normal controls on their second visit. On placebo, groups differed on visuospatial working memory (Number Correct Sequences) (F[3,79] = 3.15, p = 0.02, ηp 2 = 0.10). Tukey post hoc tests showed that both the ADHD and the ADHD + RD groups had poorer visuospatial working memory than normal controls (p = 0.048 and p = 0.071, respectively). The RD group did not differ from either group (all p values, p > 0.10). There was a group effect following atomoxetine on visuospatial working memory (F[3,79] = 4.51, p = 0.006, ηp 2 = 0.14). Only the ADHD group remained different from normal controls (p = 0.007) when treated with atomoxetine (p values for other groups, p > 0.10).
On placebo, groups marginally differed on SSRT (F[3,79] =2.36, p = 0.07, ηp 2 = 0.08). Tukey post hoc tests revealed that SSRTs of the ADHD + RD group were marginally slower compared to normal controls (p = 0.08), all other group differences were not significant (p > 0.10). After taking atomoxetine, no significant group differences were observed for SSRT (F[3,79] = 1.55, p = 0.20, ηp 2 = 0.05).
Discussion
The first goal of this study was to examine the effects of atomoxetine on visuospatial working memory and inhibition in children with ADHD, ADHD + RD, or RD. Visuospatial working memory improved after taking atomoxetine in children with ADHD + RD compared to placebo. Atomoxetine showed, compared to placebo, a marginally significant positive effect on inhibition in the ADHD + RD group. Both the ADHD and RD groups showed no improved neuropsychological functioning following atomoxetine. The second goal of this study was to determine possible effects of atomoxetine on lexical decision; no beneficial effects were found. Atomoxetine had the expected beneficial effects on ADHD symptomatology compared to placebo.
Atomoxetine affected executive functioning only in children with ADHD + RD, which suggests that ADHD and ADHD + RD are not only different subtypes of ADHD at a neuropsychological level (Purvis and Tannock 2000), but possibly also at the neurochemical level (Halperin et al. 1997). Previous research suggests a difference in noradrenaline levels between children with ADHD and children with ADHD + RD. Children with ADHD + RD had higher plasma levels of the noradrenaline metabolite 3-methoxy-4-hydroxyphenylglycol (MHPG) than children with ADHD. MPHG appeared to be inversely associated with academic achievement and verbal processing, but was not related to behavior ratings or measures of attention and impulsivity (Halperin et al. 1997).
As expected, atomoxetine improved the maintenance function of visuospatial working memory. Although the exact mechanism is unclear, working memory may be mediated by modulation of the noradrenaline α2 receptor and the dopamine D1 receptor in the prefrontal cortex (Arnsten and Li 2005). Atomoxetine increases both noradrenaline and dopamine in the prefrontal cortex (Bymaster et al. 2005), which may possibly be related to the improved visuospatial working memory performance. It is unclear whether verbal and visuospatial working memory tap the prefrontal cortex to the same extent, despite evidence that verbal working memory is more left oriented and visuospatial working memory is more right oriented in the brain (Smith and Jonides 1998). We did not include a measure of verbal working memory, hence it was not possible to conclude whether atomoxetine improves working memory in general or only visuospatial working memory.
Lexical decision appeared insensitive to atomoxetine. Previous research indicated that visuospatial working memory was associated with reading ability (Savage et al. 2007). However, the results of this study show no evidence of improvements in visuospatial working memory leading to equivalent benefit in reading as assessed by lexical decision.
The results should be interpreted in light of several limitations. Mean dose (1.11 kg/day) was relatively low compared to other studies with atomoxetine. Generally, other studies have used a higher mean end dose because these studies were longer in duration and titrated to 1.8 mg/kg, when 1.2 mg/kg was not effective after 4 weeks (Kratochvil et al. 2004; Crommen and Dankaerts 2005). However, no relation was demonstrated between weight-adjusted dose and our dependent variables. There was a relation between absolute dose and score on ADHD-RS (r = −0.52, p = 0.001) and the speed measures (MRT, r = −0.30, p = 0.01, MRT Valid Words, r = −0.29, p = 0.02 and MRT Pseudowords, r = −0.27, p = 0.041). Children with higher absolute doses were heavier and thus generally older: However, a recent meta-analysis indicated no relation between age and efficacy of atomoxetine (Cheng et al. 2007). Future research with higher absolute dose in larger groups might reveal atomoxetine effects in children with ADHD and children with RD in neuropsychological performance.
The results may be confounded by age and IQ, because the groups differed in age and IQ. We have chosen not to covary for age and IQ because age and IQ are related to the groups (Miller and Chapman 2001). A lower IQ is consistently found in children with ADHD (Frazier et al. 2004). Thus, covarying for IQ may remove crucial variance. Differences in age are more or less inherent to the disorders. To diagnose RD, a child must have followed 2–3 years of reading education; in our sample, children with ADHD + RD and RD were older than children with ADHD. Thus, age was related to groups in a nonrandom fashion, which makes covarying for age inappropriate.
Unfortunately, disproportionately more children had atomoxetine than placebo in the first period (n = 34 and n = 23, respectively). To test whether order influenced the results, we reran the analyses with treatment order as covariate, which did not alter the results. Thus, the findings on atomoxetine are not confounded by placebo or learning effects in the first period.
In summary, this is the first study to demonstrate beneficial effects of atomoxetine on visuospatial working memory and to a lesser extent inhibition in children with ADHD + RD. Atomoxetine did not affect lexical decision and EF in children with ADHD and children with RD. The present findings suggest there may be separate developmental pathways for co-morbid ADHD + RD and ADHD or RD alone.
Footnotes
Disclosures
Dr. Sergeant has been member of the advisory boards of Eli Lilly, Shire, and Janssen Cilag. Dr. Oosterlaan is a member of the advisory boards of Shire and UCB. Dr. Temmink is a member of the advisory board of Janssen-Cilag. Drs. Pereira and Vlasveld are members of the advisory boards of Janssen-Cilag, Eli Lilly, UCB, Eurocept, and Shire. The remaining authors have no financial ties or conflicts of interest to report.