
Abstract
Objective and background:
Early repolarization (ER), considered a common and benign electrocardiographic pattern on the surface 12-lead electrocardiogram (ECG), was recently found to be prevalent among patients with idiopathic ventricular fibrillation. It is also highly predominant in physically active young males. Reports on sudden cardiac death (SCD) of children and adolescents treated with psychotropic agents have raised concerns regarding the need for cardiovascular monitoring and risk stratification schedules. The rate of ER pattern has not been estimated in children with attention deficit/hyperactivity disorder (ADHD). Thus, in the present retrospective chart review study, we estimated the rate of ER pattern, as well as RR, QT, and QTc intervals, from ECG tracings of physically healthy children with ADHD versus physically and mentally healthy controls.
Methods:
The ECG tracings of 50 children (aged 8.7 ± 1.4 years; 12 girls, 44 boys) diagnosed as suffering from ADHD were compared to 55 physically and mentally healthy controls (aged 8.25 ± 2.1 years; 20 girls, 35 boys). ER was defined as an elevation of the QRS–ST junction (J point) of at least 0.1 mV from baseline with slurring or notching of the QRS complex, and assessed separately by two senior cardiologists who were blind to all other data relating to the study participants.
Results:
The rate of ER pattern was significantly higher in ADHD children compared to normal controls (32% vs. 13%, respectively, P = 0.012; relative risk [RR] = 1.68, 95% confidence interval [CI] 1.16–2.44), irrespective of stimulant treatment or gender. All other standard ECG measures (heart rate, QT and QTc intervals) were within normal range.
Conclusion:
The rate of ER in children with ADHD is significantly higher than in normal controls. Its clinical significance awaits further research.
Introduction
A recent scientific statement from the American Heart Association focused on children and adolescents with heart disease receiving medications for ADHD (Vetter 2008). It suggested avoiding their use in children with serious heart diseases. Moreover, it recommended that a careful evaluation should be instigated before commencing stimulant agents for children and adolescents with ADHD. This should culminate in assessing the correlation between clinical signs and symptoms, physical examination, relevant family and personal history, and an electrocardiogram (ECG) recording. It was emphasized that there are no widely accepted guidelines and recommendations for cardiac monitoring of ADHD patients treated with stimulant agents, and more research is warranted to assess the risk of SCD in children and adolescents, with or without heart disease, maintained on stimulant agents. Most preclinical and clinical research focused on the issue of QTc interval prolongation, as a risk factor for increased vulnerability for serious arrhythmias and SCD (Blair et al. 2004; McNally et al. 2006).
Drug-induced QT prolongation predisposes the patient to the development of torsades de pointes (TdP), ventricular tachycardia, and increased risk for SCD (Redfern et al. 2003). The association between a specific drug and development of TdP is, therefore, difficult to document. QT prolongation is considered a surrogate marker of the proarrhythmia risk. The molecular and cellular mechanisms related to drug-induced QT prolongation and TdP include putative alterations in the delayed rectifier potassium current (IKr) or trafficking of proteins forming this channel (Testai et al. 2004). Proarrhythmia caused by a QT-prolonging drug occurs infrequently, and usually multiple factors need to operate in concert to precipitate such an event, including a combination of two or more drugs affecting cardiac conduction, electrolyte balance, and possibly genetic predisposition. The ECG provides a unique opportunity to assess the safety of administered therapy. QTc interval measurement is the most routine approach in the evaluation of cardiac drug safety monitoring, although there are many challenges related to the methodology of determining QTc interval (Glassman and Bigger 2001).
Some studies of children treated with stimulants have reported a persistent modest increase in blood pressure and heart rate (Nissen 2006). No consistent ECG changes were reported, although some studies reported statistically significant QT interval prolongation (Findling et al. 2005; Donner et al. 2007). Because the QT interval is a measure of the period of both depolarization and repolarization of the ventricles, understanding the distribution of cardiac parameters in children should also focus on the characteristics of ST–T wave complex, which may shed light on repolarization heterogeneity and cardiovascular risk. In an attempt to ascertain changes in ECG parameters while on anti-ADHD agents, it is important to characterize the ECG pattern while off medication, because psychopathology could also influence cardiac parameters via changes in the autonomic modulation (van Lang et al. 2007). To the best of our knowledge, there are no data about the characteristics of cardiac ventricular repolarization in naïve children with ADHD.
Early repolarization (ER), consisting of an elevation of the QRS–ST junction (J point), QRS notching or slurring (J wave), and a tall, symmetric T wave, is a common electrocardiographic finding, which is generally considered to be benign (Wasserburger and Alt 1961). These ECG features are found in approximately 2–5% of the general population, with young male predominance, indicating a possible role to sex hormones (James et al. 2007). Their clinical significance has been confined largely to the differential diagnosis from life-threatening clinical conditions, like acute pericarditis, acute myocardial infarction, and the Brugada syndrome (Riera et al. 2008). Isolated case reports, mostly from Asia, have documented such changes in the QRS–ST junction in men with idiopathic ventricular fibrillation (Kalla et al. 2000; Takagi et al. 2000; Letsas et al. 2007). Recently, Haïssaguerre et al. (2008) reported that the prevalence of ER is much higher among patients with a history of idiopathic ventricular fibrillation compared to normal controls (31% vs. 5%, respectively). Their 5-year study, involving 22 tertiary care arrhythmia centers, was the first clinical evidence linking a commonly benign ECG pattern with observed increased arrhythmogenicity.
With these caveats in mind, our preliminary retrospective study was designed to estimate, for the first time, the rate of ER pattern in a cohort of children (age <12 years) diagnosed as suffering from ADHD, compared to normal controls.
Methods
Study population
The study population was recruited from the computerized database of the Procardia Cardiac and Rehabilitation Center of the Maccabi Health Services in Tel Aviv, Israel. ECG tracings were mandatory in ADHD children prior to commencing stimulant treatment and during maintenance. The ECG tracings in the control group were performed as part of a routine workup of children with nonspecific complains.
Initially, the study included the ECG tracings of 159 children. Thirty eight were excluded due to history, signs, or symptoms of cardiovascular disorders (2, Wolf–Parkinson–Wight syndrome; 2, ventricular septal defect; 1, congenital aortic stenosis; and 1, short QT interval [QTc <300 msec]), neurological disorders (1, epilepsy), psychiatric or developmental disorders other than ADHD (1, tic disorder and panic disorder; 1, mental retardation; 2, developmental disorder; 6, precocious puberty), and sinus tachycardia (n = 22). Eventually, 121 children were found eligible; 56 of them were diagnosed with ADHD (aged 8.7 ± 1.4 years; 12 girls, 44 boys), and 65 were to serve as physically and mentally healthy controls (aged 7.8 ± 2.1 years; 20 girls, 45 boys). All participants attended the regular education system. None of the children was medicated with vasoactive agents, except for 18 children in the ADHD group who were maintained on methylphenidate treatment. None of the participants reported substance use.
Due to the retrospective chart review nature of the study, no informed consent was required and the study was approved by the Institutional Helsinki committee.
ECG recordings and analysis
The ECGs were recorded at a paper speed of 25 mm/second and at standard amplification (1 mV = 10 mm). All ECGs were magnified with a 3 × optical magnifier, and all measurements were performed manually with a caliber of 10 msec (10 msec = 0.25 mm) accuracy. RR intervals and QT intervals were measured and expressed as their absolute values in milliseconds. QTc, which is the rate-corrected QT interval, was also calculated, using Bazett's formula (1920).
ER was defined as an elevation of the QRS–ST junction (J point) in at least two leads, with J-point amplitude elevation of at least 1 mm (0.1 mV) above the baseline. The J-point should then continue with QRS slurring (a smooth transition from the QRS segment to the ST segment) or QRS notching (a positive J deflection inscribed on the S wave). Contrary to Haïssaguerre et al. (2008), we also included ER signs in the anterior leads (V1–V3).
The ECG tracings were assessed independently by two senior cardiologists with special expertise in cardiac electrophysiology (S.S. and B.S.), who were blind to the children's other data. If the two cardiologists did not reach agreement as to the presence of ER, the corresponding ECG was excluded from further analysis.
Statistical analysis
All variables are presented as mean ± standard deviation (SD). Comparison between the two groups was performed using the two-tailed Student t-test for unpaired data. Categorical variables were compared with the two-tailed Fisher exact test. Statistical significance was set at p < 0.05.
Results
The ADHD group consisted initially of 56 children (aged 8.7 ± 1.4 years; 12 girls, 44 boys). Six children were excluded from the study due to lack of consensus between the two cardiologists. Thus, we were left with a group of 50 ADHD children (aged 8.7 ± 1.4 years; 11 girls, 39 boys; 32%) of whom 16 (2 girls, 14 boys) with ER as well. Figure 1 illustrates a representative ER pattern. The control group initially consisted of 65 children (aged 8.3 ± 2.0 years; 20 girls, 45 boys). Ten children from the control group were excluded from the study, leaving 55 healthy controls (aged 8.25 ± 2.1 years, 20 girls, 35 boys; 13%) and among them 7 children with ER (1 girl, 6 boys). A two-tailed Fisher exact test showed a significant difference in the rate of ER between ADHD and healthy controls (p = 0.012; relative risk [RR] = 1.68, 95% confidence interval [CI] 1.16–2.44). The power of our test was 65.2% for α = 0.05.
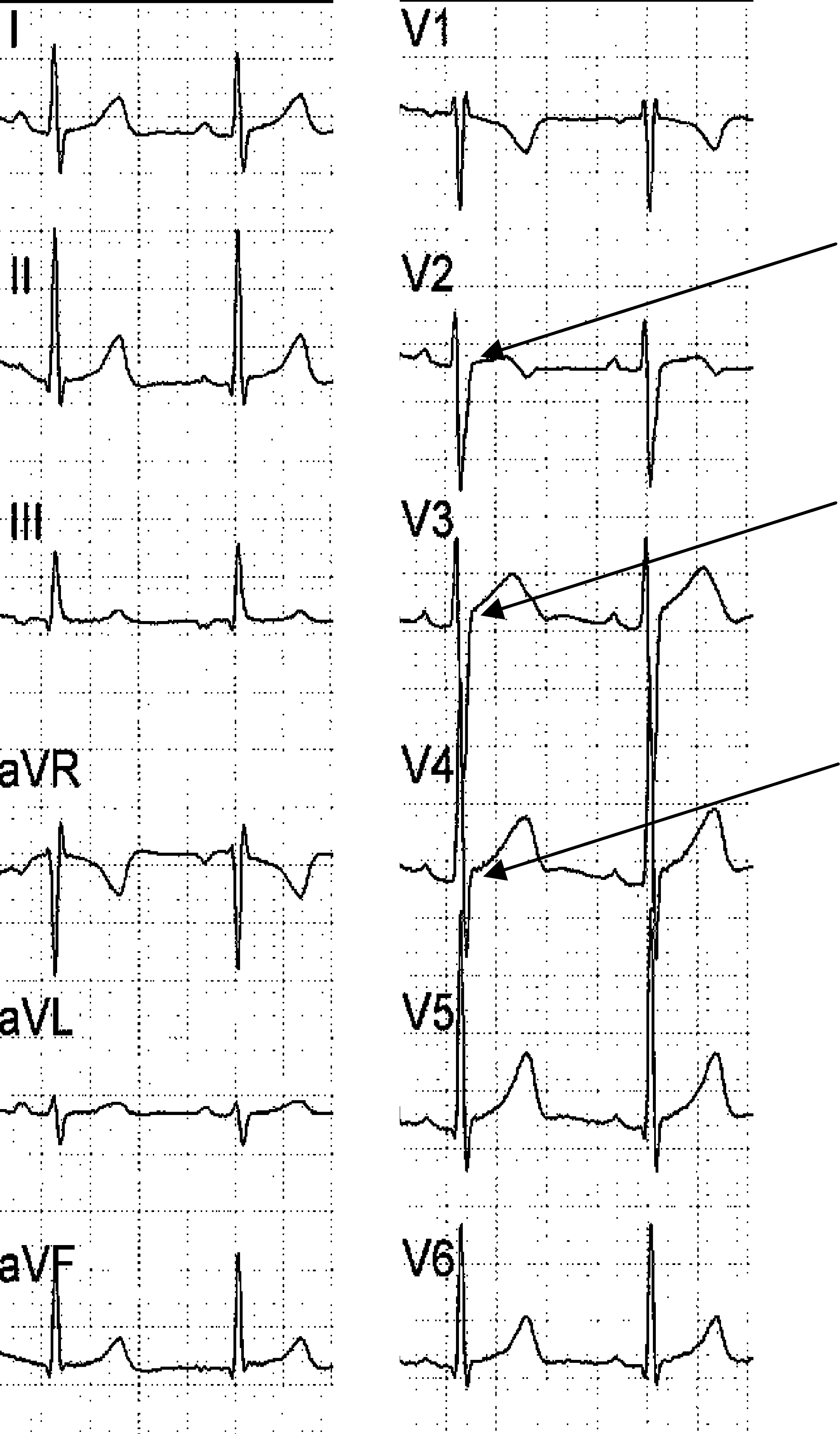
A 12-lead surface ECG of a 7-year old boy with ADHD. Early repolarization pattern is evident in leads V2, V3, V4, as indicated by the arrows.
As shown in Table 1, a similar rate of stimulant use was observed in the ADHD group both in children with and those without ER (6/16 [37%] vs. 13/34 [38%], respectively; Fisher exact test: p = 1.0, not significant [N.S.]). Within this group, no significant difference was found with regard to gender distribution in either of the subgroups: 14 males out of 16 children with ER (87.5%) vs. 25 males out of 34 children without ER (73.5%) (Fisher exact test: p = 0.47, N.S.). No significant differences were obtained between ADHD children maintained on stimulants and the untreated ADHD children with regard to RRI, QT, and QTc intervals (two-tailed Student t-test, p = 0.07–0.59, for all). The rate of ER pattern was similar in treated and untreated ADHD children (6/13 versus 10/21, respectively; Fisher exact test, p = 1.0, N.S.) (Table 1).
No statistical differences were noted between the treated and untreated ADHD children with respect to all parameters (p = 0.07–0.59, for all).
Two-tailed Fisher exact test.
Most of the controls (30/55) were subjects that were referred for ECG due to nonspecific cardiac symptoms (e.g., palpitations, chest pain).
Abbreivations: SD = Standard deviation; ADHD = attention-deficit/hyperactivity disorder; RRI = RR interval; QTc = QT corrected; ER = early repolarization.
Basic demographics and the ECG measures are summarized in Table 1. RR intervals and QT and QTc intervals were within the normal range, and no significant difference was found between the ADHD and control groups with regard to this measure.
Discussion
The aim of the present retrospective/naturalistic chart-review study was to evaluate the occurrence of ER in a group of ADHD children versus normal controls. The major finding of our study was that the presence of the ER pattern was significantly higher in the ADHD children compared to the healthy controls (32% vs. 13%, respectively), and that it was irrespective of stimulant treatment or gender. All other standard ECG measures were within normal range and were not significantly different from those reported in a recent large-scale study of children and adolescents with ADHD (Prasad et al. 2007).
While, to the best of our knowledge, our study is the first attempt to assess the rate of ER in children with ADHD, several limitations are worth mentioning. The small sample size of the ADHD group (n = 50) is a significant limitation; larger samples are necessary. Also, some of the ADHD children (19/50) were maintained on stimulants, and 3 of them were maintained on stimulants combined with another medication (2 with low-dose risperidone and 1 with low-dose olanzapine), due to the naturalistic nature of the study. In our study, similar rates of ER were noted both in the ADHD children maintained on stimulants and those not maintained on stimulants. Still, an interaction between ADHD, stimulant maintenance, and occurrence of ER cannot be discounted. Finally, the cross-sectional study design merits longitudinal follow-up studies (before and after treatment with anti-ADHD medications) to shed light on the abundance of ER, its progression course over time, and clinical significance. We attempted to control for organic causes that might influence the ECG measures by including only physically healthy children in both groups. Issues such as substance abuse were not relevant in the context of our young pediatric sample. The ECG recordings were done during the morning hours, to obviate possible diurnal influences on the ECG tracings. The lack of prospective controls and standardization involved in a chart review study should also be noted. In addition, there was a selection bias in the controls, who were referred for ECG evaluation due to nonspecific cardiac symptoms, or routine check up before medical procedures. In contrast, the ADHD children were referred for ECG as a routine policy before and during stimulant treatment. However, it seems that this bias did not affect significantly the results, because there was a higher rate of ER pattern in the ECG tracings of the ADHD subjects (nonselected group) than in the controls (the selected group) (Table 1).
Clinical and experimental studies point toward high vagal tone and markedly reduced sympathetic tone in ER, which is more commonly seen in young individuals, and shows a clear male preponderance (77%) (Mehta and Jain 1999). Psychopathology may also influence cardiac parameters via changes in the autonomic nervous system balance. A recent study has shown that ADHD children have low heart rate reactivity immediately after stress, suggesting higher vagal than sympathetic activation (van Lang et al. 2007). Thus, one might speculate about a possible association between male gender, young age, and autonomic imbalance in the emergence of ER in ADHD.
In conclusion, a high rate of ER pattern (32% versus 13% in controls) was observed in a nonselected sample of ADHD children. The relevance of ER to cardiac risk assessment in ADHD population awaits further evaluation in larger samples of treated and untreated ADHD children and adults, as well as in other ADHD-associated neurodevelopmental disorders. At present, it seems justified to screen ECG tracings of ADHD children before initiation of stimulant treatment as well as during the follow-up period, especially during dose escalation.
Footnotes
Disclosures
Drs. Nahshoni, Sclarovsky, Spitzer, Zalslman, Strasberg, and Weizman have no conflicts of interest or financial ties to disclose.