
Abstract
Objective:
Exposure to psychotropic medications before the onset of bipolar disorder (BD) in children may have profound effects on the course of illness. Both antidepressant and stimulant exposure have been proposed to hasten the course of BD development, whereas mood stabilizers have been proposed as protective. We sought to describe psychotropic medication exposure in a cohort of children at risk for BD and retrospectively determine the effect of medication exposure on age at onset (AAO) of BD.
Methods:
Subjects were 106 children and adolescents who had at least 1 parent with BD. Of these, 63 had BD I or BD II and 43 had subsyndromal symptoms of BD. AAO was determined as nearest month of first manic or hypomanic episode. Past psychotropic medication exposure prior to AAO was determined through interview and chart review.
Results:
Both groups had high rates of exposure to psychotropic medications. Antidepressant or stimulant exposure was not correlated with an earlier AAO of BD. However, mood stabilizer exposure was associated with a later AAO.
Conclusions:
Children with full or subsyndromal BD are frequently exposed to a variety of psychotropic medications before their first manic episode. Our findings do not support that early stimulant or antidepressant exposure leads to an earlier AAO of BD. However, early mood stabilizer exposure may be associated with delayed AAO. Longitudinal studies are needed to clarify these results.
Introduction
Controlled data in children with BD are lacking, but retrospective reports suggest that children with BD may be even more susceptible than adults to SSRI-induced mania (Biederman et al. 2000; Cicero et al. 2003; Faedda et al. 2004). More disturbing is the possibility that children with BD may have had SSRI exposure before their first manic episode, which may have led to or hastened the development of mania. This phenomenon has been reported (Guile 1996; Go et al. 1998); however, due to the difficult nature of prospectively studying such events, we are lacking clear data on who is at highest risk for this manic conversion. Nevertheless, an analysis of a health maintenance organization (HMO) database of over 80,000 patients 5–29 years old found children 10–14 years old to be at the highest risk for switching from a diagnosis of major depressive disorder (MDD) to BD after being prescribed an SSRI (Martin et al. 2004). This finding would suggest that children, perhaps during menarche/adrenarche, are at greatest risk for SSRI-induced manias. However, there have been no prospective studies of high-risk populations examining age at onset (AAO) of BD that control for exposure to psychotropic medications such as stimulants and antidepressants (Carlson et al. 2000a).
Stimulants also have been proposed to possess the propensity for causing or exacerbating mania in children (Koehler-Troy et al. 1986; Vitiello 2001; Scheffer et al. 2005). Whether these agents can hasten the development of BD in a patient who has not yet had a manic episode is again unclear. It has been argued that early stimulant exposure in certain subsets of children with attention-deficit/hyperactivity disorder (ADHD) may lead to an earlier AAO of BD compared to children who were not exposed to stimulants and who still later developed BD (DelBello et al. 2001b; Reichart and Nolen 2004). Furthermore, children with BD and a premanic exposure to stimulants may have a more severe course of BD than those who were not exposed (Soutullo et al. 2002). Yet other researchers have suggested that stimulant exposure in youth with ADHD and mood symptoms does not necessarily lead to high rates of bipolar development (Carlson et al. 2000a; Galanter et al. 2003). Again, rigorous retrospective or prospective studies of stimulant exposure effects on AAO would be helpful in this debate.
Alternately, it has been proposed that mood stabilizers could delay or prevent the onset of BD if used before the onset of the first manic episode (Chang et al. 2003b). The utility of these medications in preventing bipolar relapse and their neuroprotective potential (Manji et al. 2000) argues for the likelihood of this effect. We earlier reported that open divalproex was effective in treating acute mood symptoms of children with subsyndromal BD (Chang et al. 2003b). However, it is not clear whether this intervention could delay or prevent the onset of BD in these high-risk children, because a maintenance study of divalproex in such children was negative (Findling et al. 2007).
Due to the high heritability of BD, offspring of parents with BD (“bipolar offspring”) are clearly at increased risk for BD themselves (Chang et al. 2003a). Cross-sectional studies of bipolar offspring have reported 14–50% to have bipolar spectrum disorders, with 5–14% having BD I or BD II (Chang and Steiner 2003). Furthermore, bipolar offspring also have high rates of ADHD, depression, and anxiety (DelBello and Geller 2001). Many of these children, especially those who already have ADHD with mood symptoms and/or MDD, are likely experiencing a prodrome to full BD (Chang et al. 2006). Thus, these children may possess an underlying neurobiology similar to children with fully developed BD and therefore share a similar vulnerability to SSRI- or stimulant-induced mania. Yet, because they present with ADHD or depression, it is possible that they are being treated with these potentially deleterious agents. These offspring represent an important population to study for potential AAO effects, negative or positive, of early psychotropic medication exposure.
Therefore, we wished to examine the effects of psychotropic medication on the development of BD in children and adolescents. Although a prospective study would be a more powerful design, in this initial study we first sought to collect retrospective data regarding overall medication exposure in a cohort of bipolar offspring with either subsyndromal or fully developed BD. We also retrospectively assessed AAO of the first manic episode for those offspring already with BD. We hypothesized that offspring with BD would have had greater rates of past exposure to stimulants and antidepressants than those offspring with only subsyndromal BD, and that such medication exposure would be associated with an earlier AAO. Conversely, we hypothesized that those offspring with BD who had previous exposure to mood stabilizers would have a later AAO than those without such exposure.
Methods
This study was approved by the Stanford University Panel on Human Subjects in Medical Research. We collected medication histories from 106 children with at least one parent with BD I or BD II. These children were recruited as part of an ongoing larger longitudinal study of bipolar offspring (Chang et al. 2000). Signed written consent was obtained from parents or guardians and written assent was obtained from subjects. Subjects were recruited from parents who were patients at the Stanford University Bipolar Disorders Clinic, from local support groups for bipolar adults, and from the surrounding community. The sample used in this study was recruited selectively for having either suspected BD or early forms of BD (Fig. 1).
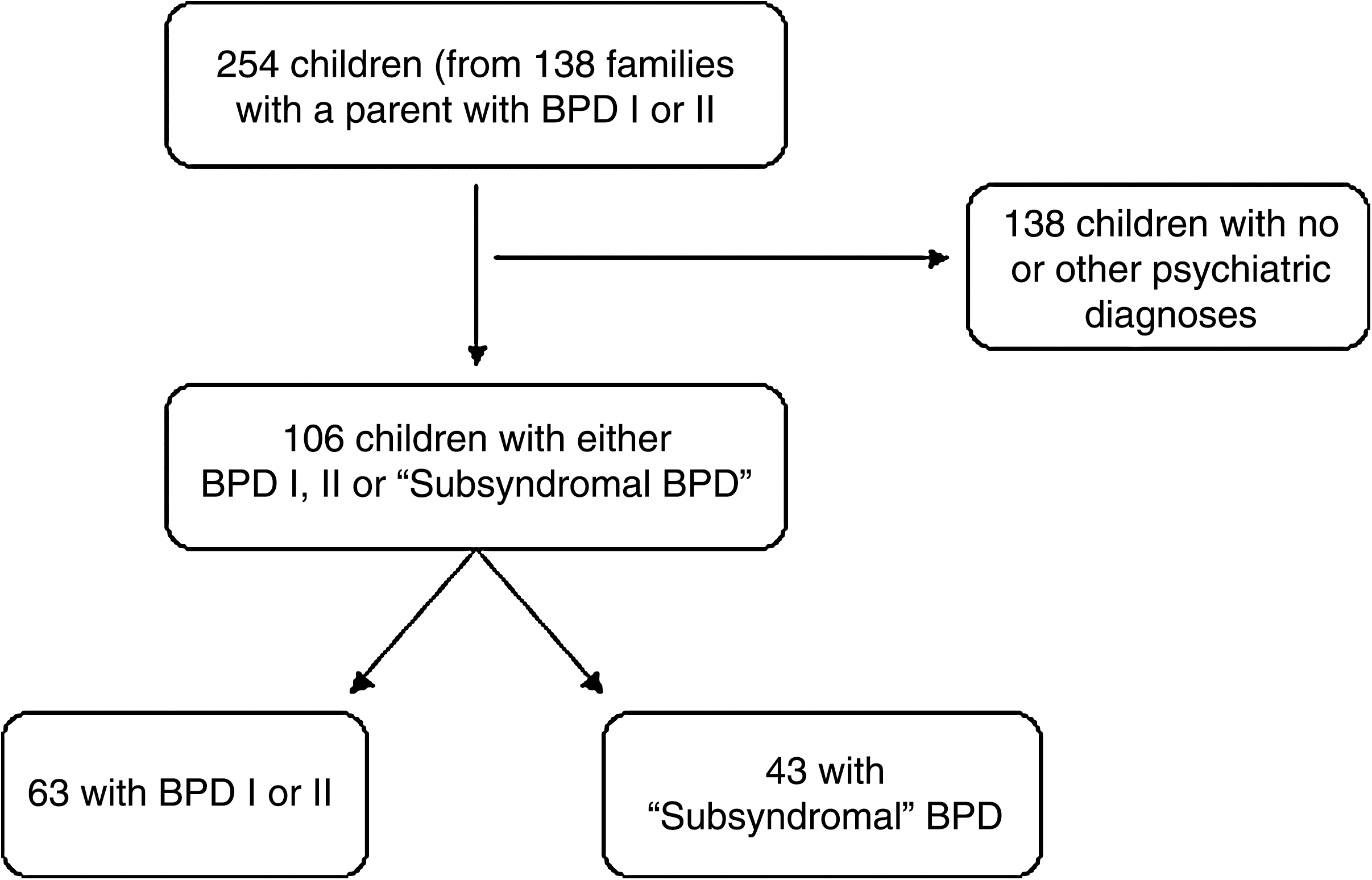
Flow chart depicting path of recruitment of subjects. “Subsyndromal bipolar disorder (BD)” was defined as subjects having attention-deficit/hyperactivity disorder (ADHD) and significant mood symptoms, as determined by a co-morbid mood disorder (major depressive disorder [MDD], dysthymia, cyclothymia) or a Young Mania Rating Scale (YMRS) >12 or Children's Depression Rating Scale–Revised (CDRS-R) >28. BD = bipolar disorder.
Parents and offspring were diagnosed by semistructured interviews, using the Structured Clinical Interview for DSM-IVAxis I Disorders (SCID) (First et al. 1995) for parents and the Washington University in St. Louis Kiddie Schedule for Affective Disorders and Schizophrenia (WASH-U K-SADS) (Geller et al. 1996) for offspring.
We obtained family history of mood disorder using the Family History–Research Diagnostic Criteria (FH-RDC) (Andreasen et al. 1977) and parental history of ADHD using the behavioral disorders supplement from the K-SADS–Present and Lifetime version (K-SADS-PL) (Kaufman 1997). We also assessed current manic symptom severity using the Young Mania Rating Scale (YMRS) (Young et al. 1978) and depression symptom severity using the Children's Depression Rating Scale–Revised (CDRS-R) (Poznanski and Mokros 1995). Subjects were included in the BD group if they had a diagnosis of BD I or BD II, and the subsyndromal BD group if they had a diagnosis of ADHD with significant mood symptoms, as determined by a co-morbid mood disorder (MDD, dysthymia, cyclothymia) or a YMRS >12 or CDRS-R >28. We used the term “subsyndromal” to indicate that they did not meet the syndromal criteria for a full manic episode, even though subjects could have only depressive symptoms in addition to symptoms of ADHD.
Psychotropic medication exposure history was obtained through interviewing the child and parent(s), reviewing medical records, and interviewing the treating physician when possible. The medications examined were stimulants, antidepressants (SSRIs and tricyclic antidepressants [TCAs]), atypical antidepressants (venlafaxine, bupropion, trazodone), antipsychotics, mood stabilizers (lithium, divalproex, and carbamazepine), and other anticonvulsants (oxcarbazepine, topiramate, gabapentin). Duration of medication exposure was rounded to the nearest month. Exposure for less than 2 weeks of a medication was not counted as medication exposure (unless there was a clear reaction to the medication, such as a worsening of mood or mania). Total months exposed were calculated by adding all separate months of exposure for that particular medication type.
We considered the AAO of BD to be the age, rounded to the nearest month, at which the child first met criteria for a manic or hypomanic episode according to the Diagnostic and Statistical Manual of Mental Disorders–Text Revision (DSM-IV-TR) (American Psychiatric Association 2000). This was chosen over age at first affective episode due to the question of whether treatment with stimulants or antidepressants led to earlier mania. However, we did not consider a manic episode that was clearly linked to de novo antidepressant use to be the first “true” manic episode, because according to the DSM-IV-TR, this would be a manic episode due to medication. To obtain first presentation of manic symptoms, we used the questions within the WASH-U-K-SADS to find the earliest age at which children met criteria for mania. For example, if a child exhibited a significant episode of irritability at age 6 years 7 months, but did not have other symptoms of mania until meeting a full episode criteria at 9 years 4 months, we considered 9 years 4 months to be the AAO of mania.
Statistical analysis
Descriptive statistics, means, standard deviations (SD), and percentages were used for all continuous and categorical variables, respectively. Because AAO data were normally distributed, independent t-tests were used to compare AAO between groups with and without particular medication exposure. Significance threshold was considered to be p = 0.05, except for the analysis of medications thought to cause earlier AAO, for which a Bonferroni correction was used to set the threshold at p = 0.025. No corrections for multiple comparisons were used for exploratory analyses of effects of medications other than stimulants, antidepressants, and mood stabilizers on AAO.
Results
Medication exposure in offspring with subsyndromal BD
The offspring with subsyndromal BD consisted of 43 subjects (30 male, 13 female) with a mean age of 12.3 ± 2.8 years (Table 1). Of these subjects, 42% had at least two co-morbid psychiatric diagnoses, with 39.5% having a diagnosis of MDD, 41.9% generalized anxiety disorder (GAD), 34.5% oppositional defiant disorder (ODD), and 100% ADHD. Regarding parents, 53.5% had BD I, 46.5% had BD II, and 69.8% of parents with BD were mothers. The percent of first- or second-degree relatives (of the child) in each family having a history of mood disorder was 49% ± 13%. Four offspring subjects (9.3%) had a history of psychosis.
Abbreviations: BD = bipolar disorder; GAD = generalized anxiety disorder; ADHD = attention-deficit/hyperactivity disorder; ODD =oppositional defiant disorder; MDD = major depressive disorder; YMRS = Young Mania Rating Scale; CDRS = Children's Depression Rating Scale; N/A = not applicable.
The mean number of psychotropic medications ever taken by these subjects was 2.7 ± 1.9. Of these 43 offspring, 62.8% had been exposed to stimulants, 39.5% SSRIs, 25.6% atypical antidepressants (nefazadone, buproprion, or venlafaxine), 7.0% TCAs, 34.9% mood stabilizers (lithium, carbamazepine, valproate), and 27.9% atypical antipsychotics (risperidone, olanzapine, and quetiapine
Abbreviations: SSRIs = Selective serotonin reuptake inhibitors; TCAs = tricyclic antidepressants.
Medication exposure in offspring with BD
There were 63 offspring with BD (42 male, 21 female), diagnosed with BD I (77.8%) or BD II (22.2%), and with a mean age of 13.1 ± 3.5 years (Table 1). Of the parents with BD, 55% had BD I, 45% had BD II, and 76.7% were mothers. The mean percentage of first- or second-degree relatives in each family with a history of mood disorder was 53% ± 20%.
The mean AAO of BD was 11.3 ± 3.7 years and the mean duration of illness was 1.8 ± 1.9 years. The majority (88.3%) of subjects with BD had at least one co-morbid psychiatric diagnosis: 81.0% had ADHD, 55.6% ODD, and 31.7% GAD. Nineteen subjects (30.2%) had experienced psychotic symptoms in the past.
For offspring with BD, the mean number of medications ever taken prior to AAO was 2.2 ± 2.1. Six of the subjects did not have a complete medication history. Sixteen (25.4%) of the subjects had not been on any medications prior to AAO. Forty one of the remaining subjects had been exposed to psychotropic medications: 46.7% stimulants, 51.7% SSRIs, 15% TCAs, 39.7% atypical antidepressants, 23.7% mood stabilizers (11.9% lithium, 11.7% valproate), and 10.2% atypical antipsychotics (Table 3). Furthermore, 15.9% had been exposed to both SSRI and mood stabilizers, and 28.6% had been exposed to both SSRIs and stimulants.
Abbreviations: AAO = Age at onset of bipolar disorder; SD = standard deviation; SSRIs = selective serotonin reuptake inhibitors; TCAs = tricyclic antidepressants.
Lifetime medication exposure in offspring with BD
At time of assessment, 65.1% of the offspring with BD had been exposed any time in their life to stimulants, 14.3% TCAs, 69.8% SSRIs, 69.8% mood stabilizers (49.2% valproate, 27.0% lithium), 56.7% antipsychotics, and 55.6% atypical antidepressants (Table 2). The mean number of medications offspring with BD were exposed to was 4.2 ± 2.3.
Age at interview was not significantly different between the BD and subsyndromal BD groups (p = 0.24). In addition, parent AAO (p = 0.25), parent co-morbidity, and family history of mood disorder (p = 0.26) were not significantly different between the two groups. However, bipolar offspring with BD had significantly more exposure to most categories of psychotropic medications (stimulants, SSRIs, TCAs, antipsychotics, mood stabilizers) than offspring without BD (Table 2).
Age at onset of BD
Independent t-tests were performed to determine if type of medication exposure was predictive of an earlier or later AAO compared to those who did not have the same class exposure. In offspring with BD, AAO of mania was significantly later if a child had prior exposure to any mood stabilizer (13.0 ± 2.8 years vs. 10.8 ± 3.8 years; t = 2.4, degrees of freedom [df] = 55, p = 0.03). However, previous exposure to SSRIs or stimulants did not significantly affect AAO (Table 3). Exploratory analyses revealed that previous exposure to lithium alone (14.4 ± 1.9 years vs. 10.9 ± 3.8 years; t = 2.1, df = 55, p = 0.04), but not valproate or carbamazepine alone, was associated with later AAO (Table 3). Furthermore, atypical antidepressants, TCAs, and atypical antipsychotics did not have a significant effect on the child's AAO when examined independently (Table 3).
Bipolar offspring who took mood stabilizers prior to AAO did not have a significantly different percentage of first- and second-degree relatives with a mood disorder than those offspring who were not prescribed a mood stabilizer (p = 0.28, df = 53, t = 1.1). In addition, parental AAO of BD was not different between these two groups (p = 0.50, df = 57, t = 0.68). Similarly, bipolar offspring who took lithium prior to AAO did not have a significantly different family history of mood disorder (p = 0.66, df = 53, t = 0.43) or parental AAO of BD than those who did not take lithium (p = 0.87, df = 57, t = 0.17). Therefore, we did not covary post hoc for these possible factors contributing to AAO.
As a further exploratory analysis, we compared AAO of offspring with a history of mood stabilizer and SSRI exposure to those with only SSRI exposure. Offspring with both exposures tended to have a later AAO (14.1 ± 3.4 years vs. 10.8 ± 3.7 years; p = 0.05). However, offspring with a history of mood stabilizer and stimulant exposure had a similar AAO as those with exposure to stimulants alone (12.6 ± 2.0 years vs. 10.8 ± 3.6 years; p = 0.29).
Discussion
Children with BD and subsyndromal BD who are bipolar offspring have high rates of psychotropic medication exposure, even before the onset of a full manic episode. We found children with BD to have taken over two different classes of medications prior to their AAO, which is not surprising because children with BD in the community commonly take three to four medications concurrently (Bhangoo et al. 2003). As hypothesized, bipolar offspring with BD had much higher rates of exposure to all classes of psychotropic medication, including stimulants and antidepressants, than bipolar offspring with subsyndromal BD. However, a causal relation cannot be made; that is, offspring who had already developed BD may be assumed to have had a more severe course of illness before the first manic episode than those without BD. Because these subjects had high rates of premorbid ADHD and depression, it is likely that they would have been treated with psychotropics at a higher rate, and possibly for longer periods, simply due to their illness burden.
The second section of our analyses yielded surprising results. In the cohort of bipolar offspring with BD, AAO was not significantly related to prior exposure to stimulants or antidepressants. In fact, the mean AAO was later (but not significantly) for those subjects with SSRI exposure than those without.
These data are somewhat contrary to suggestions from other researchers with similar data. DelBello et al. (DelBello et al. 2001a) found prior stimulant exposure to be predictive of earlier AAO of BD in a cohort of manic adolescents. However, while the presence of ADHD was not different in both the group with and the group without stimulant exposure, severity of ADHD was not controlled for. Thus, it is possible that the adolescents who had earlier AAO also had more severe ADHD, which may have necessitated treatment with stimulants. This possibility is supported by studies suggesting earlier-onset BD to be more severe than later-onset BD (Carter et al. 2003). Indeed, a follow-up analysis of these adolescents found that those with stimulant exposure had a worse course of illness (Soutullo et al. 2002)—a finding that does not speak to which condition preceded the other.
Other researchers have noted that stimulant use in children with ADHD and moderate mood symptoms does not predict a bipolar outcome (Carlson et al. 2000b; Galanter et al. 2003) and in fact may be associated with a lower risk for a bipolar outcome (Tillman and Geller 2006). Furthermore, the phenomenon of stimulant rebound may also not be associated with BD in children (Carlson and Kelly 2003). Thus, while stimulants have been reported to trigger de novo manic episodes (Koehler-Troy et al. 1986), it seems unclear if overall stimulant exposure in at-risk children leads to an earlier age at onset of BD.
Similarly, we did not find exposure to antidepressants to be predictive of an earlier AAO of BD in our population. In a chart review of patients on a child inpatient unit, Carlson and Mick (Carlson and Mick 2003) found treatment with SSRIs to increase the risk of “behavioral disinhibition,” whereas stimulant treatment was actually protective for developing such disinhibition. SSRIs have also been reported widely to trigger or exacerbate mania in both adults (Goldberg and Truman 2003) and children (Cicero et al. 2003; Faedda et al. 2004). Martin and colleagues found that in an HMO database of 87,920 patients, those 10–14 years old were most likely to convert from a diagnosis of MDD to BD after being prescribed an SSRI (Martin et al. 2004). In this study of presumed manic conversion, the number needed to harm was 10. In a cohort of bipolar offspring overlapping with the one used for the current study, 50% of prodromal or syndromal children with BD with SSRI exposure had an SSRI-induced manic episode or worsening of mania (Baumer et al. 2006).
These types of reports have led some to hypothesize that the relatively low rate of pediatric-onset BD in Europe compared to the United States might be due to the increased prescribing of antidepressants (and/or stimulants) to American children (Reichart and Nolen 2004; Soutullo et al. 2005). Thus, we were surprised to find that SSRI exposure prior to first manic episode was not associated with an earlier AAO of BD. It is possible that there may be a ceiling effect in this cohort: Our mean AAO of BD was 11.3 years, already a very young age. In this very early-onset population, selected for their genetic propensity for BD development, early exposure to these medications may not have as significant effect on AAO than in a later-onset population. Another explanation is that SSRIs simply did not significantly change the natural course of illness.
While SSRIs clearly may cause a variety of psychiatric adverse effects in children (Wilens et al. 2003), these effects, including manic induction, might not significantly alter the natural course of BD development in a detectable manner. Because we did not count an SSRI-induced manic episode as true mania, children with these episodes may not be at risk for earlier spontaneous manias. Finally, as psychosocial stress is also considered a trigger for mania (Post 1992; Hillegers et al. 2004), it is possible that those offspring with BD who were not treated with SSRIs may have experienced more psychosocial stress, leading to a relatively earlier AAO. This occurrence may have come about coincidentally, or treatment with SSRIs may also have a protective effect in decreasing stress, while still simultaneously destabilizing mood. However, it is very difficult to prove this latter scenario without careful prospective assessments of psychosocial stress in each group.
Concordant with our hypotheses, we found that exposure to mood stabilizers prior to the first manic episode was associated with a later AAO of mania. The reasons that 24% of our sample had this early treatment may be due to the increasing recognition of possible BD in children in our catchment area as well as the increasing use (and comfort of clinicians with the use) of these agents in children. The likelihood that those children with more severe symptoms were the ones receiving mood stabilizer treatment also makes this finding even more impressive. It is possible that these agents provided amelioration of manic and depressive symptoms, leading to improvements in functioning. The improved functioning may have decreased psychosocial stress, leading to later onset of mania. For example, in a 12-week open prospective study, bipolar offspring with early signs of BD, but no history of manic episodes, responded well to divalproex monotherapy, with decreased symptoms of depression and mania and overall decreases in severity of their illnesses (Chang et al. 2003b).
Another similar study found no difference between divalproex and placebo in preventing relapse of mood symptoms in children at high-risk for BD I (Findling et al. 2007). However, no study has prospectively studied such high-risk children long enough to determine whether or not an active agent such as mood stabilizers are more effective than placebo for delaying the onset of full mania. According to the kindling hypothesis (Post 1992), any type of intervention, whether pharmacologic or psychosocial, that would acutely reduce mood symptoms and associated stress could then diminish the likelihood or delay the onset of fully expressed future episodes.
In exploratory analyses, we also found that subjects with a history of mood stabilizer and SSRI exposure tended to have later AAO than those who had only SSRI exposure. However, we could not be sure that this exposure happened concurrently; therefore, it is premature to comment further on the clinical implications of this finding.
Thus, mood stabilizers might lead to prevention of BD, not just treatment of acute symptoms. Agents such as lithium and valproate have been shown to have intrinsic neuroprotective qualities in vitro (Manji et al. 2000). In humans, lithium may acutely increase gray matter volume (Moore et al. 2000; Foland et al. 2008). We also reported that treatment with lithium or valproate in children with BD was associated with relatively normal amygdala gray matter volumes, significantly greater than children with BD without such exposure (Chang et al. 2005). Our post hoc analysis implicated lithium more strongly as being associated with later AAO, and thus lithium may hold more promise as a prophylactic agent despite its possible inefficacy in treating acute depression in bipolar offspring (Geller et al. 1998). It is possible that certain agents may only be effective if administered early enough in the course of illness. Further research also needs to be conducted with atypical antipsychotics in this regard, because, although we did not find that exposure to this class of medication was associated with delayed AAO of mania, a previous study found quetiapine effective acutely in reducing mood symptoms in an at-risk population (DelBello et al. 2007).
Limitations
Foremost, this was a retrospective study that relied on parental and child report for both AAO and medication exposure data. Although we did attempt to use medical records, this was not always possible. Therefore, some data regarding onset of manic symptoms and medications were subject to parental and subject memory. This type of reporting may be problematic, but we are not aware of any directly relevant research that found this type of AAO determination or medication report to be unreliable. One study of childhood depression found that parents reported earlier AAO for depression of their child than the child themselves (Braaten et al. 2001). Also, parent-report of bipolar symptoms in general appears to be more accurate than child report (Youngstrom et al. 2004).
Because children were newly diagnosed or within a few years of their AAO, this retrospective data may have been more accurate that retrospective studies of AAO in adults. We did not examine dosages or serum levels of medications; it is possible that some subjects were not adequately treated with full doses of these medications. We also were not able to determine if concurrent mood stabilizer treatment was somehow “protective” of SSRI or stimulant treatment, as many children had times of both monotherapy and concurrent treatment. Finally, we studied AAO of first manic episode rather than first mood episode or first behavioral disorder. For early-onset BD, it is often difficult to determine when the illness truly began (Chang et al. 2003a), but for purposes of distinguishing BD from other disorders such as uncomplicated ADHD or unipolar depression, we decided to use first manic episode as our AAO index event.
Clinicial implications
Despite the retrospective nature of data acquisition, this is the first study to report that treating children with mood stabilizers early in BD development may delay the onset of their first full manic episode. Furthermore, our results support other literature suggesting that stimulants do not lower AAO of mania in this population (Craney and Geller 2003; Tillman and Geller 2006). This finding may be important because many children with early-onset BD first present with ADHD before mania onset (Faraone et al. 1997; Chang et al. 2000; Tillman et al. 2003). Thus, treating these children at risk for BD carefully with stimulants may not lead to an earlier manic episode.
Our finding that SSRI exposure was not correlated with an earlier AAO should be regarded with some caution. It is clear that SSRIs can cause de novo manic episodes in children and adolescents (Jerome 1991; Go et al. 1998; Diler and Avci 1999; Martin et al. 2004), similar to adults (Goldberg and Truman 2003). As children in clinical trials of SSRIs have had greater adverse outcomes of increased suicidal behavior than those on placebo (Ryan 2005; Wong et al. 2004), it is possible that these children may have been in the first stages of a mixed or manic episode. For this study, it is important to remember that we did not consider antidepressant-induced mania as the first manic episode qualifying a child for full BD, because it was caused by an exogenous medication. Nonetheless, until further data exonerates the role of SSRIs in BD development, we would recommend that clinicians still carefully monitor those children and adolescents with early signs of mania or family histories of BD who are placed on these agents. Meanwhile, prospective longitudinal studies of children and adolescents at high risk for BD examining medication exposure will help to answer more definitively the questions surrounding the role of psychotropic medication exposure in BD development.
Footnotes
Disclosures
Kiki D. Chang, M.D., has done research for and received grants from AstraZeneca Pharmaceuticals, Eli Lilly and Company, Otsuka America Pharmaceutical, Inc., and GlaxoSmithKline; is on the Speakers' Bureau for AstraZeneca Pharmaceuticals, Bristol-Myers Squibb, and Eli Lilly and Company; is a consultant for AstraZeneca Pharmaceuticals, GlaxoSmithKline, and Eli Lilly and Company; and is on the Advisory Board of Eli Lilly and Company. Dr. Saxena, Ms. Howe, and Ms. Simeonova have no conflicts of interest or financial ties to disclose.
Acknowledgments
The authors gratefully acknowledge the assistance of Leena Khanzode, M.D. in the preparation of this manuscript.
Portions of this manuscript were presented at the 2003 Annual Meeting of the American Psychiatric Association, San Francisco, California.
This work was supported in part by a grant from the Heinz C. Prechter Fund For Manic Depression, a NARSAD Young Investigators Award, a Klingenstein Third Generation Foundation Fellowship, and National Institutes of Health (NIH) grant MH64460-01 (Dr. Chang).