
Abstract
In clinical samples, juvenile bipolar disorder (JBPD) is frequently accompanied by co-morbid attention-deficit/hyperactivity disorder (ADHD). Clinical trials assessing combined psychopharmacological interventions in this population are scarce, and methylphenidate (MPH) may worsen manic symptoms. We conducted a randomized crossover trial with MPH and placebo (2 weeks each) combined with aripiprazole in children and adolescents (n = 16; 8–17 years old) with JBPD and ADHD who had a significant response in manic symptoms with aripiprazole but still presented clinically significant symptoms of ADHD. ADHD, manic, and depressive symptoms were assessed by means of standard scales. Fourteen out of the 16 subjects completed the trial. No significant differences between the effects of methylphenidate and placebo were detected in ADHD (F1, 43.22 = 0.00; p = 0.97) or manic (F1, 40.19 = 0.93; p = 0.34) symptoms. Significant improvement in depressive symptoms was observed in the MPH group (F1,19.03 = 7.75; p = 0.01) according to a secondary self-reported outcome measure. One patient using aripiprazole and MPH discontinued the trial due to the onset of a severe mixed episode. No other significant adverse events were observed. Although MPH did not worsen manic symptoms, it was not more effective than placebo in improving ADHD symptoms in children and adolescents with JBPD co-morbid with ADHD stabilized with aripiprazole. Further investigations are warranted. This study is registered at
Introduction
In spite of the several studies trying to differentiate clinical manifestations peculiar to JBPD and ADHD, studies assessing interventions for the dual diagnoses are scarce (Galanter and Leibenluft 2008). Mood stabilizers and/or atypical antipsychotics are the main agents to treat bipolar disorder (BPD) in children and adolescents (McClellan et al. 2007).
Aripiprazole has shown efficacy and safety in investigations in adult samples with BPD (Vieta et al. 2005; Keck et al. 2006) and more recently in children and adolescent studies. We are aware of two open trials of aripiprazole in JBPD (Biederman et al. 2007; Tramontina et al. 2007), where effectiveness was observed in improvement of mania and overall good tolerability. Findings were controversial regarding changes in weight. Two randomized clinical trials (RCTs) are available. A large (n = 296) multicenter study found that adolescents with BPD (10–17 years old) presented significant reductions in manic symptoms with the use of aripiprazole 10 or 30 mg (Chang et al. 2007). In the other RCT of 43 children and adolescents (8–17 years old) with BPD I or II, aripiprazole was superior to placebo in improving manic symptoms, but not in changes in ADHD, depressive symptoms, and weight (Tramontina et al. 2009). Good tolerability was observed. On the basis of the data available, the Food and Drug Administration (FDA) approved aripiprazole for BPD in children older than age 10 (FDA Website 2008).
Stimulants, like methylphenidate (MPH), are first-line treatment for ADHD (American Academy of Child and Adolescent Psychiatry 2007). However, some old reports suggest that the use of stimulants in children and adolescents might be a risk factor for the development of mania (see Koehler-Troy et al. 1986) and psychosis (Cherland and Fitzpatrick 1999). More recent literature addressing treatment of ADHD in patients with JBPD has suggested a positive response to stimulants, not supporting the idea that stimulant use predicts mania or psychosis (Carlson et al. 1992; Biederman et al. 1999; Kowatch et al. 2003; Pavuluri et al. 2004; Kowatch et al. 2005b).
Two previous RCTs have been published to our knowledge on this issue (Scheffer et al. 2005; Findling et al. 2007). Scheffer et al. conducted a two-stage trial, where the first phase was an 8-week open trial of divalproex sodium (Scheffer et al. 2005). Patients with JBPD and ADHD (n = 40) who presented improvement of manic symptoms according to the Young Mania Rating Scale (YMRS), but no significant improvement of ADHD symptoms according to Clinical Global Impressions–Improvement scale (CGI-I), were invited to join a 4-week randomized, double-blind, placebo-controlled, crossover trial of mixed amphetamine salts (MAS), in the dose of 5 mg twice daily (n = 30, age range 8–17 years old). Significant improvement in ADHD symptoms was observed in the MAS group, whereas no significant between-group change in the YMRS was detected. MAS were considered safe and effective without promoting destabilization of BPD.
Findling et al. conducted a 4-week double-blind, placebo-controlled, crossover trial of MPH in 16 children and adolescents with the co-morbidity (Findling et al. 2007). Best dose week of treatment (5 mg/10 mg/15 mg twice daily) was compared to placebo, and a significant difference was observed between medicated and nonmedicated groups in the ADHD Rating Scale-IV (ADHD-RS-IV) and Connors' Parent Rating Scale. No significant difference was observed in the changes in scores of the YMRS and the Children Depression Rating Scale–Revised (CDRS-R).
Due to both high co-morbidity rates of ADHD among JBPD patients and the scarcity of studies investigating the treatment of both conditions, our objective was to assess response to MPH in children and adolescents with JBPD and ADHD previously stabilized with aripiprazole. Our hypothesis was that patients would present a significantly higher response to MPH than to placebo in ADHD symptoms, while no significant mood changes would be detected during the trial.
Methods
Subjects
Subjects were recruited from two previous investigations: (1) A double-blind, placebo-controlled clinical trial of aripiprazole (registered at
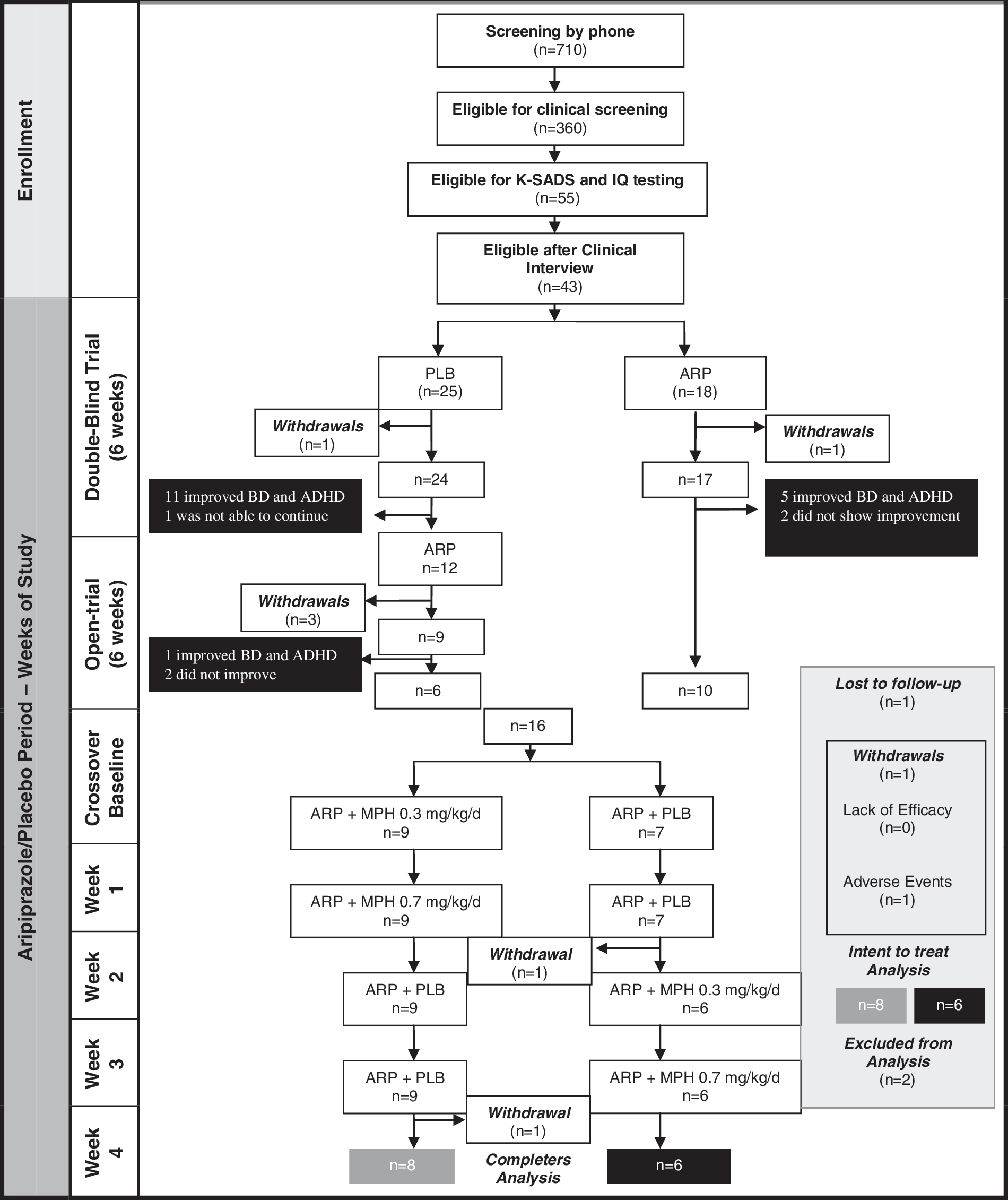
Study phases. K-SADS = Schedule for Affective Disorders and Schizophrenia for School-Age Children; IQ = Intelligence Quotient; BD = bipolar disorder; ADHD = attention-deficit/hyperactivity disorder; ARP = aripiprazole; PLB = placebo; MPH, methylphenidate.
Inclusion criteria for the trials were: (1) Age ranging from 8 to 17 years; (2) diagnoses of BPD I or II co-morbid with ADHD according to Diagnostic and Statistical Manual Mental Disorders, 4th edition (DSM-IV) criteria (American Psychiatric Association 1994); (3) clear reports of ADHD symptoms onset preceding any mood symptomatology; (4) at least 30% improvement in mood symptoms in the previous trials of aripiprazole; (5) residual attention, hyperactivity, and opposition symptoms defined as a Swanson, Nolan, and Pelham Scale IV Version (SNAP-IV) score ≥1.5. Exclusion criteria were: (1) Estimated intelligence quotient (IQ) lower than 70 assessed using the Wechsler Intelligence Scale for Children, 3rd edition (WISC-III) by a trained psychologist (Wechsler 1991); (2) use of any medication besides aripiprazole 10 weeks before entering the study; (3) diagnoses of pervasive developmental disorder, schizophrenia, substance abuse, or dependence; (4) severe suicide/homicide risk counterindicating outpatient treatment; (5) history of hypersensitivity to aripiprazole or MPH; (6) any other acute or chronic disease that may interfere in the study; and (7) pregnancy.
Parental written informed consent and children's verbal assent were obtained. This study was approved by the ethical committee of the Hospital de Clínicas de Porto Alegre, and it is registered at
Diagnostic assessment
The initial assessment comprised a telephone interview conducted by a child psychiatrist for identification of eligible candidates. When primary caregivers endorsed symptoms of BPD and ADHD according to DSM-IV criteria in their children and exclusion criteria were ruled out, children and adolescents underwent a confirmatory three-stage process, described in Tramontina et al. (2007). The evaluation was composed of: (1) A semistructured interview using the Schedule for Affective Disorders and Schizophrenia for School-Age Children–Epidemiological Version (K-SADS- E) (Orvashel 1985), modified to assess DSM-IV criteria and applied to parents by trained research assistants; (2) review of each diagnosis derived through the K-SADS-E in a clinical committee; and (3) clinical evaluation by an experienced child psychiatrist who previously received the results of the K-SADS-E. Priority was always given for the final clinical diagnoses if a diagnostic disagreement occurred in this three-stage process.
Treatment protocol
An independent third party randomized patients into groups A and B and prepared weekly pill pack supplies of aripiprazole (with the same dose from the previous double-blind or open trial ranging from 5 to 20 mg, mean 12.81, standard deviation [SD] 6.32) and MPH or placebo (PLA). Aripiprazole was administered once a day. MPH immediate release (IR) was supplied in fixed doses, according to weight. MPH IR and placebo were administered twice a day. Patients from group A followed the sequence (PLA, PLA, MPH 0.3 mg/kg per day to MPH 0.7 mg/kg per day), and group B received MPH 0.3 mg/kg per day, MPH 0.7 mg/kg per day, PLA, PLA). Because the baseline mean weight of the sample was 47.70 kg, mean dose in the first week of treatment was 15 mg (10 mg in the morning and 5 mg in the afternoon) and 35 mg during the second week (20 mg in the morning, and 15 mg in the afternoon). A pharmacist packaged MPH and matching placebo in capsules, so that they could not be differentiated by shape, color, smell, weight, or taste.
Patients were assessed weekly for 4 weeks after the baseline evaluation. No concomitant medication was allowed during the study period. Compliance was checked by self-report, mother's report, and pill counting in the blister packs returned at the end of each week. After all the four assessments were completed, the study blind was broken.
Efficacy measures
Primary outcome measures
Between-group differences in weekly scores in the Brazilian versions of the SNAP-IV and of the YMRS (MTA Cooperative Group 1999; Youngstrom et al. 2002; Vilela et al. 2005; Mattos et al. 2006). The SNAP-IV is a Likert scale ranging from 0 to 3, and it has been frequently used to assess clinical interventions in ADHD (MTA 1999; Mattos et al. 2006). The YMRS is an 11-item scale to assess changes in manic symptoms along time. It has been the most used instrument in clinical trials with children and adolescents with JBPD (Youngstrom et al. 2002). Changes in depressive symptoms were evaluated with the Brazilian version of the CDRS-R (Poznanski et al. 1979; Barbosa et al. 1997). This instrument is a 17-item clinician-administered scale that assesses presence and severity of depressive symptoms.
Secondary outcome measures
Between-group differences in weekly scores of: (1) The Child Mania Rating Scale-Parent Version (CMRS-P), a parental report on severity of manic symptoms (Pavuluri et al. 2006). Because there was not any Portuguese-validated version of the CMRS-P when the study was conceptualized, we conducted a process of translation and back-translation of the instrument by independent teams, and the final version was approved by the authors of the scale (consistency and test–retest reliability of the original version are both 0.96). (2) Clinical Global Impressions-Severity (CGI-S), an instrument widely used in psychopharmacological interventions (its scores range from 1 = not at all ill to 7 = extremely ill), was applied to rate severity of overall illness (BPD and ADHD) (Guy 2000); and (3) the Kutcher Adolescent Depression Scale (KADS) (Brooks et al. 2003). This scale is an 11-item self-report instrument to detect and monitor depression in adolescents. Its mean correlation with clinician-administered depression rating scales is 0.69. Because no previous Portuguese-validated version of the KADS was available, we again conducted a process of translation and back-translation of the instrument by independent teams, and the final version was approved by the authors of the scale.
Adverse events
Stimulants adverse events were also checked weekly through Barkley Stimulants Adverse Events Rating Scale (SAERS), an instrument frequently used in trials of MPH (Barkley et al. 1990; Zeni et al. 2007). Adverse events were also assessed using an open question (“Have you felt anything different since last week?”). According to recommendations from experts (Greenhill et al. 2004), we complemented the assessment of adverse events with a checklist of all 49 adverse events associated with the use of aripiprazole described in the literature. Weight was assessed weekly.
Statistical analyses
Analyses of primary and secondary outcome measures were performed using a mixed-effects model (MEM) approach that provides a flexible framework for the analysis of repeated measures while accounting for missing data (i.e., lost to follow-up). For each analysis, the best covariance structure fitting the data was selected using Akaike's Information Criterion (AIC).
Treatment, period, sequence, and dose-within-treatment were fixed variables. Covariables were baseline scores for each instrument. A significance level of 5% was set for all analyses. Analyses were carried on using the software SPSS for Windows, version 15. No carry-over effect was expected, because MPH is suitable for crossover designs due to its clinical response limited to no more than 4–5 h, avoiding carry-over effects (Szobot et al. 2008).
Results
Fourteen out of the 16 patients enrolled completed the trial. Baseline characteristics of the final sample are presented in Table 1. Of note, patients presented low rates of manic symptoms (YMRS scores of 11.14 ± 9.32 in the whole sample; 14.66 ± 10.34 in the group receiving placebo followed by MPH; 8.5 ± 8.14 in the other group) due to the previous use of aripiprazole and moderate ADHD symptoms (SNAP-IV baseline scores of 1.64 ± 0.54 for the whole sample; 1.83 ± 0.61 in the group receiving placebo followed by MPH; SNAP-IV baseline scores of 1.50 ± 0.45 in the other group).
Abbreviations: ADHD = Attention-deficit/hyperactivity disorder; IQ = intelligence quotient; YMRS = Young Mania Rating Scale; CMRS-P = Child Mania Rating Scale–Parental Version; SNAP-IV = Swanson, Nolan, and Pelham Scale–version IV; CDRS-R: Children Depression Rating Scale–Reviewed; KADS: Kutcher Adolescent Depression Scale; CGI-S =Clinical Global Impressions–Severity Scale; Barkley SAERS = Stimulant Adverse Events Rating Scale.
One patient using aripiprazole 20 mg at bedtime and MPH 20 mg (10 mg twice a day [b.i.d.]) left the protocol in the second week due to the need of hospitalization and was excluded from the analyses. She had not complied to the medication regimen the week before the mixed episode, and she presented a YMRS score of 43 (severe mania), CDRS-T of 55 (indicating current depression), SNAP-IV score of 3 in all subscales (severe inattention, hyperactivity, and opposition scores), and CGI-S of 7 (extremely ill). Another patient using aripiprazole and placebo did not present for the final assessment and was also excluded from the analyses. Complementary analyses were conducted including the subject who did not show up for the final visit using last observation carried forward (LOCF) (data available by request), but no significant change was detected from the results described below.
Compliance was acceptable during the trial: 95.67% for the whole trial (1194 doses taken out of 1248), and for each treatment as well (aripiprazole, 94.29%; placebo, 97.23%; MPH, 95.57%). Results for all outcomes are reported in Table 2.
Abbreviations: SNAP-IV = Swanson, Nolan and Pelham Scale-IV; YMRS = Young Mania Rating Scale; CDRS-R = Children Depression Rating Scale–Revised; CMRS-P = Child Mania Rating Scale–Parental Version; KADS = Kutcher Adolescent Depression Scale; CGI-S = Clinical Global Impressions Scale–Severity Subscale; SAERS = Barkley Stimulant Adverse Events Rating Scale.
Primary outcomes
ADHD
The MEM analyses revealed no significant treatment (p = 0.97), period (p = 0.42), or sequence (p = 0.93) effects over ADHD symptoms according to SNAP-IV score changes. Baseline SNAP-IV scores were significantly associated with response to treatment (p ≤ 0.05 for all SNAP-IV subscales). Analyses aggregating data for placebo and MPH from the two different periods were conducted through t-tests, but results remained not significant.
Mania
No significant treatment (p = 0.34), period (p = 0.16), or sequence (p = 0.81) effects were observed in YMRS score changes. The baseline YMRS score was significantly associated with response to treatment (F1,12.03 = 16.44; p ≤ 0.01).
Depression
CDRS-R score changes were not significantly associated to treatment (p = 0.54), period (p = 0.81), or sequence (p = 0.98) effect in MEM analyses. We also did not find the effect of the CDRS-R baseline score (p = 0.63)
Secondary outcomes
Mania
According to parental report in the CMRS-P, MEM analyses revealed no significant treatment (p = 0.09), period (p = 0.19), or sequence (p = 0.43) effect over manic symptoms. Significant dose-within-treatment effect (F1,34.7 = 4.05; p = 0.05) was detected. Baseline CMRS-P scores were also associated to response in manic symptoms (F1,14.23 = 189.22; p < 0.001).
Depression
According to the youth's self-report, a significant treatment effect was observed (F1,19.03 = 7.75; p = 0.01). No significant period (p = 0.92), sequence (p = 0.3), or dose-within-treatment differences (p = 0.87) were detected. Also, the baseline KADS score was associated with changes in KADS scores (F1,14.98 = 5.14; p = 0.04)
Global impressions
No significant treatment (p = 0.6), period (p = 0.68), or sequence (p = 0.97) effect on global functioning was observed according to the CGI-S score. The baseline CGI-S score had a significant effect in the outcome (F1,15.06 = 15.20; p = 0.001).
Adverse events
The MEM analyses revealed no significant treatment (p = 0.26), period (p = 0.42), or sequence (p = 0.77) effect on the onset of adverse events related to stimulants as measured by the SAERS. Baseline SAERS score had a significant effect on final scores (F1,15.10 = 45.02; p < 0.01). (See Table 3 for detailed frequency of adverse events related to stimulants along the trial.) Also, no significant treatment (p = 0.12), period (p = 0.35), or sequence (p = 0.89) effect was detected on the onset of adverse events related to the addition of stimulants in the frequency of adverse events related to the use of aripiprazole. Baseline adverse events count had a significant effect on final results (F1,13.40 = 13.6; p < 0.01). Moreover, no significant treatment (p = 0.35), period (p = 0.29), or sequence (p = 0.08) effect of MPH over weight was observed, when compared to placebo.
Scores are presented as means (standard deviation). Scores in each item of the SAERS range from 0 (absent adverse event) to 9 (severe).
Abbreviations: MPH = Methylphenidate; SAERS = Barkley Stimulant Adverse Events Rating Scale.
Discussion
In a 4-week crossover trial of MPH versus placebo in children and adolescents presenting BPD co-morbid with ADHD previously stabilized with aripiprazole, we found no significant between-group differences in changes in attention, hyperactivity, mania symptoms, and weight. A significant response in depressive symptoms was observed, according to a secondary self-report measure.
Our findings regarding ADHD differ from those found in previous studies. The trial with MAS in patients previously treated with divalproex (Scheffer et al. 2005) reported stimulants to be more effective than placebo. However, that study presented some limitations, such as the absence of a specific measure of ADHD, so that the observed “attentional” effect may be related to changes in mania. The only RCT conducted with MPH showed a significant effect of MPH over placebo in ADHD symptoms in patients previously treated with lithium and/or divalproex using a “best dose week” statistical approach (Findling et al. 2007). In that study, the use of concomitant medication was allowed, and the inclusion of BPD not otherwise specified (BPD-NOS) might have promoted significant heterogeneity in a small sample. The current study may have a methodologically more sound design to assess outcomes in such a heterogeneous condition as JBPD, as we only allowed the inclusion of BPD I or II. The open trial conducted by Carlson et al. (1992) also reported improvement of inattention symptoms with the use of the combination of lithium and low doses of MPH (5 or 10 mg).
Our results concur with findings from previous studies regarding exacerbation of mania or onset of psychosis with the use of stimulants. The other RCT using the same psychopharmacological agent (MPH) provided in this trial also found no significant changes in mood symptoms (Findling et al. 2007) according to the same instruments (YMRS and CDRS-R). This strengthens the hypothesis that MPH may preferentially not precipitate or exacerbate manic or psychotic symptoms in patients treated with antimanic or antipsychotic agents (Carlson et al. 1992; Scheffer et al. 2005; Findling et al. 2007). In all the trials, worsening of symptoms is seen as an exception more than as a rule. Although significant changes in mood in the sample as whole were not detected, precipitation of mixed states in our study was 7%. There was 1 patient who presented a severe mixed episode (YMRS = 43, CMRS = 55) after the introduction of MPH 0.3 mg/kg per day. Her grandmother's manic episode and the patient's involvement with school gangs may have triggered this episode. The severity of this episode suggests clinicians should be careful when both medications are used concomitantly, even though the episode may not have been triggered by MPH use.
Improvement of depressive symptoms was only observed by self-report measures. That is not an unexpected finding, due to a more appropriate report of internalizing symptoms by subjects themselves, unlikely of manic symptoms (Herjanic and Reich 1982). Although this result was only found in a secondary measure, making it impossible to exclude Type I error, this finding may warrant future studies of MPH in unremitted bipolar depression after an antimanic agent has stabilized manic symptoms.
MPH was well tolerated, similarly to previous reports from ADHD studies (MTA Cooperative Group 1999), and no particular side effect was responsible for dropouts in the trial. Weight changes did not significantly differ between MPH and placebo. Aripiprazole did not significantly change weight in the early stages of this trial either, suggesting this combination may not promote significant weight changes, a very important clinical issue in the treatment of these subjects. However, the short duration of the trial and its low power suggest caution when generalizing these findings.
Our results should be seen in the context of some limitations: The small sample size may not have allowed us to detect significant differences between placebo and MPH. However, it is important to note that other trials have also been conducted with the same sample size and found significant differences between MPH and placebo (Findling et al. 2007). Important differences in the study design (MPH doses, statistical analyses approach, use of antimanic agents other than atypical antipsychotics) may not enable us to compare our results to the results from those studies. The short-term duration of this trial may also be an important limitation for the observation of significant differences in adverse events between therapeutic agents.
This is the first randomized clinical trial assessing the effect of stimulants combined to atypical antipsychotics in the treatment of children and adolescents with JBPD co-morbid with ADHD. MPH was not more effective than placebo in reducing attention or hyperactivity symptoms in this short-term trial. A secondary finding suggests that depressive symptoms can be ameliorated with the addition of MPH to aripiprazole. Although MPH was found not to destabilize BPD, its use should be considered with caution due to the fact that 1 patient presented a severe mixed episode needing hospitalization during MPH treatment. Clearly, more studies are needed to assess the use of MPH combined with other antimanic agents in the quest for effective treatment for these very impairing co-morbid conditions.
Footnotes
Disclosures
Drs. Zeni and Pheula have received travel grants from Abbott to attend a national research meeting. Dr. Tramontina has been a member of the speakers' board for Abbott. Dr. Ketzer has no financial ties or conflicts of interest to report. Dr. Rohde was on the speakers' bureau and/or acted as consultant for Eli-Lilly, Janssen-Cilag, and Novartis in the last 3 years. Currently, his only industry-related activity is taking part of the advisory board/speakers' bureau for Eli Lilly and Novartis (less than US$10,000 per year and reflecting less than 5% of his gross income per year). The ADHD and Juvenile Bipolar Disorder Outpatient Programs chaired by him received unrestricted educational and research support from the following pharmaceutical companies in the last 3 years: Abbott, Bristol-Myers Squibb, Eli-Lilly, Janssen-Cilag, Novartis, and Shire.
Acknowledgments
The authors would like to thank Roberta Coelho, B.A., Aline Sokolovsky, B.A., and Joana Narvaez, B.A., for neuropsychological assessment, and Clarissa Paim, B.A., for administrative assistance. All acknowledged personnel are from the Federal University of Rio Grande do Sul, Porto Alegre, RS, Brasil. Ms. Coelho, Sokolovsky, Narvaez, and Paim do not have any potential conflicts of interest to disclose.
This work was fully supported by research grants from: Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq, Brazil) (Grant 471761/03-6), and Hospital de Clínicas de Porto Alegre (GPPG 03-325). Aripiprazole was provided by Bristol-Myers Squibb without restrictions. This is an independent investigator trial.