
Abstract
Background:
The aim of this study was to test the efficacy and safety of olanzapine + topiramate versus olanzapine monotherapy in the treatment of bipolar disorder (BPD) and treatment-attendant weight gain in children and adolescents.
Method:
Subjects (N = 40) were outpatients of both sexes, 6–17 years of age, with a Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) diagnosis of BPD (manic, hypomanic, or mixed) and Young Mania Rating Scale (YMRS) total score of >15 treated over 8-week periods in two partially concurrent open-label trials with olanzapine (n = 17) or olanzapine + topiramate (n = 23).
Results:
Subjects in both groups experienced a statistically significant reduction in YMRS scores after 8-week, open-label treatment with olanzapine (baseline YMRS = 26.7 ± 9.5; end-point YMRS = 18.2 ± 12.5, p = 0.04) and olanzapine +topiramate (baseline YMRS = 31.3 ± 7.9; end-point YMRS = 20.4 ± 11.4, p = 0.04). There was no difference in response between the two groups based on YMRS or Clinical Global Impressions–Improvement (CGI-I) scores. Adverse events were few and mild and similar between the two groups, with the exception of weight gain. The weight gain in the olanzapine group was 5.3 ± 2.1 kg and the weight gain in the olanzapine + topiramate group was statistically significantly lower, 2.6 ± 3.6 kg.
Conclusions:
Augmentation of olanzapine with topiramate resulted in a reduced weight gain over the course of an 8-week, open-label trial when compared with olanzapine treatment alone, but did not lead to greater reduction in symptoms of mania.
Introduction
Despite its favorable side-effect profile, however, a significant limiting factor in the use of olanzapine is weight gain. In an open-label study of olanzapine for pediatric-onset BPD, subjects (average age 10 years) gained an average of 5.0 kg over the 8-week period of the medication trial (Frazier et al. 2001). Elevated levels of weight gain (3.7 kg) were also observed in the 3-week, double-blind, placebo-controlled study of adolescents aged 13–17 years (Tohen et al. 2007).
Because the novel antiepileptic drug topiramate has been associated with weight loss, it has been increasingly used in clinical practice to offset the weight gain associated with atypical antipsychotics (Dursun and Devarajan 2000; Werneke et al. 2004; McElroy et al. 2007). Since topiramate also offers the putative advantage of acting as a mood stabilizer, it could not only decrease the hazard of excessive weight gain but could also improve the clinical management of this population (Chengappa et al. 1999; Lung et al. 2009; Tramontina et al. 2007; Wang et al. 2008).
This study addresses whether the co-administation of topiramate with olanzapine results in less weight gain and more robust clinical improvement than when olanzapine is used as monotherapy in children and adolescents with BPD. To our knowledge, this is the first prospective pharmacologic trial for pediatric BPD that combines topiramate with an atypical antipsychotic medication, with the express intention of minimizing weight gain as well as improving clinical response.
Methods
The study consisted of an 8-week, open-label treatment with olanzapine monotherapy or olanzapine augmented with topiramate. All study procedures were reviewed and approved by the Institutional Review Board. All subjects' parents or guardians signed written informed consent forms and all subjects signed assent forms.
Male or female subjects, 6–17 years of age were included in the trial. These two trials were both open-label trials and only in part conducted concurrently. During the time of study overlap, eligible subjects were assigned randomly to either study by alternating assignment for one study then the other. That is, if the last subject signed consent for the olanzapine open-label trial, the next patient would be assigned to the olanzapine plus topiramate study. Each subject met criteria for Diagnostic and Statistical Manual for Mental Disorders, 4th edition, Text Revision (DSM-IV-TR) BPD I, BPD II, or BPD not otherwise specified (NOS) (American Psychiatric Association 2000) and were currently displaying manic, hypomanic, or mixed symptoms (with or without psychotic features) according to DSM-IV-TR on the basis of clinical assessment by an experienced child and adolescent psychiatrist. These diagnoses were confirmed via the structured diagnostic interview Kiddie Schedule of Affective Disorders and Schizophrenia Epidemiological Version (K-SADS). DSM-IV-TR requires subjects to meet criterion A for a period of extreme and persistently elevated, expansive, or irritable mood lasting at least 1 week, plus criterion B, manifested by three (four if the mood is irritable only) of seven symptoms during the period of mood disturbance. Also recorded was the onset of first episode, the number of episodes, offset of last episode, and total duration of illness. BPD II was defined as either: (1) Having severe mood disturbance, which meets DSM-IV-TR criteria A for BPD but fewer elements in criteria B (only require two items for elation category and three for irritability), or (2) having a severe mood disturbance lasting at least 4 days (rather than 1 week) but the full diagnostic requirement of the B criteria.
Severity of symptoms of mania was assessed with the Young Mania Rating Scale (YMRS) (Young et al. 1978; Gracious et al. 2002; Youngstrom et al. 2002). During this baseline evaluation, the clinicians completed the YMRS as a measure of current symptom severity. To be included in the study, subjects must have had a score of 15 or greater on the YMRS. To assess the rates of psychiatric co-morbidity, structured diagnostic interview K-SADS were conducted with mothers. These interviews were administered by highly trained and supervised nonclinician interviewers. All diagnoses were reviewed by a sign-off committee of experienced board-certified child and adolescent psychiatrists chaired by the senior investigator (J.B.).
We excluded subjects with any serious, unstable medical illness, including hepatic, renal, gastroenterologic, respiratory, cardiovascular (including ischemic heart disease), endocrinologic, neurologic, immunologic, or hematologic disease. No subjects were tapered off of their current antimanic medications for the purpose of enrolling in this study unless the current treatment was determined to be ineffective as indicated by continuing to meet entrance criteria (active symptoms of mania and a YMRS Score of ≥15). Mood stabilizers, antimanic agents, anticonvulsants, and other neuroleptic therapy were not allowed during this study. Antidepressants were exclusionary to the study.
Olanzapine was initiated at 2.5 mg/day, with weekly increases of 2.5 mg to 5 mg permitted at the discretion of the clinician, with a maximum dose of 20 mg allowed for the study. For those subjects receiving olanzapine plus topiramate, topiramate was initiated at a dose of 25 mg/day, with weekly increases of 25 mg/day up to the maximum dose of 100 mg/day. Topiramate was titrated to 100 mg in all subjects as tolerated. Some subjects were on lower doses due to clinician assessment of side effects. Olanzapine was titrated to treat BPD according to the dosing schedule. If subjects were currently receiving stimulants or atomoxetine for co-morbid attention-deficit/hyperactivity disorder (ADHD), they would have been continued if, in the clinician's judgment, it was in the best interest of the patients to continue this treatment, the patient did not wish to stop stimulant treatment, and only if the patient had been on a stable dose for at least 30 days. If extrapyramidal symptoms occurred, benztropine mesylate was allowed in doses of up to a maximum of 2 mg/day. The use of the benzodiazepine lorazepam was permitted during the study in doses of 2 mg or less per day for extreme agitation. Nonpharmacological treatments, such as individual, family, or group therapy, were allowed if they were in place before the subject joined the study and if the therapy regimen remained the same throughout the study.
The severity of symptoms of depression was assessed with the Children's Depression Rating Scale–Revised (CDRS-R) (Emslie et al. 1997). Other psychiatric symptom domains were assessed at baseline and end point with the Brief Psychiatric Rating Scale (BPRS) (Lachar, Bailley et al. 2001). We used the approach proposed by Lachar et al. (Lachar et al. 2001) to characterize symptom severity in the BPRS using a modified factor terminology. “Resistance” was renamed Mania Symptoms (Uncooperativeness, Hostility, Excitement, Grandiosity); Positive symptoms (Unusual Thought Content, Conceptual Disorganization, Hallucinatory Behavior, Suspiciousness, Disorientation) and Negative symptoms (Blunted Affect, Emotional Withdrawal, Motor Retardation) remained the same; Psychological Discomfort was renamed Anxious/Depressed (Anxiety, Somatic Concerns, Guilt Feelings, Tension, Depressive Mood, Mannerisms & Posturing).
To assess clinically significant severity and improvement relative to baseline, we used the National Institute of Mental Health (NIMH) Clinical Global Impressions–Severity (CGI-S), and–Improvement (CGI-I) scales (National Institute of Mental Health 1985). CGI severity and improvement were assessed separately for depression, mania, conduct disorder, and ADHD. The score for the CGI-S ranges from 1 (normal, not at all ill) to 7 (among the most extremely ill patients). The score for the CGI-I ranges from 1 (very much improved) to 7 (very much worse).
The YMRS and the CGI-I mania scales were the primary outcome measures identified for this study. Response was defined by having either a 30% reduction in symptoms according to the YMRS score at end point or by having been judged as much or very much improved on the CGI-I (≤2). We also calculated response by the more standard metric of 50% reduction in symptoms according to the YMRS score at end point. These ratings were made at each of the weekly assessments. Our secondary measures of outcome (the CDRS-R and the BPRS) were assessed at baseline, week 4, and at week 8 (or study end point).
Safety was assessed at each visit using spontaneous reports of treatment-emergent adverse events, changes in vital signs, and laboratory measures. Blood pressure and weight were recorded at each visit. Prolactin, glucose, and lipid levels were obtained at baseline and posttreatment. Although every effort was made to obtain fasting levels, this was generally not possible, and lipid tests are not fasting level.
Statistical analysis
Analyses were intention to treat (ITT). A mixed-effects model, repeated-measures approach was used to account for missing data in our longitudinal assessments of safety (i.e., weight and vital signs) and efficacy. Omnibus and pairwise comparisons were made with postestimation Wald tests such that c2 statistics were reported for continuous data. Continuous and categorical data were tested with analysis of variance (ANOVA) and Pearson c2, respectively, for nonlongitudinal data (i.e., demographics at baseline, prevalence of adverse effects, or response at end point, etc.). Statistical significance was determined at p < 0.05.
Results
Forty subjects were enrolled in the trial (n = 17 for olanzapine monotherapy and n = 23 for olanzapine with topiramate augmentation). Seventy two percent (n = 29) of subjects completed the 8-week study. In the olanzapine group, 14 subjects met criteria for BPD I and 3 met criteria for BDP II. In the olanzapine + topiramate group, 22 subjects met criteria for BPD I and 1 met criteria for BPD II. Although permitted in this study, no subject was diagnosed with BPD NOS. The rate of dropout was not statistically significantly greater for olanzapine than for olanzapine + topiramate (n = 4 or 24% versus n = 7 or 30%, respectively; c2 (1) = 0.2, p = 0.6). The reason for dropout was different between treatment arms, however: 100% (n = 7) of dropouts on olanzapine with topiramate augmentation were due to lack of efficacy, whereas 50% of dropouts on olanzapine monotherapy were due to lack of efficacy and 50% (n = 2) were due to adverse effects (c2 (1) = 4.2, p = 0.04). Both subjects dropping out from the study due to adverse effects reported increased appetite at the dropout visit and 1 of the subjects reported tremor. The neurological side effects did not differ significantly between the two treatment groups and included the following specific descriptors: Spacey, tremor, akathasia, dazed, nystagmus, and speech deterioration.
As shown in Table 1, there were no differences between subjects on demographic or clinical variables. The majority of subjects in both groups presented with mania mixed with depression at study entry (Table 1). At study entry symptoms of ADHD and conduct disorder were common in both groups of subjects. Global assessment of function scores indicated that both groups of children were highly impaired (Table 1). The average daily dose of olanzapine in the monotherapy group was 8.6 ± 3.4 mg and was 9.9 ± 5.2 mg in the topiramate augmentation group (F([1.37] = 0.8, p = 0.4). The average dose of topiramate at the end point was 70.5 ±30.5 mg/day. One subject in the olanzapine + topiramate group was on a stimulant and no one in the monotherapy olanzapine group was on a stimulant. No subject was on atomoxetine.
Abbreviations: CGI-S = Clinical Global Impressions–Severity; ADHD = attention-deficit/hyperactivity disorder; GAF = Global Assessment of Functioning.
As shown in Fig. 1, there was a clinically and statistically significant improvement in both the olanzapine monotherapy (Wald c2 (8) = 45.5, p < 0.001) and olanzapine + topiramate groups (Wald c2 (8) = 85.4, p < 0.001) (Fig. 1). At study end point (week 8 or LOCF), there was a 8.5 ± 15.3 point reduction in olanzapine monotherapy and an 10.6 ± 13.0 point reduction in YMRS scores of the olanzapine + topiramate subjects. The response curves illustrated in Fig. 1 over the course of the trial were not statistically significantly different for olanzapine- and olanzapine + topiramate-treated subjects (Wald c2 (8) = 5.1, p = 0.75).
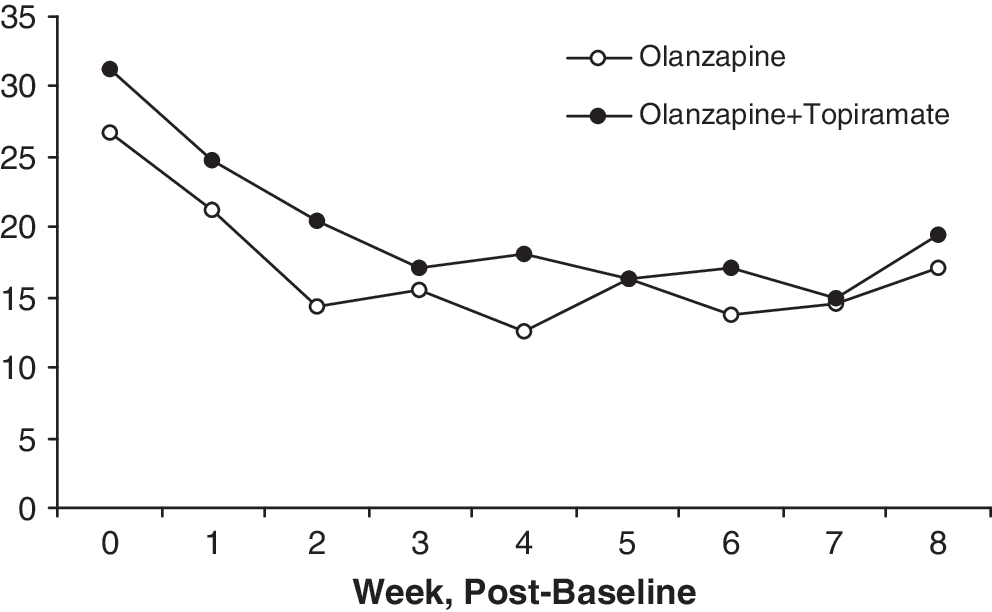
Change in YMRS scores in treated with olanzapine (n = 17) and olanzapine + topiramate (n = 23) in open study over 8 weeks. YMRS = Young Mania Rating Scale.
The rate of improvement according to CGI (CGI-I ≤2) of mania was not statistically significantly different in monotherapy or augmented subjects (Fig. 2). The rate of improvement for depression and the disruptive behavior disorders (in those subjects with active symptoms at baseline) was modest in both groups (Fig. 2).

CGI-rated improvement (defined as CGI-I ≤ 2) in mania and psychiatric co-morbidity among children with CGI-S ≥ 3 at baseline (no between-group differences found). CGI-I = Clinical Global Impressions–Improvement; CGI-S = Clinical Global Impressions–Severity.
We employed an a priori definition of response on manic symptoms of a 30% reduction in YMRS score or being rated as much or very much improved on the CGI. The proportion of subjects with either a 30% reduction (47% versus 50%, c2 (1) = 0.03, p = 0.9) or 50% reduction (47% versus 32%, c2 (1) = 0.9, p = 0.3) in YMRS scores was not statistically significantly different in monotherapy and topiramate augmentation groups. When combined with the CGI results, there was no difference in our definition of response in the monotherapy and augmentation groups (47% vs. 60%, c2 (1) = 0.8, p = 0.4).
The scores from the baseline and end-point assessments of the YMRS, CDRS-R, and BPRS are presented in Table 2. Both groups demonstrated improvement as rated by the YRMS, but only the olanzapine monotherapy group showed any improvement on the BPRS. This improvement was due to a statistically significant change in symptoms of mania and co-morbid positive symptoms. Only subjects in the olanzapine + topiramate group demonstrated statistically significant improvement on depressive symptoms, but the change was of little clinical significance.
YMRS, BPRS,
p < 0.05 from baseline to end point within group.
Abbreviations: YMRS = Young Mania Rating Scale; BPRS = Brief Psychiatric Rating Scale; CDRS-R = Children's Depression Rating Scale-Revised; SD = standard deviation.
There was a statistically significant increase in total cholesterol level in the olanzapine + topiramate group relative to the olanzapine monotherapy group (Table 3). There was a statistically significant increase in glucose and prolactin levels in the olanzapine monotherapy group but not in the augmentation group. Treatment in both groups was associated with an increase in pulse (Table 3).
p < 0.05 from baseline to end point within group.
Abbreviations: SD = Standard deviation.
There was a statistically significant increase in weight from baseline to end point in both the olanzapine + topiramate group (2.6 ± 3.6 kg) and the olanzapine monotherapy group (5.3 ±2.1 kg). The difference in weight gain at end point between these groups was statistically significant (Table 3). z-Scores indicating deviation from growth curves defined by age and gender are presented in Fig. 3 to evaluate the impact of these medications on changes in BMI Over the 8 weeks, the subjects in the olanzapine monotherapy group increased their BMI by 0.6 standard deviations (SDs) relative to population-based norms. The subjects in the olanzapine + topiramate group documented an increase in BMI of 0.3 SDs over 8 weeks.

BMI for age and gender z-scores in subjects treated with olanzapine (n = 17) and olanzapine + topiramate (n = 23) in open study over 8 weeks. BMI = Body mass index.
As illustrated in Fig. 4, the rate of spontaneously reported side effects did not differ between olanzapine- and olanzapine +topiramate-treated subjects with the exception of increased sedation reported with olanzapine monotherapy (p = 0.04). In both groups, the most commonly reported side effects were increased appetite, symptoms of common cold, headaches, and sedation. The neurological side effects did not differ significantly between the two treatment groups and included the following specific descriptors: Spacey, tremor, akathasia, dazed, nystagmus, and speech deterioration.

Side effects and adverse events. GI = Gastrointestinal.
Discussion
We compared olanzapine monotherapy to olanzapine administered with topiramate in an 8-week, open-label trial. Both the olanzapine monotherapy and the olanzapine augmented with topiramate groups experienced similar improvements in manic symptoms as measured by the YMRS scale and the CGI scale for mania. However, the olanzapine + topiramate group experienced half as much weight gain as the olanzapine monotherapy group (2.5 kg vs. 5.1 kg), and this difference was statistically significant. To our knowledge, this is the first study that addresses the strategy of adjunctive topiramate to limit weight gain in youths treated with atypical antipsychotic medication.
Although higher levels of topiramate might be equally or more useful for offsetting weight gain, we chose the dosing ceiling for topiramate of 100 mg, based on clinical observation that weight loss and appetite suppression occurs with low-dose topiramate and considering that clinicians would likely be reluctant to use high doses of a medication with cognitive clouding as a side effect in youth. We reasoned that if we can demonstrate that a low dose with likely lower side effects is useful to offset weight gain, then clinicians might see this as a viable option.
Despite its role as a putative mood stabilizer, the group receiving topiramate did not demonstrate superior improvement in BPD symptoms, nor did its addition to olanzapine result in a lower average dose of olanzapine over the course of the 8-week trial. The olanzapine monotherapy group showed a statistically significant improvement in manic symptoms of the BPRS score whereas the olanzapine + topiramate group improvement did not reach statistical significance. This between-group difference was likely a chance finding due to multiple comparisons.
The research reports regarding topiramate as a putative mood stabilizer have been mixed, with some open-label studies demonstrating reduction of bipolar symptoms, but placebo-controlled studies failing to demonstrate efficacy (Marcotte 1998; Chengappa et al. 1999; McElroy and Keck 2000; Calabrese et al. 2001; Chengappa et al. 2001; Ghaemi et al. 2001; Grunze et al. 2001; Letmaier et al. 2001; DelBello et al. 2002a; Suppes 2002; Delbello et al. 2005).
In contrast, treatment with olanzapine, whether alone or in combination with topiramate, resulted in a marked decrease of manic symptoms. These results are consistent with a previous open-label study, a study of preschoolers, and a large multisite, double-blind, randomized clinical trial. Taken together, these results support the role of olanzapine in the treatment of pediatric BPD (Frazier et al. 2001; Biederman et al. 2005b; Tohen et al. 2006b; Tohen et al. 2007).
However, a serious counterbalance to the effectiveness data is the consistently identified severe weight gain associated with olanzapine treatment in pediatric patients. Considering that weight gain has been associated with disturbance of glycemic and lipid control and the development of hyperinsulinemia and diabetes (Correll and Carlson 2006), it is imperative to develop appropriate measures to address this serious adverse effect.
The reduction in weight associated with topiramate is consistent with previous studies documenting that treatment with topiramate leads to weight loss in other clinical poulations (Gordon and Price 1999; Dursun and Devarajan 2000; Appolinario et al. 2001; Chengappa et al. 2002). A chart review by Chengappa et al. followed the weights of adult psychiatric patients over a 100-day period. These authors reported that those taking valproate gained an average of 6.4 kg, those taking lithium gained an average of 6.3 kg, but those taking topiramate lost an average of 1.2 kg (Chengappa et al. 2002).
Likewise, in a double-blind, placebo-controlled study of topiramate for BPD in youth, subjects lost weight on topiramate and gained weight on placebo (−1.76 kg in the topiramate group vs. +0.95 kg in the placebo group), and 3 out of 11 overweight subjects attained normal weight by study end (Delbello et al. 2005). In a chart review of 16 obese female outpatients with depressive disorder treated with topiramate, body mass index (BMI) decreased significantly, with a mean weight loss of 5.9 kg over 40 weeks (Carpenter et al. 2002). In a case series of 3 adult patients with both BPD and diabetes mellitus type II, topiramate was added to existing medications and followed for 1–2 years. All 3 obese patients experienced dramatic weight loss from 20 kg to 33 kg, plus all three were able to discontinue insulin treatment in favor of oral hypoglycemics (Roy Chengappa et al. 2001).
Although the mechanism by which topiramate leads to weight loss remains unclear, some authors have suggested that it may be due to appetite suppressions while others raise the question as to whether topiramate exerts its weight reduction effects primarily through hypoglycemic effects (Roy Chengappa et al. 2001). Future work might evaluate the safety and effectiveness of additional agents that can offset weight gain as well as elucidate the mechanism of weight gain, such as with measures of insulin and leptin and diaries of caloric intake and exercise.
The finding that cholesterol is higher in the olanzapine +topiramate group versus the olanzapine group alone, despite the lower weight loss, is an unexpected finding and may be due to the fact that the blood tests were not fasting levels. Further research should adhere to fasting blood tests for accurate lipid levels.
Study limitations
Limitations of this study include the heterogeneity of the sample with the majority of subjects diagnosed with BPD I and a minority with BPD II included. Another limitation is the low dose, 100 mg, of topiramate used. Other studies used varying doses up to 350 mg/day, and one study noted that weight loss correlated directly with topiramate dose as well as length of treatment (Carpenter et al. 2002). Whether improved weight control in children and adolescents could be achieved with higher doses of topiramate has yet to be tested. Lipid levels and glucose were not fasting levels, and this is a significant weakness of this study. An additional limitation of this study is the lack of information regarding medications taken in the previous month prior to entry into these studies, as recent prior exposures to medications might influence short-term outcomes regarding weight gain. Other major limitations of this study are that it was an open-label and uncontrolled study and raters were not blind to the treatment condition. Dosing was adjusted based on clinical judgment and was not systematic across subjects. While concomitant ADHD treatment was permitted, only 1 subject was on a stimulant medication, making it impossible to evaluate the utility of this concomitant medication in facilitating weight gain. However, this fact should not affect the weight outcome. As this study used olanzapine only, it is unclear whether these findings can be generalized to the use of adjunctive topiramate with other atypical antipsychotic medications. Despite these limitations, this study supports the use of topiramate administered with olanzapine to minimize the olanzapine associated weight gain in BPD youth.
Footnotes
Disclosures
Janet Wozniak, M.D., is the author of Is Your Child Bipolar?, published May, 2008, by Bantam Books; a consultant for Pfizer, Shire Pharmaceuticals, and Eli Lilly; has received research funding from Eli Lilly and the National Institute of Mental Health (NIMH); and is on the speaker's bureaus of Eli Lilly and Janssen. Jim Waxmonsky, M.D., is on the speaker's bureau of Novartis; has received honoraria from Shire and Scepter; and has received research support from Eli Lilly and Shire Laboratories. Eric Mick, Sc.D., has received research support and is on the Advisory Boards of McNeil Pediatrics, Ortho-McNeil Janssen Scientific Affairs, Pfizer, Shire Pharmaceuticals, and the National Institute of Mental Health (NIMH); and has an advisory or consulting relationship with Pfizer and Shire Pharmaceutical. Liisa Hantsoo, B.A., and Meghan Kotarski, M.B.A., have no conflicts of interest or financial ties to disclose. Joseph Biederman, M.D., is currently receiving research support from Alza, AstraZeneca, Bristol Myers Squibb, Eli Lilly and Co., Janssen Pharmaceuticals Inc., McNeil, Merck, Organon, Otsuka, Shire, NIMH, and National Institute of Child Health and Human Development (NICHD). In previous years, Dr. Biederman has received research support, consultation fees, or speaker's fees for/from the following additional sources: Abbott, AstraZeneca, Celltech, Cephalon, Eli Lilly and Co., Esai, Forest, Glaxo, Gliatech, Janssen, McNeil, NARSAD, NIDA, New River, Novartis, Noven, Neurosearch, Pfizer, Pharmacia, The Prechter Foundation, Shire, The Stanley Foundation, UCB Pharma, Inc., and Wyeth.
This work was supported by a center grant from the Stanley Medical Research Institute and a grant from the Stanley Foundation.