
Abstract
Background:
Still little is known about neuropsychological differences between boys and girls with attention-deficit/hyperactivity disorder (ADHD) and whether there are sex-specific differences in the modulation of attentional performance by methylphenidate (MPH).
Method:
In this study, 27 males and 27 females between 8–12 years old and with ADHD were investigated in a double-blind, placebo-controlled trial on five computerized attention tests (0.25 vs. 0.5 mg/kg MPH as a single dose, versus placebo).
Results:
Boys and girls with ADHD did not differ with respect to age, intelligence quotient (IQ), symptom severity, co-morbidity patterns, and ADHD subtype. However, ADHD boys were more impulsive on a sustained attention task, whereas girls with ADHD had more deficits on tasks measuring selective attention. Attentional performance increased differentially as a function of MPH dose, with some tasks showing linear improvement with higher dosage whereas more complex tasks in particular showed inverse U-shaped patterns of MPH effects. However, these effects were comparable between girls and boys.
Conclusions:
Our data suggest that there are some gender differences in attentional performance in subjects with ADHD in a clinical sample, even if symptom severity and co-morbidity are controlled; however, modulation of attention by MPH does not seem to differ between sexes.
Introduction
Thus, a number of researchers have tried to investigate sex differences in subjects with ADHD with respect to clinical features (in particular, ADHD subtype distribution, symptom severity, or co-morbidity patterns), structural brain abnormalities, and neuropsychological functioning. These studies suggest that symptom severity in girls is higher compared to boys with ADHD, and co-morbid disorders are more common in boys if assessed in clinical samples (Carlson et al. 1997). Neuropsychological studies have provided mixed results, with earlier studies suggesting girls with ADHD are more impaired than boys with ADHD (Gaub and Carlson 1997), whereas more recent studies suggest that girls and boys with ADHD were both impaired in processing speed, but that boys were slower in processing speed than girls (Rucklidge and Tannock 2001) or that girls with ADHD made significantly fewer impulsivity errors than boys with ADHD (Newcorn et al. 2001). More recently, a meta-analysis of neuropsychological studies of adults with ADHD (aged >18 years) investigated whether differences between ADHD and controls vary as a function of age and sex (Balint et al. 2008). The results suggest that males with ADHD have a higher level of impairment, especially for more complex tasks. A limitation of these studies is that attention and its components were tested with only one task, for example, a continuous performance test. As far as we know, a model-oriented comparison of attentional functions between boys and girls with ADHD has yet to be conducted.
In addition, some authors have found that the ADHD subtype and the presence of co-morbid disorders can affect performance on neuropsychological testing (e.g., Epstein et al. 1997; Günther et al. 2009). Girls are diagnosed more often with ADHD of the predominantly inattentive type, and they have higher ratings of internalizing disorders like depression and anxiety (Gershon 2002; Levy et al. 2005). Co-morbid anxiety seems to be associated with better attentional functioning in children with ADHD (Schatz and Rostain 2006; Vloet et al., personal communication), whereas children with disruptive behavior co-morbidities are described as more impulsive and more inattentive than children without such co-morbidities (Halperin et al. 1990; Van der Meere et al. 2005). Thus, the differences in subtype and co-morbidity patterns may result in differences in neuropsychological test results between boys and girls. Therefore, to detect sex differences in ADHD, a model-oriented design is necessary, wherein possible confounders such as co-morbidity and subtype are controlled.
Differences in attentional performance between girls and boys with ADHD and the influence of stimulant medication on attention
Even less is known about sex-specific treatment effects in ADHD. Stimulant medication is the primary medical treatment for ADHD and is recommended in practice guidelines for male and female subjects with ADHD (e.g., American Academy of Child and Adolescent Psychiatry 2002; Rushton et al. 2004; Taylor et al. 2004). However, several studies have documented disparities in treatment rates for boys and girls (Hoagwood et al. 2000; Guevara et al. 2002). Interestingly, males with ADHD are consistently more likely than females with ADHD to use stimulants, even after controlling for symptom characteristics or severity of ADHD (Charach et al. 2006; Miller et al. 2008). Moreover, there is preliminary support for pharmacodynamic differences between boys and girls (Sonuga-Barke et al. 2007), with girls responding better on behavioral ratings than boys 1.5 hours posttreatment but generating inferior response rates by the end of the day. By contrast, the age of initiation and duration of treatment seems to be similar between girls and boys (Barbaresi et al. 2006; Epstein et al. 2006). Aside from behavioral improvements, methylphenidate (MPH) has been shown to enhance cognitive performance in tests measuring aspects of attention, memory, and executive functioning (Kempton et al. 1999; Tucha et al. 2006; Bedard et al. 2007). Only a few studies have explored MPH effects on different aspects of attention using a model-based approach (Konrad et al. 2004; Tucha et al. 2006). Tucha and colleagues (2006) demonstrated that children with ADHD without stimulant medication are markedly impaired in various aspects of attention. Eight different computerized attention tasks were administered to examine different aspects of attention. Impairments were seen in attentional aspects of intensity (arousal, vigilance, and sustained attention), selectivity (selective attention and distractibility), and supervisory attentional system (SAS) (shifting). Furthermore, MPH led to improvements of attentional functioning in children with ADHD. Although MPH improves attention, children with ADHD in this study did not reach a normal level of attentional functioning.
In addition, in a previous study of ours (Konrad et al. 2004), we could show that some aspects of attention (e.g., alertness and sustained attention) improved linearly as a function of dosage, whereas other aspects, like inhibition and shifting (SAS), were enhanced at a low dosage but not at a higher dosage (U-shaped) in school-aged children with ADHD. Because the number of girls was rather small in that study, we did not address sex aspects. In summary, so far very little is known about sex-specific treatment effects of MPH on cognitive functions. Thus, the aim of the present study was to compare dose-dependent effects of MPH on attentional processes between boys and girls with ADHD. As in our previous study (Konrad et al. 2004), we ran a double-blind, placebo-controlled trial with a relatively low single dose of MPH (0.25 mg/kg body weight), a relatively high dose (0.5 mg/kg body weight) of MPH, and a placebo mimicking the typically prescribed single doses (which are administered twice to three times a day resulting in a daily dose about 0.8–1 mg/kg body weight). After controlling for co-morbidity and ADHD subtype distribution, we expected that males and females would not differ in their performance on the placebo trial (Biederman et al. 2005; Seidman et al. 2005; Seidman 2006; Wodka et al. 2008). Furthermore, we predicted differential dose effects of MPH across both sex groups (Konrad et al. 2004): The performance of intensity parameters of attention would increase with higher dosage, whereas other aspects would either not change (divided attention), or would show an inverse-U trend (SAS). Most of the available data on sex-related MPH research suggest that there are no differences in side effects or efficacy (Barbaresi et al. 2006; Sonuga-Barke et al. 2007). Therefore, we predicted that dose-dependent effects of MPH on attentional functions would be comparable for boys and girls.
Methods
Participants and selection procedure
A total of 54 children with ADHD, aged 8–12 years, 27 in each sex group, participated in this study. Additionally, data from 20 boys and 9 girls were taken from a study previously published by our lab (Konrad et al. 2004). All children met the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) criteria for ADHD (American Psychiatric Association 1994) and were recruited from our inpatient and outpatient departments of child and adolescent psychiatry. All new referrals with suspected ADHD symptoms underwent an extensive child psychiatric examination conducted by an experienced child and adolescent psychiatrist. Classification according to DSM-IV was based on a German semistructured interview (K-DIPS; Unnewehr et al. 1995) of the parents and the child, developmental history, playroom observation, and pediatric examination. Additionally, the Child Behavior Checklist (CBCL) (Döpfner et al. 1998) was administered to all parents of the children. Only children without a prior history of stimulant treatment or other medication for ADHD were included in the study protocol. Further exclusion criteria were: General intelligence quotient (IQ) below 80 (Wechsler Intelligence Scale for Children-III; WISC-III) (Tewes et al. 1999); any potentially confounding diagnoses, such as psychosis, mania, major depression, substance abuse, pervasive developmental disorders, or receptive language disorders; or any kind of additional medication. The two sex groups were not different with respect to age (t(52) =0.696; p = 0.489), IQ, (t(52) = 1.067; p = 0.291), co-morbidities (χ2 (1) > 0.355; p > 0.379), subtypes of ADHD (χ2 (1) > 0.831; p = 0.362) or number of nonresponders (χ2 (1) > 0.386; p = 0.535). Only 41 (76%) of the CBCLs given to the parents were returned or filled out completely (20 boys and 21 girls). Both groups were equally impaired on the inattention subscale (T score > 70; see Table 1) and did not differ significantly from each other with respect to the other CBCL subscales. Informed parental consent was obtained for all participants, and the study was approved by the Medical Ethical Committee of the University Hospital of Aachen. In addition, all children themselves gave their assent for participation. Table 1 summarizes the major clinical and demographic data.
Abbreviations: ADHD = Attention-deficit/hyperactivity disorder; ADHD-C = combined subtype; ADHD-IA = inattentive only subtype; DBD =disruptive behavior disorder (conduct disorder or oppositional defiant disorder according to DSM-IV criteria); WISC-III = Wechsler Intelligence Scale for Children-Third Edition; CBCL = Child Behavior Check List (T-Scores).
Medication protocol
A double-blind, placebo-controlled, mixed-factorial crossover design was used in which every child received a placebo, a low dose of MPH (0.25 mg/kg), and a high dose (0.5 mg/kg) on two occasions across a 6-day period. The active medication and placebo were prepared by a physician who was not involved in the assessment. All capsules were identical opaque gelatin capsules and were administered in a double-blind manner. Capsules containing placebo (lactose) and 0.25 mg/kg and 0.5 mg/kg doses of MPH were prepared for each subject. The dosage (to the nearest 2.5 mg), was based on the child's weight although there is no evidence that gross body weight is predictive of response to MPH (Rapport and Denney 1997). The mean dosage for the 0.25 mg/kg condition was 9.6 mg (±2.4 mg) for the boys and 9.6 mg (±2.2 mg) for the girls (t(52) = 0.015; p = 0.980). Moreover, the mean dosage for the 0.5 mg/kg condition was 19.4 mg (±4.9 mg) for the boys and 19.4 mg (±4.3 mg) for the girls (t(52) = 0.037; p = 0.971). The two doses were chosen based on the fact that in clinical practice children are normally administered doses of 0.5–1 mg/kg MPH each day, given on two or three occasions a day. Prior to testing, all the children were given 0.3 mg/kg MPH each day for at least 1 week to ascertain tolerance. Within the 6-day protocol, the order of drug conditions was randomized, with the restriction that higher doses should never be administered after the placebo. Thus, there were 11 possible orders for the 6-day procedure as a whole, and 6 possible orders for the sequence of the 3 neuropsychological assessments. Children were assigned in equal numbers to each of the 6 orders.
Medication was administered once a day between 7 and 8 a.m.; cognitive testing began 60 minutes after medication and lasted between 50 and 70 minutes. On each test, three parallel versions of the computerized attentional tasks (de Sonneville 2000) were used, and the order of the tasks was balanced to reduce learning and fatigue effects. MPH response was defined on the bases of behavioral ratings obtained by the parents and/or by teachers during the drug onset phase.
A model-oriented approach for assessing attentional processes
Concepts of attention generally distinguish between selectivity and intensity of attention. Selectivity refers to the process that modulates responsiveness to specific stimuli constellations by giving priority to certain stimuli, whereas intensity describes the ability to activate and maintain attention over time. In addition to selectivity and intensity components of attention, a SAS is assumed to act as a control mechanism, modulating both selectivity and intensity (Van Zomeren and Brouwer 1994). Figure 1 presents such a theoretical framework and possible paradigms for assessing these attentional functions. Although this conceptualization has also been criticized for its lack of specification, it nevertheless allows a classification of paradigms and is also supported by clinical studies (Spikman et al. 2001) as well as by functional imaging data (Cabeza and Nyberg 2000).
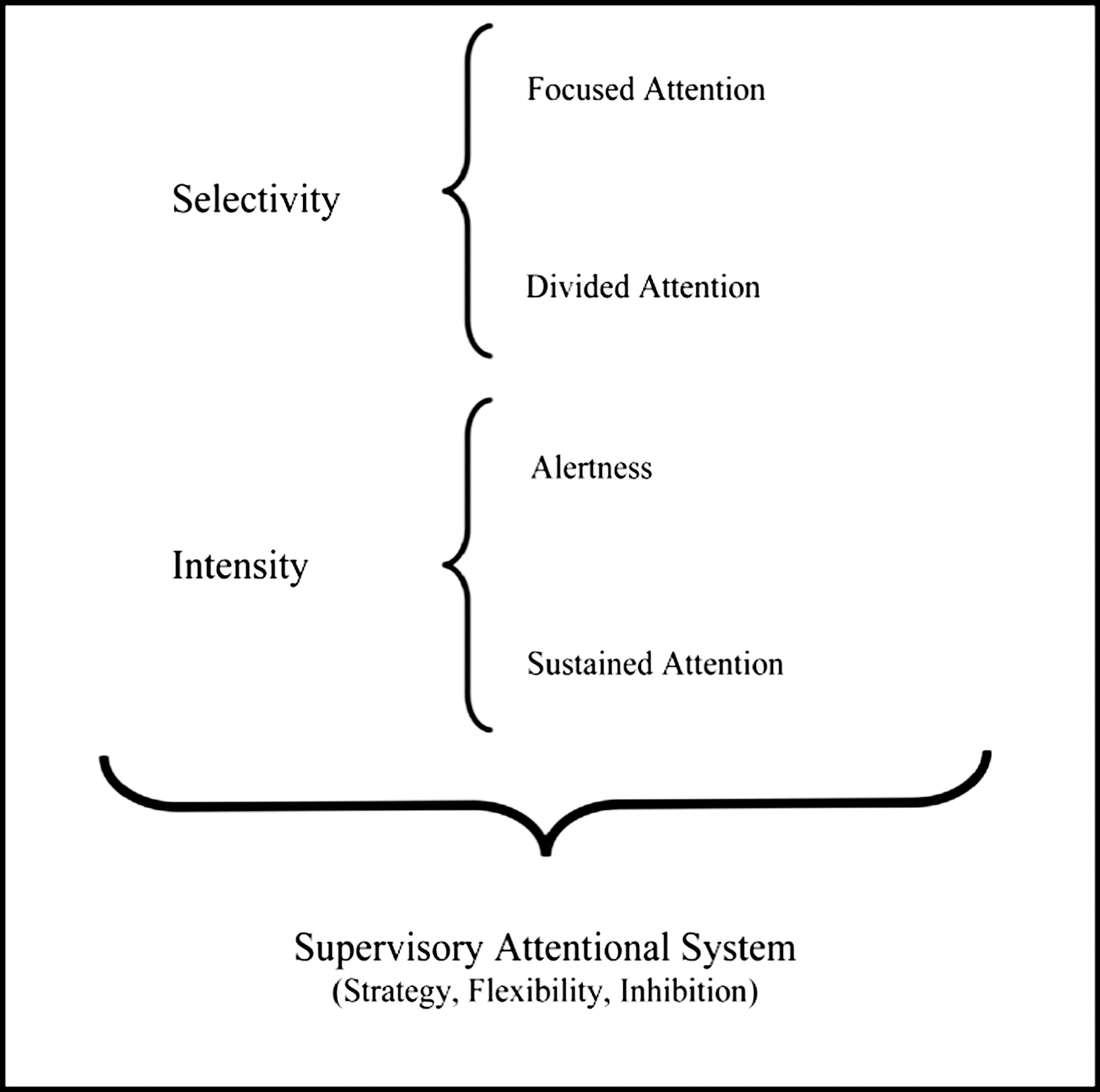
A schedule of the theoretical framework of attentional functions according to Van Zomeren and Brouwer (1994).
Experimental procedure
Baseline speed was assessed with a simple reaction time (RT) task (de Sonneville 2000). The child had to respond with his/her dominant hand to stimulus presence within 32 trials. The dependent measures were the median and the within-subject standard deviation (SD) of the RT.
Sustained attention involved the continuous and consecutive presentation of 50 series of 12 different dot patterns (600 signals; de Sonneville 2000). In each series, an equal number of three-, four-, or five-dot patterns were presented in a pseudorandom manner. The child was instructed to push the “yes” button with the index finger of the dominant hand whenever a four-dot pattern (target) was presented and to press the “no” button with the index finger of the nondominant hand if the presented pattern contained three or five dots (nontargets). Two types of correct responses were counted: Hits on four dots and correct rejections of three- and five-dot patterns. Two types of errors were registered: Misses (Mis) and false alarms (FA). As an index of speed (RT), the sum score of the 12 latencies was calculated. The standard deviation of the sum scores across 50 series was taken as a measure of fluctuation in speed during task performance (SD).
In the focused attention task, four letters were presented simultaneously, and the child was instructed to respond with the “yes“ key to one target letter, but only if this appeared on one of the relevant diagonal positions (de Sonneville 2000). The child was told to reject any other signal (“no” response). The dependent measures were RT, SD, Mis, and FA.
Divided attention was a test that combined an optic and acoustic discrimination task (Fimm and Zimmermann 2001). Children were asked to respond as quickly as they could whenever a square appeared and also if an alternating high and deep tone was repeated. The dependent measures were RT, SD, Mis, and FA.
The visual set-shifting task consisted of three parts (de Sonneville 2000). The signal was a bar with a colored square. The square was liable to jump from left to right and vice versa. Depending on the color of the square after the jump, the child had to copy the movement (part 1) or was required to mirror the movement of the square (i.e., press the left key in response to a rightward movement or the right key after a leftward one; part 2). In part 3, the square was liable to change color at any moment, at which time the child had to adjust his/her responding behavior. Parts 1 and 2 consisted of 40 trials each, and part 3 had 80 trials. The dependent measures were the total number of errors (ER) as well as the mean RT and SD of the congruent and incongruent trials of part 3.
Statistical analysis
Data were analyzed using SPSS 16. The demographic and clinical characteristics were assessed by an independent t-test (IQ, age, and CBCL scores) and chi-squared–Pearson (ADHD subtype, number of nonresponders, and co-morbidity). Repeated measure group differences were evaluated using repeated measure analysis of variance (ANOVA), with sex (female and male) as independent variable, drug dosage (placebo, 0.25 mg, 0.5 mg) as the within-subject factor, and the neuropsychological scores on the five attention tasks as dependent variables. Furthermore, partial eta-squared (pη2) was calculated to measure effect size (0.01 = small effect, 0.06 = medium, >0.14 = large). Only children with no missing data were included in the study. In the case of significant F-values, post hoc comparisons and trend tests were performed to establish the presence of a linear or quadratic relationship. It was decided not to adjust for multiple testing to avoid Type II errors and also to detect mild differences on a more liberal level (Tabachnick and Fidell 2000).
Results
Differences between males and females
In total, we examined 17 neuropsychological variables. Among four of these dependent measures, differences between males and females could be detected. The boys had significantly faster reaction times on the sustained attention task (F(1,52) = 4.42; p = 0.040; pη2 = 0.078) and lower SD values on the focused attention (F(1,52) = 1.97; p = 0.001; pη2 = 0.187) and divided attention tasks (F(1,52) = 7.4; p = 0.009; pη2 = 0.125). Furthermore, the boys had significantly more Mis in the sustained attention task (F(1,52) = 6.79; p = 0.012; pη2 = 0.115). All differences had medium-to-high effect sizes (pη2 > 0.06; for all details of the results see Table 2).
Linear effect.
Low Dose is Enough.
High Dose is Necessary.
Inverse U-Shaped.
Abbreviations: MPH = Methylphenidate; M = male; F = female; RT = reaction time (milliseconds or seconds [for sustained attention]); SD = standard deviation; FA = number of false alarms; Mis = number of misses; ER = number of total errors.
Effect of MPH
Significant improvement under medication could be detected for the SD of baseline speed (F(2,104) = 7.87; p = 0.001; pη2 = 0.132) and the RT (F(2,104) = 9.21; p = 0.001; pη2 = 0.15) and SD (F(2,104) = 4.06; p = 0.02; pη2 = 0.072) of the focused attention task. Furthermore, the SD (F(2,104) = 5.28; p = 0.007; pη2 = 0.092), Mis (F(2,104) = 23.56; p < 0.001; pη2 = 0.312), and FA (F(2,104) = 3.51; p = 0.033; pη2 = 0.063) of the sustained attention task showed significant improvement. The largest effects were detected for the RTs (F(2,104) = 14.19; p < 0.001; pη2 = 0.214) and SDs (F(2,104) = 35.07; p < 0.001; pη2 = 0.403) of the set shifting task. No effects could be detected for the divided attention paradigm (F(2,104) < 1.88; p < 0.157). Except for the number of Mis and FA in the sustained attentions task, significant effects were primarily detected for RT and SD of the tasks.
Post hoc analyses and trend tests revealed four differential dose–response effects for several parameters (see Fig. 2 for more details). The trend tests for the first two effects (Low Dose Enough and High Dose is Necessary) were significant for linear and quadratic effects (shown in Fig. 2A). For the SD of the sustained attention task, significant differences were found between the placebo and the low-dose condition and between the placebo and the high-dose condition. However, there were no significant differences between the low and the high doses in this task. Thus, higher doses did not further improve the performance (Low Dose is Enough). Most of the effects showed no significant difference between the placebo and low-dose condition and a significant improvement on the high-dose condition (High Dose is Necessary). This was found for the SD value of the focused attention task, the FA of the sustained attention task, and for RTs of the set-shifting paradigm. The SD of baseline speed and Mis of the sustained attention task showed a linear dose–response with significantly better performance in the high-dose condition compared to the low-dose condition (Linear). In addition, two parameters showed a significant difference between the low-dose and high-dose condition, but performance was found to be worse in the high-dose condition (Inverse U-shaped). This inverse U-shaped pattern could be detected for RT of the focused attention task and for the SDs of the set-shifting paradigm.
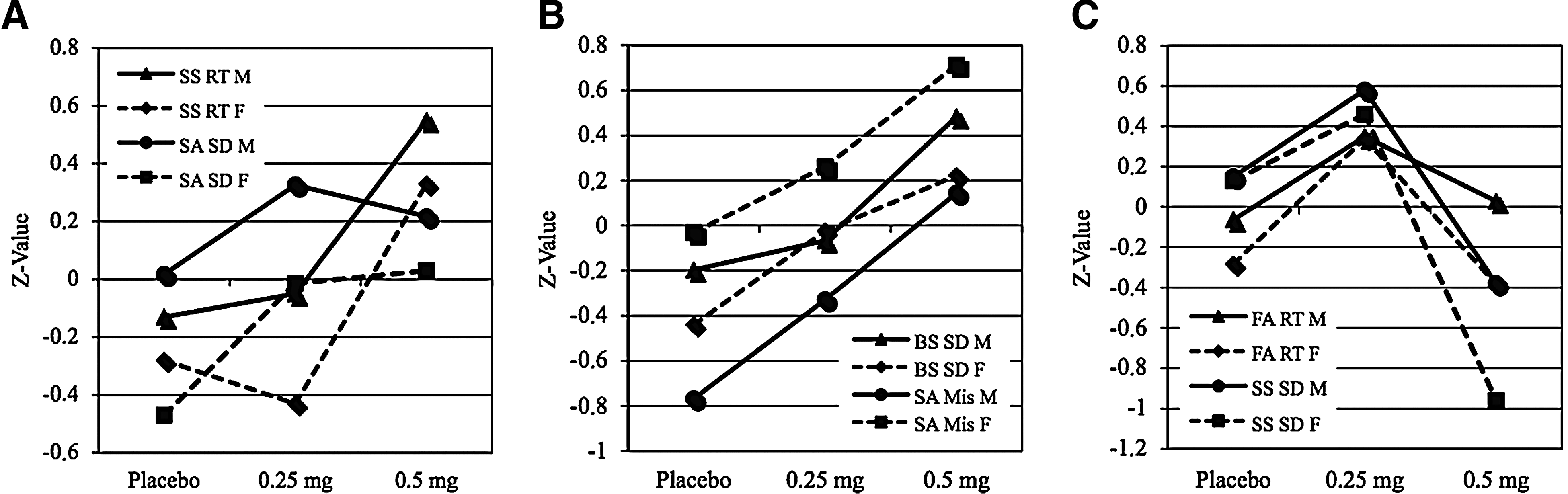
Dissociation of dose-related effects across different measures of attentional domains of functioning. (
Impact of sex on the effect of MPH
No significant interaction between sex and effect of medication could be detected within the different neuropsychological parameters. However, two trends or marginal interaction effects (p < 0.10) were detected for SD of the focused attention task (F(2,104) = 2.98; p = 0.061) and RT of the divided attention task (F(2,104) = 2.69; p = 0.073). On both parameters the performance of the boys increased (“Linear” for focused attention and “Low Dose is Enough” for divided attention), whereas the performance of the girls did not change or worsen. None of these effects could be explained by a ceiling or floor effect found only amongst males or only amongst females.
Discussion
The aim of our study was to examine the dose-dependent influence of MPH on attention in relation to sex. Furthermore, we wanted to investigate whether boys and girls with ADHD in a clinical sample differ in their attentional functions when they were matched for age, IQ, ADHD symptom severity, co-morbidity patterns, and ADHD subtype. Therefore, we compared 27 males and 27 females with ADHD in a double-blind, placebo-controlled trial on five different attention tests with a low dose of MPH, a high dose of MPH and placebo.
Sex differences
In contrast to our expectations, we detected sex-related differences on attentional functions. The boys had significantly faster reaction times (sustained attention task), but had lower standard deviations of RTs (focused and divided) and made more errors (sustained attention). This replicated the findings of Newcorn and colleagues (2001) that girls with ADHD are less impulsive than boys with ADHD. They interpreted the faster RT on their Continuous Performance Test (CPT) as a measure of impulsivity, leading to a higher number of errors. In contrast, the girls in our study had higher SDs on two of the five tasks. This is in accordance with earlier research, wherein girls from clinical samples are supposed to be more impaired than boys with ADHD (Carlson et al. 1997). Other studies however, which assessed several neurocognitive parameters, concluded that there are no differences on neuropsychological tasks between boys and girls with ADHD. For example, Seidman et al. (2005) compared 103 boys with ADHD with 101 girls with ADHD in an age range of 9–17 years on different neuropsychological tests. Seventeen dependent variables from five tests were examined (Wisconsin Card Sorting Test, Stroop, California Verbal Learning test, and Rey Osterreith Complex Figure task, and an auditory CPT), but only two significant differences could be detected, suggesting that males and females with ADHD have comparable neuropsychological deficits. However, only one attention test was included, and the mean age of the whole sample (13.5 for the boys and 12.5 for the girls) was not comparable with our study. We detected a difference between boys and girls on four (23%) of our attention variables, and the effects were medium to large. Because there is no evidence that the average effect size for sex differences differs from the average effect size found in other domains of neuroscience, we conclude that boys with ADHD in the age range of 8–12 years are more impulsive than girls on a sustained attention task, whereas girls with ADHD have significantly higher SDs on tasks measuring selective attention. Besides, this is the first study that compared different attention tasks in relation to sex for children with ADHD. It is noteworthy that the results should be replicated in an independent nonclinical epidemiological sample.
Differential effects of medication
Across both sexes, we predicted differential MPH dose effects on attentional performance parameters. We were able to replicate our previous findings (Konrad et al. 2004) in an extended sample. Improvement of performance due to MPH medication could be detected in four of the five attention tasks. Only the results of the divided attention task, a part of selectivity of attention, did not improve. All other tasks improved; however, the dose-dependent effects differed as a function of attentional functions. Two groups of attentional parameters responding to different doses could be summarized that are important for clinical practice. The first group consists of three effects, whereby only an improvement or no change of the attentional function could be detected. Some of the parameters improved linearly, whereas SD of the sustained attention did not improve after high dosage as compared to low dosage. Only for sustained attention (SD) a low dose of MPH was enough, whereas a proper linear effect was found for baseline speed (Alertness) and for one of the error parameters of the sustained attention task. Furthermore, the improvement of three variables was not appreciable between the placebo and low-dose condition, but with the high dose of MPH the results were significantly better. The second pattern of response to medication could best be described with the inverse U-shaped pattern. The RT of the focused attention task and the SD of the set-shifting paradigm increased significantly on low dose, whereas the performance decreased significantly with a higher dosage. Due to the significant decrease of the performance in the high-dose condition, the second group must be clinically differentiated from the first one. Compared with the study of Konrad and colleagues (2004), we replicated the finding for girls that the intensity parts of attention (alertness and sustained attention) could be better described by group 1. Moreover, executive functioning (set shifting) and more complex attention parameters are more sensible to the inverse U-shaped pattern (Tannock et al. 1995; Sprague and Sleator 1977; Konrad et al. 2004). Altogether, our results are in agreement with previous findings that conclude that MPH treatment increases different attention parameters (e.g., Epstein et al. 2006; Tucha et al. 2006).
More interesting and in agreement with other studies (Barbaresi et al. 2006), no significant differences could be detected between girls and boys with ADHD in relation to the efficacy of MPH. Only two marginal interaction effects between treatment and sex could be detected (p < 0.1). On both parameters, a trend was detected—boys profited from MPH whereas girls did not. Most of the MPH effects, however, were identical between boys and girls (see Fig. 2). This is in line with practice guidelines (e.g., American Academy of Child and Adolescent Psychiatry 2002; Rushton et al. 2004; Taylor et al. 2004), wherein no differences are made in the treatment of boys and girls with ADHD. Note, however, that in our study the two sex groups were comparable in subtype distribution, co-morbidities, and behavioral problems (see outcomes of the CBCL measures). As stated in the introduction, boys and girls could differ in relation to these factors. Thus, due to different subtypes and/or co-morbidities, differences in psychosocial treatment could be necessary (Rucklidge 2008) and differences in MPH efficacy could be expected (Polanczyk 2008).
Limitations
This study has several limitations. First, our sample was clinically referred. Due to a later referral and diagnosis of ADHD in girls (Abikoff et al. 2002) and a higher probability for male sex to be treated with stimluants (Charach et al. 2006; Miller et al. 2008), it is possible that findings in a nonreferred sample would be different. One could speculate that only severely impaired girls are referred to child and adolescent psychiatry and treated with MPH. Thus, girls with ADHD may be less impaired on different aspects of attention in a nonreferred sample. Therefore, the generalization of our results to the ADHD population in general is limited. Second, we did not consider systematic pubertal development or pubertal hormones (such as steroid levels). This could be an important confounder for the assessment of attentional functions in girls during their menstrual cycle. Interaction between hormones and stimulant medication is an unaddressed question. Only two studies to date have looked at the effects of hormonal changes on the response to amphetamine during the menstrual cycle (Justice and de Wit 1999; Justice and de Wit 2000). Preliminary findings suggest that the effect of amphetamine partly depends on hormone levels. Thus, when comparing the efficacy of MPH between boys and girls, it seems essential to control for hormonal fluctuations, especially if examined in postpubertal adolescent and adult females. However, due to the inclusion of subjects in the age range 8–12 years in our study (mean age = 11.05), we regard the effect of this possible confounder as minor. Finally, we could not detect sex differences or sex-by-MPH interactions on most of our behavioral attention tests. Therefore, we assumed that both sexes are identical on these measurements. However, numerous studies report no behavioral differences, whereas neural activity seems to be different between males and females (e.g., Piefke et al. 2005; Jacobsen et al. 2007; Koch et al. 2007). For example, Jacobson and colleagues' (2007) examination of sex-related differences in visual and auditory attention as a function of prenatal exposure to maternal tobacco use revealed that in some of the attention variables the behavioral performance did not differ between the sexes. However, significant differences were detected in activated brain regions between females and males.
Conclusion
Due to the detected sex differences in attentional performance, the target for intervention might be different for boys and girls. For example, based on a neuropsychological assessment of different aspects of attention, the treatment focus for girls might be to optimize selectivity aspects for attention, whereas the focus for boys with ADHD could be, for instance, to decrease impulsivity. Thus, depending on the predominant attention deficit of a child, different doses might be necessary to improve attentional functions. Furthermore, the sex-independent differential dose effects of MPH on attentional functions suggest that typical clinical practices for determining the response to stimulant treatment from a single measure, such as a behavioral rating scales or a single attention task, might be insufficient. However, both sex groups profit in the same way, and no differences could be detected in MPH efficacy between boys and girls with ADHD. It is important to note that our results are based on group means. Clinically, it is important to measure at the individual level to detect best-dose responses. Nevertheless, sex matters for neuroscience (Cahill 2006) and future studies should not only include sex as a confounding variable but include sex as a main research factor.
Footnotes
Disclosures
Dr. Günther has received speeking fees from Novartis and Eli Lilly. Dr. Konrad has received speeking fees from Eli Lilly, Novartis, and Medice. Dr. Herpertz-Dahlmann is a consultant to Eli Lilly and has received industry research funding from AstraZeneca, Eli Lilly, Novartis, and Janssen Cilag.
This research was funded by the German Society for the Advancement of Scientific Research (DFG grant KFO112).