
Abstract
Attention-deficit/hyperactivity disorder (ADHD) is a common neurobehavioral disorder that affects children worldwide. The etiology of ADHD is complex and not fully understood. Earlier studies associated elevated levels of manganese (Mn) with learning problems, attention deficits, and ADHD. Furthermore, it has also been shown that the dopamine (DA) system, the primary site of action of pharmacological ADHD treatments, is influenced by high levels of Mn. Recent studies have suggested that Mn accumulates in dopaminergic neurons via the presynaptic dopamine transporter (DAT). A role for altered functioning of the dopaminergic system in the etiology of ADHD has been well established through neurochemical, neurophysiological, imaging, and genetics studies. Methylphenidate (MPH) is a psychostimulant commonly used to manage ADHD symptoms. The pharmacotherapeutic effect of MPH occurs primarily through its action of inhibiting DAT, and thus increasing dopamine, as well as other catecholamines, at the synapse. We assessed a group of children with ADHD and matched control children without psychopathology attending public schools in a southern Brazilian city and reported elevated serum concentrations of Mn in treatment-naïve children with ADHD compared to normal controls. Interestingly, children with ADHD receiving concurrent MPH showed no difference in Mn serum levels versus controls. We then prospectively assessed the impact of naturalistic treatment with MPH and determined that Mn concentrations were significantly reduced from baseline values following MPH exposure.
Introduction
Although the etiology of ADHD is still unknown, several lines of evidence based on neurochemical, imaging, and genetic studies point toward dysregulation of catecholaminergic systems in ADHD (Biederman 2005). Neurochemical studies have shown that stimulant medications such as methylphenidate (MPH) used for treatment of ADHD block the dopamine transporter (DAT) and also enhance dopamine (DA) and norepinephrine release (Segal and Kuczenski 1997; Kuczenski and Segal 2002). Positron emission tomography (PET) studies have also shown that therapeutic oral doses of MPH bind with strong affinity to the DAT (Volkow et al. 2002).
ADHD is highly heritable with estimates in the range of ≈60%–90% (Levy et al. 1997; Smalley 1997; Thapar et al. 1999; Faraone and Doyle 2001). Genetic studies have yielded mixed results using both candidate gene analyses as well as linkage and genome-wide association studies, with the majority of risk still unexplained. Despite possible variations in sample size and diagnostic criteria used, the extant evidence suggests that other factors also may play a role in the development of ADHD symptomatology, including environmental risk factors. Some research points to a possible role of heavy metals, such as lead, in ADHD (Nigg et al. 2008).
Manganese (Mn), a transition metal and an essential mineral, is neurotoxic at high concentrations (Aschner et al. 2007). This element is readily present in the soil, atmosphere, and plants (Cockell et al. 2004). In particular, plants such as soybean and rice are naturally abundant in Mn because they accumulate this ion from the soil. Several studies have associated elevated levels of Mn in children with learning problems and cognitive and attention deficits (Pihl and Parkes 1977; Collipp et al. 1983; Wasserman et al. 2006; Woolf et al. 2002; Wright et al. 2006). Studies using rats and nonhuman primates have shown that the dopaminergic system is particularly vulnerable to elevated Mn (Bird et al. 1984; Tran et al. 2002; Guilarte et al. 2006). Studies in rodents showed that Mn exposure reduced DA levels in the striatum; this finding was also correlated with neurocognitive deficits (Tran et al. 2002). Other studies with rhesus monkeys raised on soymilk formula, which is naturally abundant in Mn, suggest that exposure to Mn increases impulsivity, and thus that Mn may negatively influence neurobehavioral development (Golub et al. 2005).
Recent studies have also shown that the DAT is affected by elevated levels of Mn (Anderson et al. 2007; McDougall et al. 2008). Anderson and colleagues (2007) have reported that inhibition of DAT in rats, with a specific inhibitor of this transporter, significantly attenuated the accumulation of Mn after an acute dose of MnCl2.
Therefore, because elevated levels of Mn influence the dopaminergic system and dopaminergic transmission is postulated to be involved in the etiology of ADHD, we hypothesized that Mn might influence symptoms of ADHD via disruption of the dopaminergic system, via interactions DAT as one of its target proteins.
In our initial studies, we set out to investigate the interplay of environmental risk factors in the development of ADHD in children attending public schools in Curitiba, a southern Brazilian city. We contrasted Mn levels in a group of children with ADHD and control children; subsequently, we explored the hypothesis that treatment with MPH would possibly be associated with changes the levels of Mn in these children with ADHD. We were especially interested in Mn in our populations, given common dietary constituents of soybean, rice, and black bean products, foods with significant Mn concentrations.
Methods
Recruitment and diagnosis
This study was reviewed and approved by our Institutional Review Board.
Participants were recruited from local public schools. Through lectures at local public schools, teachers were encouraged to identify students with suspected learning difficulties, attention problems, and hyperactive behavior; teachers were informed about the availability of research evaluations via referral to our research institute. Parents accompanying their children provided written informed consent. Families entered a multistage, multimethod assessment process to establish diagnostic groups. Child assessment and information on ADHD symptoms at home and school were obtained using the parent and teacher versions of the Swanson, Nolan and Pelham, version IV (SNAP-IV) (Swanson 1995) and the Conners’ questionnaire (Conners 1995) for initial screening. Subsequently, students received thorough medical evaluations that included neurological, ophthalmological, and audiological examinations to rule out perceptual disorders. Assessment of psychiatric disorders was performed using a structured interview, the Computerized Diagnostic Interview Schedule for Children (C-DISC) (Shaffer et al. 2000). The C-DISC is a highly structured interview based on Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) criteria (American Psychiatric Association 1994). Interviews were conducted by highly trained clinical psychologists and were administered to the children and the parent (typically the mother). The Child Behavior Checklist (CBCL), the Teacher's Report Form, and the Youth Self Report (for those above 11 years) (Achenbach 1993) were used to supplement information obtained in the direct interviews, and to determine impact of symptoms in other settings.
Full-scale intelligence quotient (IQ) was measured using the Wechsler Intelligence Scale for Children, 3rd edition (Weschsler 1991), and academic achievement was determined using the Teste de Desempenho Escolar (Stein 1994), developed to primarily measure mathematical, reading, and writing skills in Brazilian children attending the first to fifth grades.
Inclusion criteria for the ADHD group included meeting full DSM-IV criteria for any ADHD subtype, and no concurrent chronic medical disorder. Controls were those who did not meet criteria for any DSM Axis I or Axis II disorder, as well as having no physical conditions such as epilepsy.
Measurement of serum Mn
Between 8:00 and 9:00 AM, fasting venous blood samples were collected by a trained phlebotomist who is a specialist in sampling from children. Each student had ≈4 mL of whole blood drawn into a 5-mL Z trace elements Serum Clot Activator blue-top vacutainer tube. Blood samples were assayed by graphite furnace atomic absorption spectrophotometry (GR Clinical Laboratories, Curitiba, PR) in triplicate. Results that were above the reference value of 3.3 μg/L were reanalyzed. In addition, whole blood iron, magnesium, calcium, and potassium were also analyzed.
Statistical analysis
The two-tailed paired Student t-test was used to assess significance, with p < 0.05 considered statistically significant.
Results
At total of 166 children between the ages of 7 and 15 (9 ± 1.5 years) were enrolled and screened for the study. Of those, a total of 106 children were identified who met full DSM-IV criteria for ADHD. A subset of 74 children met the diagnostic criteria for ADHD and were not taking any medication at the time of initial assessment were prescribed MPH (10–20 mg qd [once a day], immediate release), and reassessed after treatment. The clinical and demographic characteristics for the different groups are presented in Table 1. There were no significant group differences in age. As expected, most children in our sample were males (84% males vs. 16% females). The IQs among the groups did not differ significantly between subjects with ADHD versus controls.
m: Children who were already taking medication (MPH) for ADHD at the time of the evaluations and blood sample analysis.
Controls were defined as those without any DSM Axis I or Axis II psychophathology, and those who were without any neurological problems such as epilepsy or other brain disorders.
p < 0.05.
p < 0.001.
Abbreviations: ADHD = Attention-deficit/hyperactivity disorder; ADHD-C = ADHD-combined type; ADHD-I = ADHD-inattentive type; WISC-III = Wechsler Intelligence Scale for Children, 3rd edition; IQ = intelligence quotient; CBCL = Child Behavior Checklist; Mn = manganese.
Children who met the diagnostic criteria for ADHD and who were not currently taking any medications had Mn levels significantly higher than those of controls (p < 0.001). Interestingly, children with a history of current stimulant treatment for ADHD were noted to have lower Mn serum levels than untreated ADHD children (p < 0.05). Mn levels were higher in children with ADHD predominantly inattentive; however, this difference was not statistically significant (p = 0.65). No differences were noted in whole blood iron, magnesium, calcium, and potassium between groups.
To explore the hypothesis that MPH was associated with reductions of Mn levels in children diagnosed with ADHD, 74 children meeting the diagnostic criteria for ADHD (n = 50 ADHD predominantly combined, and n = 24 predominantly inattentive) were openly prescribed MPH (10–20 mg qd, immediate release). Mn levels were measured after 5–6 months of treatment.
Of the 74 children who were prescribed MPH, only 30 actually took the medication regularly as prescribed. The main reason for lack of compliance with the treatment given by parents was economic. Treatment with MPH was associated with significantly reduced serum Mn versus pretreatment levels (Fig. 1).
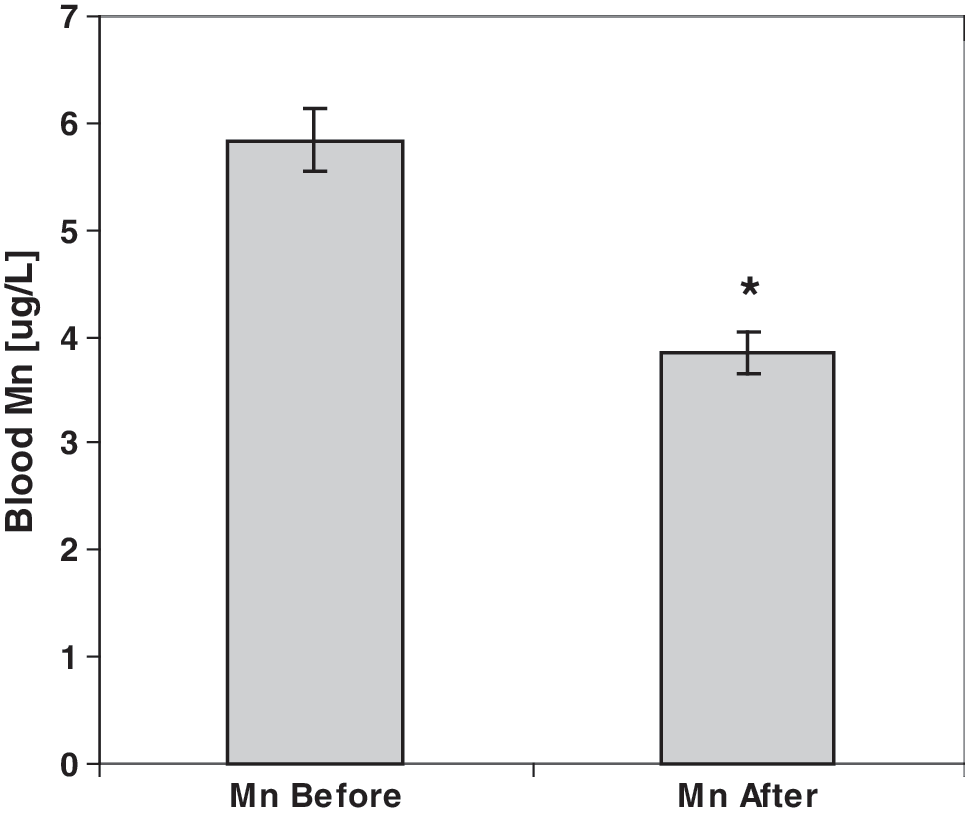
Serum levels of Mn in children diagnosed with ADHD before and after 5–6 months of treatment compliance with MPH (10–20 mg qd, immediate release). (*) p < 0.001. Mn = Manganese; ADHD = attention-deficit/hyperactivity disorder; MPH = methylphenidate; qd = once a day.
Discussion
The presently reported data contain two primary findings of note. First, treatment-naïve subjects with ADHD were found to have higher Mn levels than controls. Second, as shown in Fig. 1, following open treatment with MPH of a subsample of subjects with ADHD, Mn levels were noted to fall after several months of treatment (5.84 ± 2.88 vs. 3.58 ± 1.66 μg/L, p < 0.001). Treatment with MPH was associated with Mn levels comparable to levels noted in control subjects and indistinguishable from that in subjects with ADHD who had already been taking MPH (Table 1). The apparent decline in Mn levels from pre- to posttreatment yielded a dimensionless effect size estimate of approximately 1.0, a large effect.
Prior studies have clearly documented neurotoxic effects of substantial Mn exposure, including severe neurological symptoms. The clinical syndrome is referred to as “manganism” and is a parkinsonian syndrome characterized by muscular hypertonia, bradykinesia, rigidity, postural instability, speech disturbances, and muscle tremors (Banta and Markesbery 1977; Bowler et al. 2006; Cersosimo and Koller 2006). Exposure to subtoxic levels of Mn has also been suggested to be associated with learning and attention problems (Pihl and Parkes 1977), hyperactive behavior, and learning problems (Collipp et al. 1983), with neurofunctional alterations characterized by neuromotor and cognitive deficits, and mood changes (Roels et al. 1985; Roels et al. 1987; Iregren 1990; Roels et al. 1992; Lucchini et al. 1995; Mergler and Baldwin 1997). A recent retrospective study performed with exposed workers employed in ferro- and silico-Mn plants in southwest Quebec reported an association between Mn exposure and neuropsychiatric symptoms (Bouchard et al. 2007). Few data are available that provide clear cut-offs for “nontoxic” levels of Mn.
The mechanism by which Mn causes neurotoxicity is not entirely known. Studies have shown that once Mn crosses the blood–brain barrier, either by diffusion or active transport (Rabin et al. 1993), it can be taken up into astrocytes and neurons (Erikson and Aschner 2006). While astrocytic uptake of Mn occurs via the divalent metal ion transporter 1 (DMT1), neuronal uptake of Mn is regulated by transferrin (Suarez and Eriksson 1993) and by the DAT (Chen et al. 2006; Anderson et al. 2007). Once inside neurons, Mn can promote autooxidation of DA, leading to the production of reactive DA quinones (Miller and Brudvig 1990; Shen and Dryhurst 1998). Furthermore, it has been shown that Mn interferes with mitochondrial adenosine triphophate (ATP) biosynthesis (Chen et al. 2001). Although Mn is heterogeneously distributed in the brain, it has a tendency to accumulate in DA-rich cortical and subcortical areas, particularly in the basal ganglia (Dietz et al. 2001; Josephs et al. 2005; Guilarte et al. 2006; Klos et al. 2006; Uchino et al. 2007). Because Mn toxicity produces adverse motor effects that resemble Parkinson's disease, the dopaminergic system has been the focus of intensive research. Of particular interest, studies have indicated that DAT is a substrate for Mn (Ingersoll et al. 1999; Huang et al. 2003; Chen et al. 2006; Uchino et al. 2007). For example, Chen and colleagues (2006) demonstrated that Mn inhibits binding of the cocaine analog [3H]-WIN 35,428 to the DAT with a statistically significant 30% reduction in B max reduction, suggesting that Mn decreases DAT binding site availability. Recent studies have shown that rats exposed to Mn postnatally have persistent declines in DAT protein expression and [3H]dopamine uptake in the striatum and nucleus accumbens (McDougall et al. 2008). Molecular imaging techniques have also provided additional insight into how Mn may cause toxicity. PET studies on cynomolgus macaques chronically exposed to Mn showed a dramatic decrease in the capacity of striatal dopamine release after an amphetamine challenge (Guilarte et al. 2008). However, the majority of the studies have examined the effects of high levels of acute or chronic exposure to Mn (10–150 μg/L); thus, little is known about exposure to lower subtoxic levels (Aschner et al. 2007). The normal blood concentration of Mn has been estimated to be in the range of 0.8 and 2.1 μg/L (Dobson et al. 2004). Here, we showed that subtoxic concentrations of Mn (3.3–6 μg/L), lower than that observed in patients exhibiting parkinsonian symptoms, may be associated with a neurobehavioral disorder.
Limitations
The methods used in this study present a number of limitations. First, it is an open-label design study and therefore lacks several standard features of clinical trials, most notably inclusion of a placebo group and utilization of double-blind analysis. However, a design based on randomization and using a separate placebo group would require a sample size at least twice as large and would expose half of the patients to placebo conditions for 5 months, which may have not be justified or approved by our Ethics Committee on Human Research. Second, the patient compliance level in this study was quite low; only 30 of 76 children actually took the medication regularly as prescribed. This problem could have been attenuated if there were additional funding to provide these low socioeconomic families with the medication. Third, the concentrations of Mn were measured in serum only. Although serum Mn has been shown to be a good indicator of recent exposure (Lu et al. 2005), additional measures, such as Mn presence in hair, could provide an index of chronic exposure. Indeed, elevated Mn hair content has previously been associated with behavioral, cognitive attention deficits in children (Barlow 1983; He et al. 1994; Woolf et al. 2002; Wright et al. 2006). Nonetheless, the present empirical data revealed a statistically significant (p < 0.001) difference in Mn levels between ADHD patients and control subjects. Furthermore, our data showed that children who were already taking MPH had Mn levels indistinguishable from that of controls.
Clinical implications
Despite the caveats mentioned above, these data suggest that further studies of Mn levels in children with ADHD and the effects of MPH are warranted. Clearly such findings should be replicated in a larger, randomized, and double-blind controlled study. Furthermore, our data suggest that in addition to increasing the levels of synaptically available DA by inhibition of DAT reuptake, MPH may also have neuroprotective effects due to prevention of DA autooxidation and disruption of the ATP biosynthetic pathway, a presumed mechanism of Mn neurotoxicity. Furthermore, because neither
We speculate that our observed relationship between ADHD diagnosis and higher Mn levels may be part of an “environmental etiology of dopamine deficits (ADHD)” (Swanson et al. 2007), wherein small but biologically relevant levels of Mn may interfere with maintenance of optimal levels of DA in predisposed subjects. It may also be clinically relevant to prescribe reduced ingestion of Mn-rich food, such as rice and soy-derived products, in children who have a familial predisposition to develop ADHD.
Our observation of a prospective effect of MPH against elevated Mn levels also raises the question of whether one mechanism of MPH's effects may impact behavior via a reduction of Mn's influence on DA release and tone. It will be of interest to assess whether or not the observations presented here may represent an interaction between genetic vulnerability and environmental risk factors, particularly with regard to the effect of Mn on the dopaminergic system.
Disclosures
Mr. Cunha, Ms. Benko, Ms. Costa, and Ms. Farias have no conflicts of interest or financial ties to report. Dr. McCracken has had affiliations within the past 3 years with Janssen Pharmaceutica, Eli Lilly, Abbott, Bristol Myers Squibb, Wyeth, Novartis, Sanofi-Aventis, and Novopharm. Drs. Cordeiro and Farias have not received any funding nor had any affiliations with companies that may represent a conflict of interest in this study.
Footnotes
Acknowledgments
This study was supported by the State of Parana Department of Science and Technology and the State Health Department, Mr. Norbert Gehr, and the UCLA Foundation. We thank social worker Ms. Rosilda Ferreira for her assistance, Curitiba's Secretary of Education Ms. Eleonora Fruet, the public school teachers, the students and their families for participating in the study.