
Abstract
Objective:
The aim of this study was to evaluate the time course and predictors of improvement in health-related quality of life (HRQL) and medication satisfaction in children diagnosed with attention-deficit/hyperactivity disorder (ADHD) and treated with the methylphenidate transdermal system (MTS).
Methods:
Temporal relationships between ADHD symptoms, medication satisfaction, and HRQL measures were examined via latent growth curve, structural path, and growth mixture models.
Results:
Higher levels of medication satisfaction at the end of titration predicted greater increases in family HRQL (p = 0.004) and, to a lesser extent, child HRQL (p = 0.068) throughout the study. At 4 of 6 (p < 0.05) and 5 of 6 (p < 0.10) contemporaneous time points, ADHD symptoms predicted child HRQL. At 2 of 6 (p < 0.05) and 3 of 6 (p < 0.10) contemporaneous time points, ADHD symptoms predicted family HRQL. ADHD did not predict child or family HRQL improvements at subsequent time points. A uniform pattern of change for child HRQL was noted, with most HRQL change following the pattern of symptom change during titration. Three distinct patterns of change were noted for family HRQL.
Conclusions:
In most cases, medication satisfaction, ADHD symptoms, and HRQL improved simultaneously, suggesting that HRQL was not a delayed response to improvement in symptoms. Children showed a uniform pattern of improvement in HRQL that followed symptom change; three distinct patterns of change were found for improvement in family HRQL.
Clinical Trial Registry:
#NCT00151970.
Introduction
The objective of this post hoc study was to examine the temporal relationship between symptoms, HRQL, medication satisfaction, and the time course of improvement of HRQL for the family and child using data gathered during a clinical trial of the methylphenidate (MPH) transdermal system (MTS). MTS is a patch that, when applied to the hip, is designed to release racemic MPH for as long as the patch is worn, bypass first-pass metabolism, minimize MPH plasma level fluctuation, and afford the flexibility to control the drug's duration of effect. The effectiveness and tolerability of MTS have been documented in clinical studies of children and adolescents (Pelham et al. 2005a; Pelham et al. 2005b; McGough et al. 2006; Findling et al. 2008; Wilens et al. 2008; Findling et al. 2009a; Findling et al. 2009b).
At the onset of the post hoc study, we hypothesized that changes in ADHD symptoms would predict future improvements in HRQL. Furthermore, we anticipated that satisfaction with medication would reflect the patient's overall comfort level and response, and as such we hypothesized that medication satisfaction at the end of titration would be a predictor of improvement in HRQL across the study. Last, we hypothesized that most patients would experience a linear, albeit lagged, improvement in HRQL as their symptoms resolved.
Subjects and Methods
Subjects
Subjects aged 6–12 years diagnosed with ADHD by Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision (DSM-IV-TR) criteria (American Psychiatric Association 2000) were eligible for inclusion in the study. Subjects were required to at minimum complete the Basic Test of the Permanent Product Measure of Performance math test assessment and to have a minimum intelligence quotient (IQ) score of 80. Subjects were excluded if they had severe oppositional defiant disorder or conduct disorder. Subjects were also excluded if in the view of the treating clinician they had any other co-morbid diagnoses that would contraindicate MTS treatment or confound efficacy or safety assessments. Subjects with a history of failing to respond to psychostimulant treatment were also excluded. Subjects were not permitted to have taken another investigational product within 30 days of screening or to participate in other research trials involving drug treatment during the course of the study.
Data were collected at eight sites across the United States; the institutional review board at each site approved the study. The subjects agreed to the study and the subjects' parent or legally appointed representatives (hereafter simply referred to as the subjects' parents) provided written consent in accordance with the International Conference on Harmonisation Good Clinical Practice Guideline E6 and applicable regulations.
Study design
A detailed description of the study design has been reported previously (Wilens et al. 2008). In brief, this was a multicenter, randomized, double-blind, three-way crossover study (with a placebo-controlled analog classroom portion) performed to analyze the efficacy, safety, and duration of effect of MTS patches worn for 4 and 6 hours by children diagnosed with ADHD. The study consisted of four experimental phases: Screening and washout (4 weeks); open-label dose optimization (5 weeks); double-blind, three-way crossover (3 weeks); and follow up (1 week).
During the open-label dose-optimization phase, subjects wore MTS patches for 9 hours daily. The dose was increased each week over 5 weeks from the initial dose of 10 mg using 15-, 20-, and 30-mg patches until subjects showed an acceptable response (e.g., at least a 30% reduction ADHD-Rating Scale-IV [ADHD-RS-IV] score and a Clinical Global Impression–Improvement (CGI-I) scale score of 1 or 2, with acceptable side effects). Further dose changes were not permitted after the fourth week of the dose-optimization phase. Subjects who did not reach an optimal dose by week 5 were discontinued from the study.
Subjects who successfully completed the open-label dose-optimization phase were randomized for the double-blind analog classroom phase of the study. Analog classroom sessions (Wigal and Wigal 2006) were conducted on 3 separate days once per week during weeks 6, 7, and 8, during which time subjects received placebo and their optimized MTS dose for 4 and 6 hours in a random order during the session. With the exception of these 3 analog classroom days, subjects remained on their open-label optimized MTS dose with a 9-hour wear time during the rest of the week.
For the HRQL (measured by the disease-specific HRQL instrument ADHD Impact Module-Child [AIM-C]; Landgraf et al. 2002) and parent Medication Satisfaction Survey (MSS) analyses presented herein, the primary study time points of interest were baseline, end of titration (week 5, visit 7), and end of study (week 8, visit 10) when these data were collected.
Study measures
Primary efficacy and safety measures for this MTS classroom study have been reported previously (Wilens et al. 2008). The primary efficacy measure of ADHD symptoms was obtained via clinician-completed ADHD-RS-IV. The ADHD-RS-IV is an 18-item questionnaire based on DSM-IV-TR criteria that assists clinicians in diagnosing ADHD and assessing treatment response. Each item is scored from 0 (no symptoms) to 3 (severe symptoms). Total scale scores range from 0 to 54 (DuPaul et al, 1998). Scores for the ADHD-RS-IV inattentive and hyperactive/impulsive subscales were used in the present analyses.
Two secondary efficacy measures are also relevant to the present study: (1) A measure of child and family HRQL, the AIM-C and (2) parent satisfaction regarding the efficacy and tolerability of MTS assessed with an MSS. The AIM-C has previously been shown to display good psychometric properties, including good item convergent and discriminant validity and excellent reliability (Cronbach α = 0.88 and 0.92 for the child and family HRQL subscales, respectively; Landgraf et al. 2002). The questionnaire consists of two core scales to assess HRQL impact on the child (eight items) and family (ten items). The measure also consists of two multiitem scales to assess medication tension/worry (three items regarding tension and embarrassment in administering and taking ADHD medication, respectively) and missed-dose worry (four items regarding worry about the number of daily doses missed at home or school). In addition, the AIM-C includes 10 clinical treatment questions (including a missed-dose item and five items that address behavioral change and management), a six-item school cooperation scale, nine parent attribute/knowledge items, four economic impact items, and four demographic questions answered by the subject's parent (Landgraf et al. 2002). Only the AIM-C Child and Family Impact scales, used to evaluate child and family HRQL, have been included in this report (see Appendix). For the AIM-C Child Impact scale, caregivers are asked to describe the behavior of their children with ADHD over a 2-week recall period. Caregivers are also asked to respond to a series of general statements to assess the impact of ADHD on themselves and on the family. Thus, based on the item construction, a specific time referent is not warranted for the AIM-C Family Impact scale. The MSS is a nonvalidated 11-question survey designed to assess parent satisfaction with the study medication.
Statistical analysis
Power to detect interrelationships between ADHD symptoms, child and family HRQL, and medication satisfaction was determined using a bivariate correlation model (null hypothesis r = 0.00). To be conservative, sample size estimation was limited to individuals with data at all time points from the parent MTS classroom study (n = 115). Power to detect a medium relationship (r = 0.30, α = 0.05, two-sided) was excellent (0.91). Power to detect a small to medium relationship (r = 0.20) was modest (0.58).
Subjects who received at least one MTS patch application were included in the safety population. AIM-C child and family HRQL, overall medication satisfaction, and moderator analyses of both HRQL and medication satisfaction were conducted using the safety population.
Scores for the AIM-C Child Impact Scale (eight items) and the AIM-C Family Impact Scale (ten items) were computed separately by summing the items within each scale. Raw scores were transformed to a 0–100 continuum, with higher scores indicating greater HRQL. MSS total scores were computed by first recoding reverse-scored items and averaging item scores.
Principal component solution and reliability
Prior to determining the interrelationships between HRQL and ADHD symptoms, a series of principal components analyses were computed for both the AIM-C Child and Family Impact Scales and the MSS. These analyses were undertaken to confirm that the AIM-C Child and Family Impact Scales and the MSS could be considered unidimensional for future structural models. The number of components to retain was determined using the Glorfeld modification of Horn Parallel Analysis (Horn 1965; Glorfeld 1995).
Reliability is a sample-dependent construct and the ability to examine interrelationships is dependent on adequate reliability. Therefore, the reliability of each scale was examined using the Cronbach α to estimate internal consistency reliability.
Temporal interrelationships
Temporal interrelationships between ADHD symptoms, medication satisfaction, and child and family HRQL were examined in two ways. First, a latent growth model was computed that simultaneously modeled baseline (intercept) and changes (slope) in inattentive and hyperactive/impulsive ADHD symptoms and child and family HRQL measures. This model also included end-of-titration medication satisfaction as a covariate predicting changes in HRQL measures. The advantages of using this model over a correlation approach are threefold: (1) The constructs are evaluated simultaneously, (2) the relationships can be estimated accounting for missing data, and (3) the time between each observation is directly modeled rather than assumed to be equidistant.
Second, structural (path) models were computed estimating contemporaneous and cross-lagged relationships between ADHD symptoms, medication satisfaction, and HRQL. Structural path models simultaneously estimate both contemporaneous and lagged correlations across all time points in a single analysis while also accounting for missing data. Furthermore, rather than estimating all possible relationships, the cross-lagged relationships in this model explicitly examined whether ADHD symptom levels predicted HRQL levels contemporaneously or at the subsequent time point (cross-lagged). Fit of the structural model was determined using the χ2 test, the Comparative Fit Index (CFI), and the Tucker–Lewis Index (TLI) (Bollen 1989; Hu and Bentler 1999).
The growth and structural models provide unique, complementary information about the temporal interrelationship between medication satisfaction, ADHD symptoms, and HRQL. The structural model estimates relationships between constructs at each time point and two successive time points, whereas the growth model examines baseline levels and changes in ADHD symptoms and HRQL across the entire study.
Individual differences
To examine individual differences in changes in child and family HRQL from baseline to end of study, a series of growth mixture models examining 1–4 class solutions were computed, separately for child and family HRQL. The Bayesian Information Criterion (BIC) was used to determine which class solution showed the best fit (Yang 2006; Nylund et al. 2007). The BIC evaluates the relative fit of nested and nonnested models accounting for parsimony, with lower values implying better model fit. These models examine whether changes are consistent across individuals or whether subgroups of individuals show unique patterns of change. All structural and growth (mixture) models were computed using Mplus (version 5.0) (Muthén and Muthén 2007).
Results
Subjects
A total of 148 subjects were screened of which 128 were enrolled in the study. The safety population consisted of 127 subjects who received at least one dose of MTS. Within the safety population, 7 subjects discontinued prior to the double-blind randomization phase, 3 subjects were randomized but did not undergo MTS treatment, and 2 subjects did not complete the analog classroom phase of the study, 1 due to an application site reaction and 1 due to an adverse event (AE) (conjunctivitis) resulting in a total of 115 study completers (Fig. 1). The majority of subjects in the safety population analyzed in this post hoc study were white (66.1%) and male (62.2%). The mean (standard deviation, SD) age of these subjects was 8.81 (1.84) years. Co-morbid diagnoses included oppositional defiant disorder (ODD; n = 16, 12.5%), simple phobia (n = 3, 2.3%), enuresis (n = 12, 9.4%), depressive disorder with mild symptoms (n = 1, 0.7%), and trichotillomania (n = 1, 0.7%).

Subject disposition flow chart. BMI = body mass index; PERMP = Permanent Product Measure of Performance; ECG = electrocardiogram; BMI = body mass index; ITT = intent to treat.
Principal component solution and reliability
Results of principal components analyses indicated single-component solutions for both child and family HRQL and MSS measures at each time point when the Glorfeld modification of Horn Parallel Analysis (Horn 1965; Glorfeld 1995) was used as the criterion for determining the presence of additional factors, which is consistent with previous validation work (Landgraf et al. 2002). This indicates that child and family HRQL and medication satisfaction can be considered unitary constructs and were modeled as such in subsequent analyses.
The reliability of HRQL and medication satisfaction measures across each study time point is presented in Table 1. Results indicated good to excellent reliability for the HRQL measures and adequate reliability for the MSS in this sample. The slightly lower level of reliability for medication satisfaction may have been due to restriction of range in this sample because the majority of subjects were very satisfied with MTS treatment.
Abbreviations: AIM-C = ADHD Impact Module-Child; HRQL = Health-related quality of life.
Temporal interrelationships
Growth curve models indicated that higher levels of medication satisfaction at the end of titration predicted greater increases in family HRQL (standardized slope estimate = 0.88, z = 2.87, p = 0.004), and to a lesser extent child HRQL (standardized slope estimate = 0.35 z = 1.83, p = 0.068) throughout the study. Baseline levels of inattentive and hyperactive/impulsive ADHD symptoms did not predict changes in HRQL across the study (largest standardized estimate = 0.20, z = 0.53, p = 0.594). However, decreases in the slope of inattentive and hyperactive/impulsive symptoms from baseline to end of study were significantly related to increases in child and family HRQL from baseline to end of study (smallest standardized estimate = −0.59, smallest z = 1.90, p = 0.057).
The structural (path) model examining contemporaneous and cross-lagged relationships simultaneously is divided into three figures. The first two figures present the prediction of child HRQL (Fig. 2) and family HRQL (Fig. 3) from ADHD symptoms. The remaining figure (Fig. 4) presents the prediction of child and family HRQL from medication satisfaction ratings.
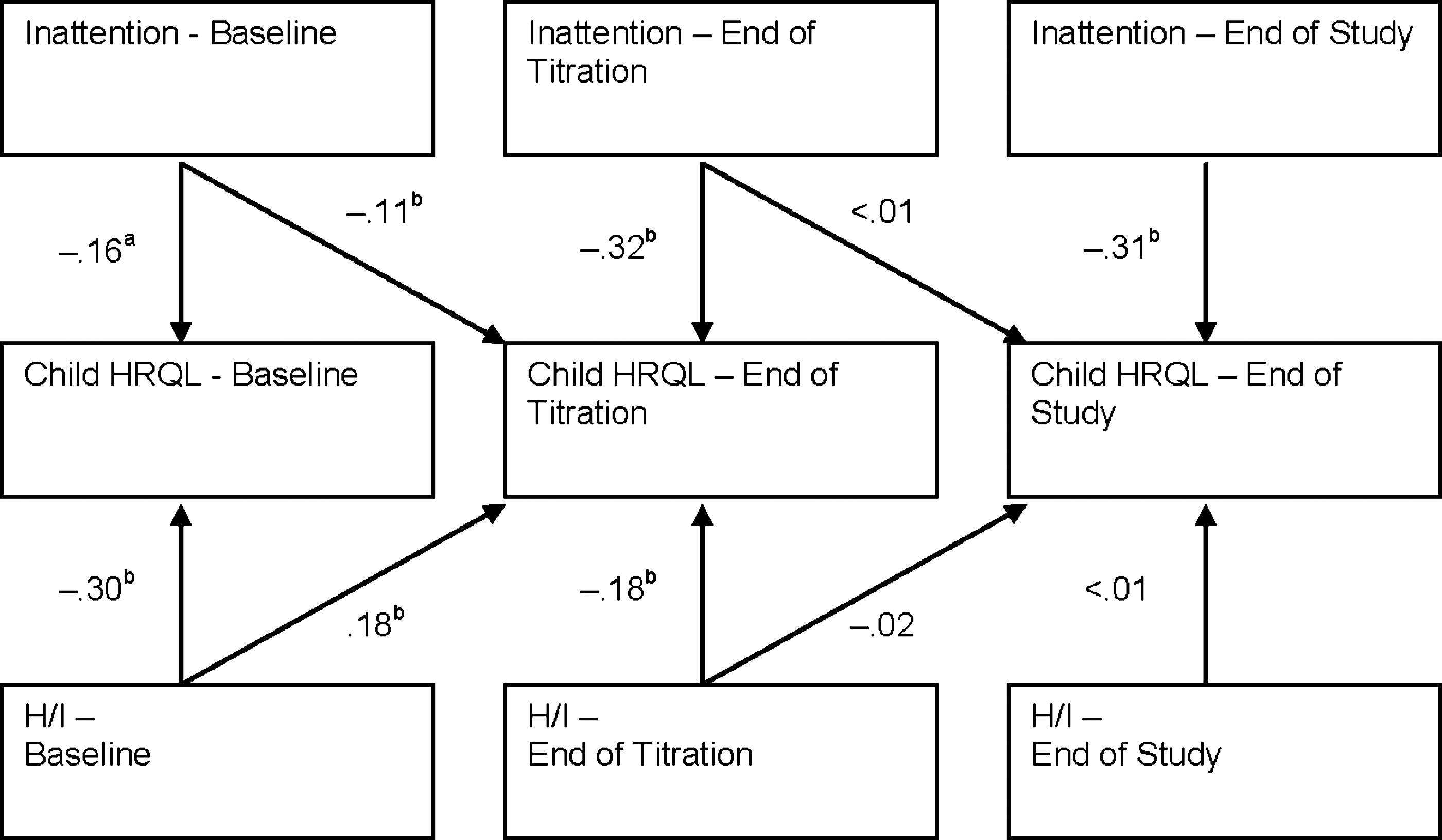
Structural (path) model examining the prediction of child health-related quality of life (HRQL) from attention-deficit/hyperactivity disorder (ADHD) symptoms. (a) 0.05 ≤ p < 0.10; (b) p < 0.05. H/I = hyperactive/impulsive; AIM-C = ADHD Impact Module-Child; HRQL = health-related quality of life.
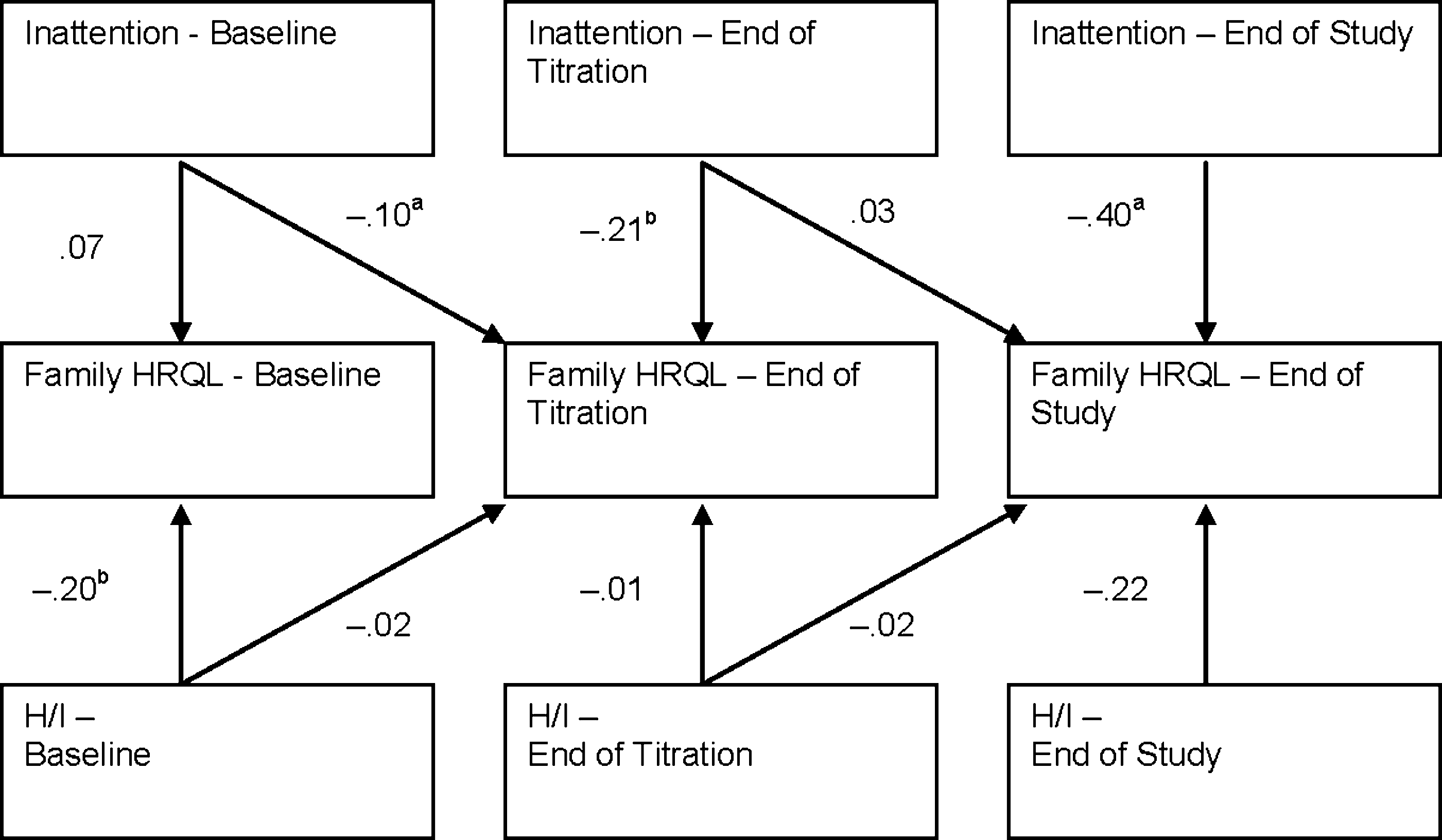
Structural (path) model examining the prediction of ADHD Impact Module-Child (AIM-C) Family health-related quality of life (HRQL) from attention-deficit/hyperactivity disorder (ADHD) symptoms. (a) 0.05 ≤ p < 0.10; (b) p < 0.05. H/I = Hyperactive/Impulsive.
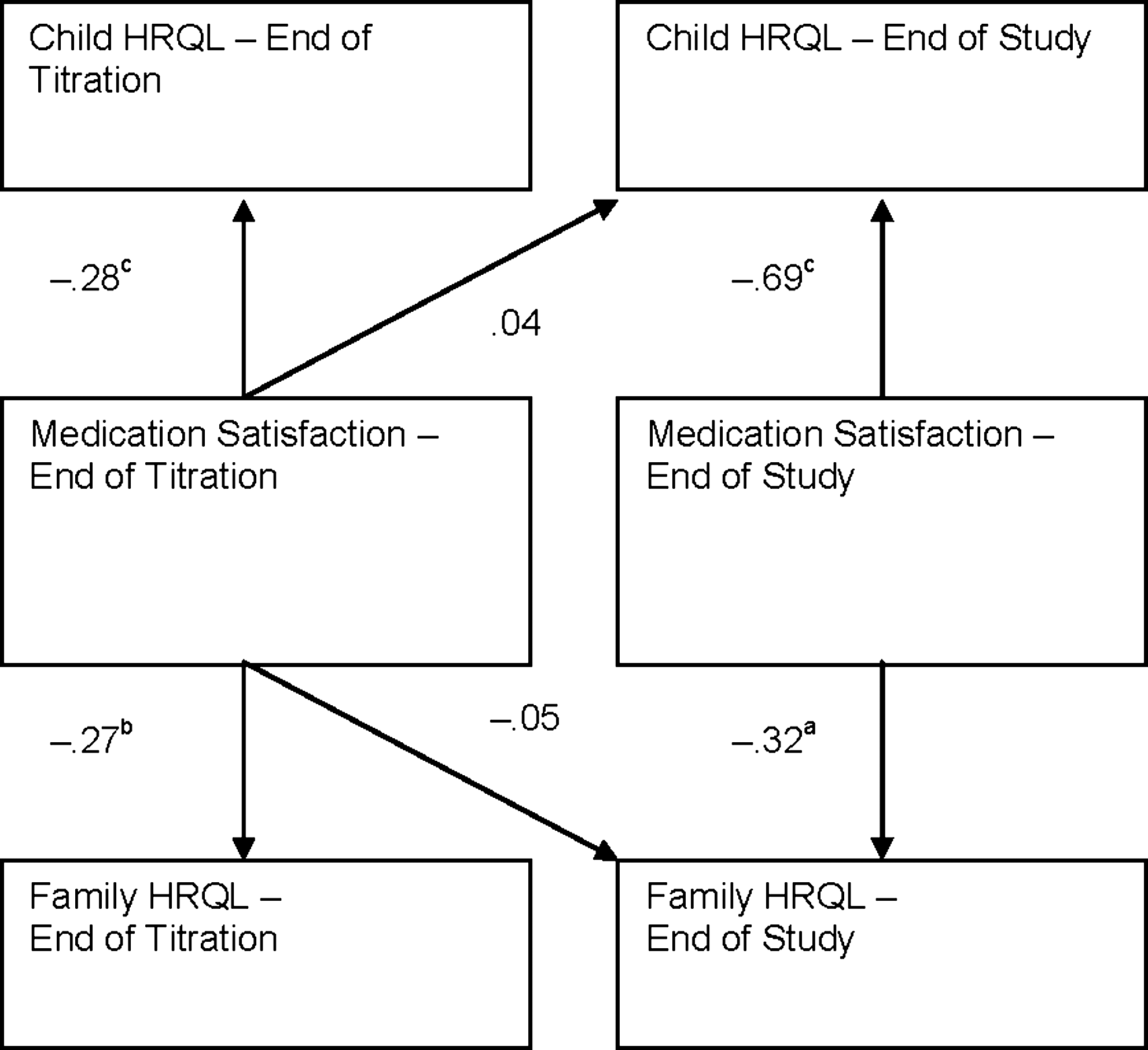
Structural (path) model examining the prediction of ADHD Impact Module-Child (AIM-C) Child and Family health-related quality of life (HRQL) from medication satisfaction. aNot significant due to substantial variability in the estimate; b0.002 ≤ p < 0.05; c p < 0.002.
Results for the structural model indicated excellent model fit (χ2[22] = 32.41, p = 0.071, CFI = 0.97, and TLI = 0.91). Inspection of Fig. 2 reveals that lower symptom ratings predicted higher child HRQL at each time point (all but one of the contemporaneous relationships between ADHD symptoms and child HRQL were at least marginally significant; the smallest standardized path estimate = −0.16, z = 1.91, p = 0.056). The only exception can be seen in the lower half of Fig. 2. The prediction of child HRQL from hyperactive/impulsive symptoms at end of study was not significant (standardized path estimate = 0.002, z = 0.03, p = 0.974).
The lower half of Fig. 2 also contains only one significant cross-lagged relationship between ADHD symptoms and child HRQL; higher levels of baseline hyperactive/impulsive symptoms predicted higher child HRQL at end of titration (standardized path estimate = 0.18, z = 2.35, p = 0.019). This finding is likely due to the fact that individuals with higher baseline hyperactive/impulsive symptoms showed the largest increases in child HRQL from baseline to end of titration. In general, these findings indicated that ADHD symptom levels at a given time point do not drive child HRQL at the subsequent time point.
Inspection of Fig. 3 reveals that, for the prediction of family HRQL from ADHD symptoms, the only significant contemporaneous relationships were the prediction of baseline family HRQL from baseline hyperactive/impulsive symptoms (standardized path estimate = −0.20, z = 2.35, p = 0.019) and the prediction of end of titration family HRQL from end of titration inattentive symptoms (standardized path estimate = −0.21, z = 2.06, p = 0.040). One additional contemporaneous correlation was marginally significant, prediction of family HRQL from inattentive symptoms at end of study (standardized path estimate = −0.40, z = 1.82, p = 0.069). All other contemporaneous relationships involving family HRQL were nonsignificant (largest standardized path estimate = −0.22, z = 1.48, p = 0.139). There was one marginally significant cross-lagged relationship between baseline inattentive symptoms and end-of-titration family HRQL (standardized path estimate =−0.098, z = 1.68, p = 0.093). No other cross-lagged relationships between ADHD symptoms and family HRQL approach significance (largest standardized path estimate = 0.027, z = 0.75, p =0.454).
Inspection of Fig. 4 reveals significant and substantial contemporaneous relationships between medication satisfaction and child and family HRQL at end of titration and end of study (smallest standardized path estimate = −0.27, z = 2.77, p = 0.006). There were no significant cross-lagged predictions of child or family HRQL from medication satisfaction (largest standardized path estimate = −0.05, z = 1.36, p = 0.176).
Individual differences
Growth mixture models evaluated individual differences in the patterns of child and family HRQL scores across study time points. Figure 5 presents child HRQL scores across study time points; a single-class solution fit best (1-class BIC = 2,852, 2-class BIC = 2,859, 3-class BIC = 2,866, 4-class BIC = 2,871). This class showed a steady upward trajectory from baseline to end of study. Figure 6 presents the family HRQL scores; a 3-class solution fit best (1-class BIC = 3,008, 2-class BIC = 2,977, 3-class BIC = 2,971, 4-class BIC = 2,985). The largest class (78.19% of the sample) showed a pattern of large increases in family HRQL scores from baseline to end of titration and the smaller, but continued increases in scores from end of titration to end of study. A smaller proportion of the sample (14.2%) started with moderate levels of family HRQL scores, showed increased family HRQL scores from baseline to end of titration, and then decreased scores from end of titration to end of study. The end point of this group was roughly equivalent to its baseline levels. The smallest class (7.60% of the sample) had very low family HRQL scores at baseline that improved slightly by end of titration and then dramatically by end of study. This group ended with moderate family HRQL scores, considerably higher than its baseline level scores. In this group, changes in family HRQL appear to be lagged relative to improvements in ADHD symptoms, suggesting that symptom improvement may drive family HRQL in this small subgroup.

Changes in ADHD Impact Module-Child (AIM-C) Child health-related quality of life (HRQL) across the study.
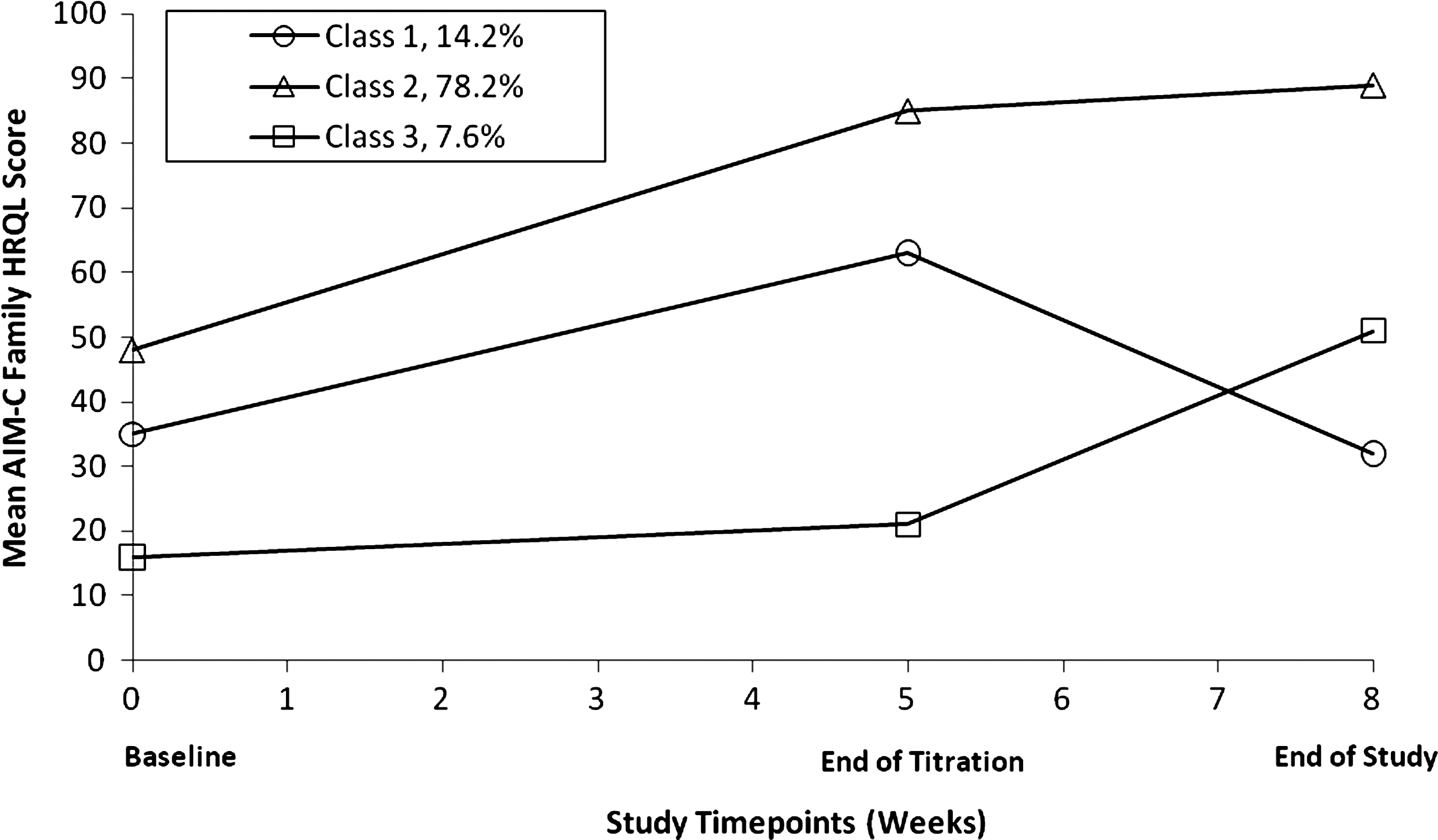
Changes in ADHD Impact Module-Child (AIM-C) Child health-related quality of life (HRQL) scores across the study for three separate classes (subgroups).
Discussion
This report presents a comprehensive analysis of the temporal relationships between three important constructs in the measurement of outcome for ADHD medication treatment: ADHD symptoms, medication satisfaction, and HRQL. This is the first examination, to our knowledge, of the temporal relationships between these constructs in children with ADHD treated with stimulants. Understanding the relationships between ADHD symptoms and HRQL is relevant to characterizing outcomes from ADHD medication treatment and has potential to shed light on the drivers of positive outcomes following medication treatment.
Examination of the relationships between symptoms and HRQL also has implications for clinicians. Alhough symptoms and functioning are examined in the clinic simultaneously, if clinicians identify improvement in medication satisfaction or ADHD symptoms, a lagged relationship may indicate that they could reassure the family of potential later gains to HRQL. Alternatively, if the clinician knows that change in symptoms occurs simultaneously with change in HRQL rather than occurring after a period of delay, then the clinician can evaluate and anticipate changes to HRQL as symptoms decline. Finally, if there are distinct patterns in the time course of improvement of HRQL, clinicians can monitor and identify those patients who may be immediate or delayed responders.
The present study examined the hypothesis that ADHD symptoms would predict later improvements in child and family HRQL. Interestingly, the results indicated that there is little or no lag between improvements in symptoms and changes in HRQL, indicating that symptoms improvement translates contemporaneously into improved HRQL, contrary to our hypothesis. Benefit obtained from improvement in ADHD appears to be felt and reported by the patient at the same visit that symptom change occurs. Temporal resolution of HRQL outcome measures was limited to three time points over the relatively short duration of the study. Future studies including more frequent measurements over longer study duration may help further characterize the relationship between ADHD symptoms and HRQL.
These results are consistent with the findings of a similar study in adults (Weiss et al., in press) in which it was also found that HRQL changed generally with symptom improvement (although obvious variability occurs across families) and that both medication satisfaction and change in symptoms were robust predictors of improved HRQL following treatment with mixed amphetamine salts (extended release). Thus, this temporal relationship between HRQL change and symptom change has now been demonstrated in two ADHD patient populations, adults treated with mixed amphetamine salts, and children with ADHD treated with MTS.
Growth curve models found that medication satisfaction may be an important predictor of HRQL, supporting our second hypothesis. Specifically, medication satisfaction at the end of titration predicted improvements in family HRQL and, to a lesser extent, child HRQL, in the growth models. However, this finding was not supported by cross-lagged relationships in the structural model. The discrepancy in these models indicates that the majority of symptom change occurred between baseline and end of titration. This implies that medication satisfaction is a marker for the parents' views of the success during initiation and titration of medication treatment but may not predict future changes in HRQL. Furthermore, baseline ADHD symptoms were not a significant predictor of change in HRQL, indicating that improvement in symptoms and medication satisfaction following titration, rather than baseline severity of illness, determine whether or not there is a change in HRQL.
The present data also provided a novel look at individual differences in changes in HRQL across medication treatment of ADHD via growth mixture models. Findings suggested that child HRQL generally showed a unitary upward trajectory with individual differences simply varying around this upward trajectory. A substantial proportion of patients (85.79% of the sample) showed substantial increases in family HRQL either during or following medication titration. Interestingly, a small percentage of patients (14.21%) showed a pattern of initial increases followed by declines to baseline levels in family HRQL scores. A review of these patients indicated that they showed smaller changes in symptoms across the study and may have been less satisfied with medication treatment, but the lack of a declining subgroup for child HRQL suggests that other family-specific factors (e.g., such as unrealized or unrealistic expectations for change) may be influencing this subgroup.
It is interesting that, while child HRQL is uniformly better with treatment, family HRQL shows distinct patterns of response. It may be that family HRQL is determined by multiple factors other than improvement in the child's well-being through medication treatment, making this construct a less direct evaluation of medication symptom efficacy, but highly relevant to the overall picture of outcome. Observed differences may also be due to the use of the parent as a proxy reporter for the child impact scale. Some have argued that the proxy report may be unduly biased (Coghill et al. 2009); however, it is not always possible to ask children to self-report, and previous findings have indicated that the AIM-C Child Impact scale is reliable and valid when completed by the caregivers (Landgraf 2002; Manos et al. 2009; Bukstein et al. 2009). Furthermore, differences in the findings may be due to differences in time referencing. The AIM-C Child Impact scale uses a 2-week recall. The AIM-C Family Impact scale asks caregivers to respond to general statements about the impact of the child's ADHD on themselves and the family.
For the clinician, results of the present study indicate that family HRQL may not always correspond with symptom improvement. When improvement in family HRQL does not occur, the clinician needs to follow up to determine the reason why. This lack of improvement may be related to patient treatment or other external factors such as imbedded aversive behavior management practices of parents or to sustained negative impressions of the child due to a history of aversive interactions between the parent and the child.
Future efficacy and effectiveness research will benefit from measuring change in symptoms, medication satisfaction, and HRQL for the family and the child. Although these constructs are fairly closely correlated, they are not identical, and improvement can vary between them. Identifying other determinants of family HRQL besides medication satisfaction may be helpful for further tailoring ADHD treatments to impact the family system. In particular, initiating parent and family support mechanisms may be necessary to further enhance and maintain positive outcomes in terms of family HRQL.
Limitations
This analysis reports AIM-C and MSS data collected during an open-label period of study, thus, subjects and parents were not blinded to MTS treatment and there was no placebo control group for comparison. The AIM-C includes a self-report for family HRQL, which includes parent as well as family items and a proxy report for child HRQL. As with any proxy measure, the observer is inherently influenced by his or her own perception of another's health and well being. Thus, in addition to the use of a placebo group, future studies might include, if possible, child report of their own HRQL.
Subjects who failed to respond to psychostimulants in the past, and those with conduct disorder, were excluded from the study. This likely contributed to the uniform upward trajectory of child HRQL, and these findings may not generalize to other, less strictly defined patient populations. Finally, there may be a significant halo effect when measuring HRQL and medication satisfaction in the context of a clinical trial of a new medication. Further studies of HRQL and medication satisfaction in different contexts are required to learn more about the temporal dynamics of these constructs.
Conclusion
Improvement in ADHD symptoms and medication satisfaction predict improvement in family and child HRQL. This is the first study, however, to demonstrate that while the HRQL of the child improves in a uniform and consistent way, there are multiple patterns of change in family HRQL, including a small minority where deterioration is observed. This suggests that symptom improvement, medication satisfaction, and family HRQL are overlapping but distinct concepts, and that clinicians would do well to distinguish these when the child's symptoms improve to determine if there is actually improvement in the family's HRQL or if other factors are precluding the expected downstream benefits of treatment.
Patient report of satisfaction with medication is as strong a predictor of initial changes in HRQL as symptom improvement. Thus, patient satisfaction with medication is an outcome that has received little attention, but represents an important determinant of the broader picture of treatment response. ADHD symptoms and HRQL change closely in time. The hypothesis and common perception that it takes time for a child's improvement to be reflected in improved well-being, or that improvement must “ripen” to be seen and felt by others is not supported by the evidence. This suggests that quality of life and medication satisfaction can be included in short-term trials, adding an important dimension of outcome complimentary but not identical to improvement in core symptoms.
Footnotes
Disclosures
Dr. Frazier has acted as a consultant/advisor for Shire Pharmaceuticals. Dr. Manos has received research support from Shire Pharmaceuticals, acted as a consultant for Eli Lilly, and has served on speaker's bureaus for Shire US and Veritas Institute for Medical Education. Ms. Landgraf is the vice president and chief scientific officer at HealthActCHQ, Inc., which owns the intellectual property rights to the AIM-C survey. Dr. Weiss has received research support from Eli Lilly, Shire Pharmaceuticals, Purdue, and Janssen; acted as a consult/advisor for Shire Pharmaceuticals, Novartis, Eli Lilly, Janssen, Purdue, Takeda, Abbott, and J&J; and served on speaker's bureaus for Abbott, Eli Lilly, Shire Pharmaceuticals, Novartis, Janssen, Purdue, and Takeda. Dr. Weiss has also received royalties from Checkmate Plus and The Johns Hopkins University Press. Dr. Hodgkins is a full-time employee of Shire Pharmaceuticals and has stock ownership in the company. Dr. Gibbins has received travel reimbursement from Eli Lilly.
Acknowledgments
The authors would like to thank the parents and children who participated in the study. The authors acknowledge Laura Miesle, PharmD, of The JB Ashtin Group, Inc., Plymouth, Michigan, for editorial assistance in the preparation of this manuscript and Shire Development Inc., Wayne, Pennsylvania, for funding this editorial assistance.
Appendix
This study was funded by Shire Development Inc., Wayne, Pennsylvania.
Reproduced with permission from HealthActCHQ Inc., Cambridge, MA. ©Copyright 2001–2006. All rights reserved.
*