
Abstract
Objective:
The aim of this study was to evaluate the tolerability and efficacy of rapid quetiapine loading in youth diagnosed with pediatric bipolar disorder (PBD).
Method:
Quetiapine was started at 100 mg/day, and increased to 400 mg/day by day 5 in 75 bipolar children (6–16 years), presenting in an acute manic or hypomanic episode. Subsequent dose adjustments were predicated on the clinical picture. Response was defined as a ≥50% reduction in baseline scores on the Young Mania Rating Scale (YMRS). Clinical Global Impression–Improvement Scale (CGI-I) scores of “2 much improved” or “1 very much improved” were used as secondary measures of response. Remission was defined as a YMRS score of ≤12. Adverse events, blood pressure, weight change, somnolence, extrapyramidal syndrome (EPS), and akathisia were monitored to determine tolerability.
Results:
At 8 weeks, 94% of the sample had a CGI-I score ≤2, and 70% were in remission at 6 months. Sedation was reported by 50% of subjects during the first week; this rate dropped to 5.6% at 6 months.
Conclusion:
The findings indicate that rapid dose administration of quetiapine in children and adolescents with PBD is generally well tolerated and efficacious.
Introduction
Previous studies in youths have demonstrated the utility of quetiapine in the treatment of bipolar disorder (BD). When used as an adjunct to conventional mood stabilizers in adolescents, quetiapine has improved both the magnitude and rate of response (DelBello et al. 2002; DelBello et al. 2006). Quetiapine monotherapy has demonstrated efficacy comparable to divalproex in the management of manic symptoms in this population (DelBello et al. 2006). In addition, quetiapine may reduce manic symptoms more rapidly and result in greater remission rates than divalproex (DelBello et al. 2006). Quetiapine and other second-generation antipsychotics have a different and frequently better tolerated side-effect profile than first-generation antipsychotics (FGAs). Quetiapine has a low propensity to cause extrapyramidal symptoms (EPS), akathisia, or elevation of prolactin. Somnolence and sedation are the most common side effects of quetiapine therapy, but these effects are usually transient and frequently decrease when higher doses are used (Correll et al. 2008.)
Studies in adults show that rapid titration of quetiapine is well tolerated and promotes faster recovery (Hatim et al. 2006). Following a more conventional dosing schedule, one study (Bowden et al. 2005) demonstrated with a mean dose of 586 mg/day at day 21 a 50% decrease from baseline Young Mania Rating Scale (YMRS) scores for 53.3% of subjects, with an attrition rate of 6.5% primarily due to somnolence and weight gain. In hospitalized manic adults, an accelerated schedule with a loading dose of 200 mg on day 1, followed by a 200 mg/day dose increase on days 2, 3, and 4 was studied; by day 21, the mean dose was 900 mg/day, resulting in a ≥50% change from baseline YMRS in 75% of subjects by day 7, 57.8% remission by the end of week 1, and 73.7% remitting by day 21 (Hatim et al. 2006). Rapid dose escalation during week 1 was well tolerated with 5% attrition. Agitation was the most commonly reported side effect. No studies to date have investigated rapidly loading quetiapine in outpatient adults.
Rapid oral loading of valproate and lithium in adults has shown promise in the treatment of acute mania (Keck et al. 2001), but with more modest outcomes and/or more troubling side effects than that reported by Hatim et al. Rapid lithium (lithium carbonate formulation) loading starting at doses of 2,400–4,050 mg daily, depending on clinical considerations (age, weight, demonstrated lithium tolerance), was initiated in hospitalized adult patients meeting Diagnostic and Statistical Manual of Mental Disorders, 3rd edition (DSM III) (American Psychiatric Association 1981) criteria for mania, followed by dose reduction based on clinical state, side effects, and serum levels (Moscovich et al. 1992). Mean Clinical Global Impression–Severity (CGI-S) scores decreased by 22% after 48 h of lithium treatment. The Biegel–Murphy Mania State Rating Scale demonstrated a greater than 50% improvement in manic symptoms within the first week (Moscovich et al. 1992).
An open-label, 10-day pilot study examining the safety and efficacy of rapid administration and acute treatment with Lithibid® was initiated in 15 hospitalized adults with BD in manic or mixed episodes with or without psychotic features. A starting dose of 20 mg/kg per day was used. Doses were adjusted downward for patients whose serum lithium levels exceeded 1.4 mEq/L during the study, and for those not tolerating side effects. Although this study consisted of a small sample size and no control group, there was a greater than 50% decrease in baseline YMRS scores for 9 (60%) subjects by day 10. This dosing strategy was generally well tolerated, although 3 (20%) participants developed new-onset bradycardia, and other side effects included nausea (n = 2), diarrhea (n = 2), tremor (n = 2), dizziness (n = 2), fatigue (n = 2), and polydipsia (n = 1) (Keck et al. 2001). Care must be taken to avoid lithium toxicity (Carroll et al. 2001). There are currently no published studies evaluating rapid loading of lithium in children.
The safety and tolerability of accelerated oral loading of divalproex in acutely manic bipolar patients has also been studied. In a randomized, double-blind, parallel-group trial comparing oral loading of divalproex with standard titration of either divalproex or lithium, loading doses of divalproex of 30 mg/kg per day for 2 days followed by 20 mg/kg per day was as well tolerated at the usual divalproex and lithium dosing (Hirschfeld 1999). This study examined 59 patients, aged 18–60 years, with a Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association 1994) diagnosis of BD (manic or mixed) and hospitalized for treatment of an acute manic episode (Hirschfeld et al. 1999). In addition to rapid oral loading of divalproex being as well tolerated as the other two methods, the rapid-loading dose group attained therapeutic concentrations more rapidly than the other groups (Hirschfeld et al. 1999).
In PBD, rapid loading comparable to the current report has been previously reported up to 400–450 mg/day (DelBello et al. 2006). Rapid dosing of quetiapine beyond 400 mg/day has not been published in children. The purpose of this study is to investigate rapid titration of quetiapine in manic children with BD. It was hypothesized that rapid escalation of quetiapine to 400 mg and beyond would be well tolerated and demonstrate fuller and a more rapid symptom reduction.
Method
We describe a retrospective study evaluating the treatment of referred patients with a diagnosis of BD I or II. Institutional Review Boards at the respective institutions approved the data collection as part of a clinical research registry. Study data were derived from clinical data authorized by patients through assent and parent/guardian consent for research activities consistent with this study. Although the data were collected prospectively, this was a retrospective study methodologically. No subjects were included who at any time voiced any desire to be excluded. All treatment decisions were made in the best interests of the individual subjects based upon what was considered to be the best available information and the established treatment guidelines of the clinics. Parental consent and child assent were secured prior to initiating all treatments.
Table 1 displays sample characteristics; a total of n = 75 bipolar children between 6 and 16 years of age, in current manic or hypomanic episodes, were identified via chart review with diagnosis confirmed through the administration of the Washington University Kiddie Schedule for Affective Disorders and Schizophrenia (WASH-U-KSADS). YMRS and Clinical Global Impression–Improvement (CGI-I) scales were recorded at the time of each visit, as is routine in our clinics. Inclusion criteria consisted of outpatients, with a diagnosis of BD I or II, current manic, or hypomanic episode indicated by DSM-IV criteria, a baseline YMRS score of ≥20, at least one dose of study medication, and at least one postbaseline efficacy and tolerability measurement. Concomitant anticonvulsants, mood stabilizers, and stimulants were allowed. Although antidepressants were not exclusionary for this clinical naturalistic study, no subjects were on antidepressants. Exclusion criteria included substance abuse disorder, diagnosis of pervasive developmental disorder, mental retardation, or a demonstrated intolerance to quetiapine.
Abbreviations: BD = Bipolar disorder; ADHD = attention-deficit/hyperactivity disorder; DVP = divalproex.
The YMRS is not a diagnostic instrument, but does generally reflect an overall severity of mania. The convention is that a YMRS score of about 20 is moderate in severity. The combination of a shorter than 7 days, but more than 4 days, and lack of psychiatric hospitalization or significant impairment resulted in our diagnosing a portion of the subjects with BD II.
All subjects received an initial dose of quetiapine 100 mg/day on day 1, and increased to 400 mg/day by day 5. Thereafter, dose adjustments were clinically guided, taking into account drug tolerability and symptom severity. In some cases, this exceeded the Food and Drug Administration (FDA) package insert recommendation of 800 mg/day, with a range 400–1000 mg/day. At 6 months, the mean dose was 750 mg/day (standard dose (s.d.) = 151 mg/day). Other measures of central tendency were similar (median and mode = 800 mg/day).
The YMRS and CGI-I scale were administered to all subjects at baseline, 2 weeks, 4 weeks, 8 weeks, 12 weeks, and at 6 months. A criterion for response was defined as a ≥50% decrease in baseline YMRS scores. CGI-I scores ≤2 were reported as a secondary measures of response. Remission was defined as a YMRS score of ≤12.
Tolerability was measured through collection of data regarding adverse events using the Side-Effects for Children and Adolescents (SEFCA), blood pressure, pulse, and weight change. Somnolence, EPS, and akathisia were assessed through patient and parent report and a focused physical exam for EPS if indicated.
Analysis was performed using the Statistical Package for the Social Sciences for Windows, version 15.0 (SPSS 15), and a last observation carried forward (LOCF) approach was implemented, with alpha set at p = 0.05 (two-tailed). Descriptive analysis of means, standard deviations, frequencies, and percentages were derived from data. Two-way mixed analysis of variance (ANOVA) with between-subjects measures response status, gender, and attrition status, and within-subject measure of time (baseline, 2 weeks, 4 weeks, 8 weeks, 12 weeks, and 6 months) were used to examine main effects and interactions between factors. Although we could not assume equal variance for each set of difference scores, the Greenhouse–Geisser correction was used, and LOCF was used to assure a complete data set. Chi-squared and correlation analysis were used to evaluate relationships between missing data and variables in an effort to determine if data were missing completely at random. There were a series of null hypothesis for the rapid loading of quetiapine in our sample: (1) There will be no difference in YMRS or CGI-I scores between baseline and 6 month measures for all subjects, (2) there will be no difference in YMRS or CGI-I scores between males and females over the course of the study, and no interaction between these variables, and (3) there will be no relationship between YMRS or CGI-I scores and other variables collected, between those subjects missing outcome data and those who are not. When baseline measures were discrepant for between subject factors, analysis of covariance (ANCOVA) was used to adjust for these baseline differences.
Results
Subject demographics are reported in Table 1. A total of n = 75 consecutive subjects were included in the study. Participants were on average 9.5 years old (standard deviation [SD] 2.2 years). Twenty-eight (37%) subjects were female, and the ethnic distribution matched that of the area: 52 (69%) Caucasian, 12 (16%) African American, 5 (6.7%) Hispanic, 5 (6.7%) Asian, and 1 (1.3%) Native American. Forty-nine (65%) subjects had a BD I diagnosis, and 39 (80%) of these BD I patients also met criteria for attention-deficit/hyperactivity disorder (ADHD); 26 (35%) subjects had a BD II diagnosis, and 18 (70%) of these BD II patients also met criteria for ADHD. All subjects were titrated to 400 mg/day by day 5. The 400-mg/day dose was maintained until the follow-up visit at week 2. Doses were adjusted at subsequent clinic visits based on clinical response. At week 4, the mean dose was 554 mg/day (±75 mg/day); and 726 mg/day (±103mg/day) at week 8; 748 mg/day (±95mg/day) at week 12, and 796 mg/day (±125mg/day) at 6 months. Whereas overall dose increased over the course of the study, no differences were observed by gender F(1,72) = 0.035, p = 0.852, nor any dose and gender interaction effects, F(1.998,143.889) = 0.0.108, p = 0.980. Initially, sedation appeared to be related to rate of dose escalation rs (70) = 0.71, p < 0.05, indicating a slower titration for those who experienced somnolence, although final dose was unrelated to sedation.
Some outcome data points were missing for 40% of subjects. Missing data were not related to any major variables including gender χ2(1) = 0, p = 1.0, ethnicity χ2(4) = 3.378, p = 0.497, dose escalation rs (70) = 0.89, p = 0.457, sedation χ2(1) = 0.91, p = 0.34, weight gain χ2(10) = 11.44, p = 0.324, concurrent diagnosis χ2(3) = 1.134, p = 0.769 or concomitant medications χ2(5) = 3.119, p = 0.682. Missing data were most frequently related to early clinical response and a return to a previous provider.
Between baseline and week 2, 50% of subjects reported sedation. By week 4 this rate had dropped to 15% and continued to decrease throughout the course of the study; at the 6-month visit, 5.6% of subjects reported somnolence. Our data did not support a relationship between stimulant use and patient report of sedation rs ,(54) = 0.132, p = 0.34. Orthostatic hypotension was not reported. Conversely, a statistically significant, although clinically unimportant increase in diastolic F(1,53) = 7.756, p = 0.01 (d = 0.05), blood pressure was observed with higher doses. No changes in systolic blood pressure were reported. A mean weight increase of 3 lbs (range = –1 to 6 lbs, s.d. 1.5 lbs) was observed during the 6-month study period, which was expected and is consistent with normal growth patterns for our sample when compared to standard growth charts. Lithium or valproate combination therapy did not appear to be related to greater weight gain F(2,53) = 0.1831, p = 0.833. Similarly, co-administration of stimulants did not appear to reduce weight gain observed with quetiapine treatment t(54) = 0.459, p = 0.648.
Subjects were dichotomized into remitters (final YMRS ≤12) and nonremitters (final YMRS > 12), with 70% of intent-to-treat sample meeting remission criteria at 6 months (Fig. 1). There was a main effect for YMRS change over the course of the study, F(3.152,226.957) = 3.58, p = 0.013 (Greenhouse–Geisser correction), main effect for response status, F(1,72) = 53.75, p < 0.01, and a significant interaction between YMRS and response status, F(3.152,226.957) = 30.876, p < 0.01 (Greenhouse–Geisser correction). Post hoc analysis revealed that both remitters and nonremitters improved, although remitters improved by a greater margin. Differences between remitters and nonremitters were discernable at 2 weeks, with an effect size of d = 1.218. As the study progressed, the discrepancy between remitters and nonremitters was increasingly evident, and, at week 8, nonremitters mean YMRS was located at the 96th percentile of the remitters 8-week YMRS distribution, with 75.4% non-overlap between the two distributions. Clinically, these two populations were differentiable at 8 weeks. Using LOCF, there was evidence of a 50% decrease from baseline YMRS by week 8 for, n = 59 (79%) of sample, and CGI-I scores ≤2 at week 8 for n = 67 (90%) of sample.
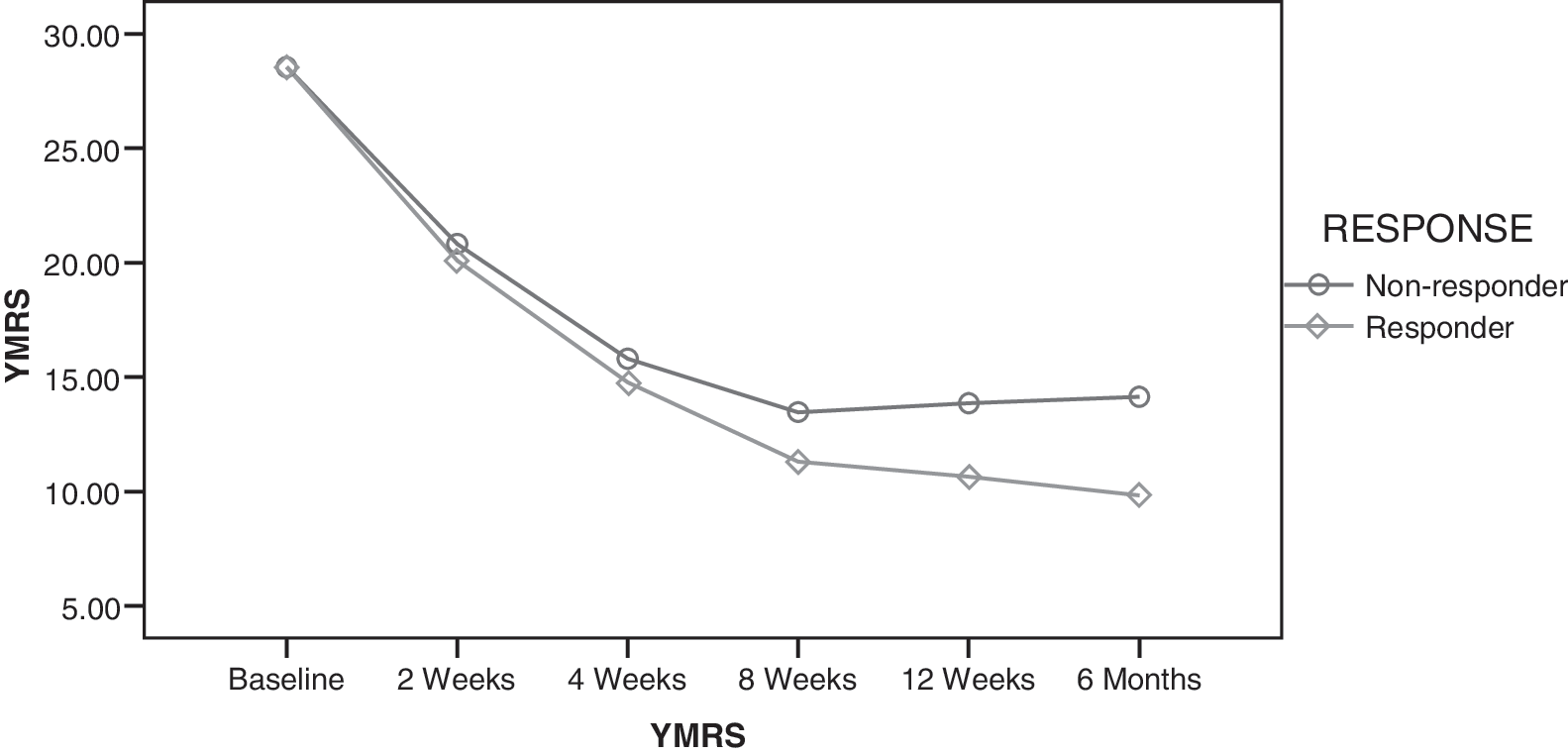
Average Young Mania Rating Scale (YMRS) scores throughout the course of the study for sample responders and nonresponders.
Discussion
In this study we evaluated the safety and efficacy of rapid quetiapine titration in children with BD. The findings indicate that rapid dose administration of quetiapine in children is generally well tolerated and efficacious. On starting patients with PBD at 100 mg/day, increasing dose to 400 mg/day by day 5, and subsequent increases in dosing subsequently guided by clinical impression, there was a mean end of study dose of 796 mg/day (±125mg/day) (see Table 1). This dosing has been consistently related to full clinical response in clinical samples for youths with both BD and psychotic illnesses. Analysis revealed that data were missing at random, and that there were no distinct differences between those missing data (leaving the clinic early) and those who were not in terms of gender, age, ethnicity, dose escalation, sedation, weight gain, response to treatment (as measured by YMRS and CGI-I scores), concurrent diagnosis, or concomitant medications.
The most commonly reported effect of rapid dose administration was somnolence. This is comparable to published controlled studies on quetiapine, and is likely explained by H1 antagonism. Tolerance to this effect could explain the decrease in sedation reported by subjects after the first 2 weeks of the study (Correll 2008). There is some clinical suggestion that rapid escalation may, in fact, decrease the length and perhaps the severity of sedation. Sedation was equally reported, regardless of the use (or not) of concomitant medications. Other antihistiminic side effects are known to be related to treatment with quetiapine and appear to be more common at lower doses. Histamine acts as an anorexigenic amine and plays a role in the regulation of appetite and metabolism, possibly through mediation of the leptin system (Jørgensen et al. 2007). Correll (2008) indicates that we might expect a greater SGA-induced weight gain with a mood stabilizer/SGA combination than with SGA monotherapy. It is possible that rapid quetiapine loading can more quickly move patients out of the lower dose range, and as a result, we observe less SGA-related weight gain. In addition, many of our patients were not drug naïve. This has been suggested to result in less weight gain (Correll 2008).
Orthostasis is commonly reported during treatment with quetiapine. At higher doses, adaptation of the α-adrenergic system and or blockade of α 2 autoreceptors may reduce orthostasis (Correll 2008). Interestingly, we observed an increase in diastolic blood pressures at higher doses. Children are often described as having "more elastic" arteries and may therefore be less susceptible to orthostatic hypotension than adults or, more specifically, the elderly. Weight gain is another effect associated with the use of quetiapine. There was a mean 5% increase from baseline weight at 6 months, which was not mediated nor moderated by other subject medications. Although the full impact of treatment with quetiapine is not yet realized at 8 weeks, n = 67 (90%) had improved (CGI-I ≤2) and n = 59 (79%) of subjects had a ≥50% decrease in YMRS from baseline. By 8 weeks, the distinction between remitters and nonremitters becomes very clear, and at 6 months, n = 52 (70%) of sample were in remission (YMRS ≤12).
Whereas LOCF is a conservative approach to evaluating efficacy findings in our study, this approach may underestimate effective dosing and rate of dosing. As a result, it may be advisable to increase dose even beyond that reported in this study. This study was a pre-experimental design with no control group and a convenience (clinically referred) sample. As a result, internal and external validity should be interpreted with caution.
Conclusion
In summary, a sample of 75 manic or hypomanic (baseline YMRS ≥20) pediatric patients (6–16 years) diagnosed with BD I or BD II were identified and determined suitable for treatment with quetiapine fumarate. Subjects received an initial dose of quetiapine 100 mg/day and were increased to 400 mg/day by day 5. Thereafter, any dose adjustments were clinically guided, taking into account drug tolerability and symptom severity. The findings indicate that rapid dose escalation of quetiapine in children is well tolerated and generally leads to significant and stable improvement in YMRS and CGI-I scores at 6 months.
Footnotes
Disclosures
In the last 3 years, Dr. Scheffer has had the following interactions with pharmaceutical companies: on speakers bureau for, consultant for, and has received research support not related to this paper from Astra-Zeneca; and has received research support from Wyeth, Pfizer, and Bristol Myers Squibb. Dr. Scheffer owns no stock in any pharmaceutical company. The remaining authors have no financial ties to disclose.
There has been no financial support for this manuscript of any kind.