
Abstract
Objectives:
The aims of this study were to determine if relationships exist between the efficacy of atomoxetine for treatment of attention-deficit/hyperactivity disorder (ADHD) and demographic characteristics, specific co-morbid diagnoses, subtype of ADHD, and/or additional use of a stimulant medication.
Method:
A retrospective chart review was performed using data from an institutional electronic medical record system. Children aged 5–17 years who were diagnosed with ADHD and prescribed atomoxetine were included; 432 study subjects were categorized as treatment success (TS), treatment failure (TF), or undetermined. Co-morbid diagnoses, demographic factors, subtype of ADHD, and additional use of stimulant medications were examined for association with TS.
Results:
A total of 88 children were categorized as TS, 197 as TF, and 147 as undetermined. More subjects in the TS group were receiving stimulant medication in addition to the atomoxetine than in the TF group (p = 0.0319; 95% Wald confidence interval [CI], 1.064–3.972). There was no significant difference between groups for any demographic characteristic, the presence of any co-morbid diagnosis, or type of ADHD. In particular, the presence of anxiety or depression was not associated with a response to atomoxetine.
Conclusion:
Children who were prescribed a stimulant medication in addition to atomoxetine had better outcomes in treating ADHD than those receiving only atomoxetine.
Introduction
Although ADHD is a distinct disorder, conditions such as oppositional defiant disorder (ODD), major depressive disorder (MDD), anxiety disorder, learning disorders, conduct disorder (CD), bipolar disorder (BD), enuresis, and substance-related disorders may mimic or coexist with ADHD (Spencer et al. 2002a).
A single etiology for ADHD has not been identified. Instead, the disorder is thought to have a multifactorial basis. Proposed etiologies, including prenatal and perinatal risk factors, genetics, and neurobiological deficits, may all contribute to the pathophysiology of ADHD (Spencer et al. 2002a). It appears that the disorder involves abnormalities of dopaminergic and noradrenergic neurotransmission in the frontal cortex (Michelson et al. 2004).
Medications that affect dopaminergic and noradrenergic neurotransmission, such as the stimulants methylphenidate and d-amphetamine, are the most commonly used medications for treatment of ADHD. Although these medications are generally considered effective and safe for treatment of ADHD in children and adolescents, approximately 30–50% of all children and adults with ADHD either do not respond to or do not tolerate treatment with stimulants (Greenhill 1995; Wilens et al. 1995). These drugs have common side effects, including weight loss, stomachaches, headaches, tic exacerbation, and initial insomnia (Spencer et al. 2002b; Tasman et al. 2003).
Although several antidepressant medications have been used in the treatment of ADHD, including tricyclic antidepressants, monoamine oxidase inhibitors, and others, atomoxetine is the first nonstimulant agent approved by the Food and Drug Administration (FDA) for treatment of ADHD in children and adults. Atomoxetine, initially developed as an antidepressant, is marketed for treatment of ADHD by a novel mechanism of action, the highly selective inhibition of the presynaptic norepinephrine transporter, which inhibits the reuptake of norepinephrine.
Data from clinical trials demonstrate atomoxetine to be well tolerated and effective in treatment of ADHD in children and adolescents (Hammerness et al. 2009a, Kelsey, 2004). However, our clinical experience with this medication in treating children and adolescents with ADHD has been disappointing. In an effort to identify groups likely to have success with atomoxetine treatment for ADHD, and thus efficiently target its use, this study was developed to investigate the efficacy of atomoxetine in certain subgroups of children and adolescents with ADHD. We retrospectively examined factors contributing to treatment success by analyzing data from our institution's electronic medical record system.
The primary aims of our study were to determine if there is a relationship between the efficacy of atomoxetine in ADHD and: (1) Demographic characteristics, (2) specific co-morbid diagnoses (Table 1), (3) subtype of ADHD, and (4) additional use of a stimulant medication.
Methods
Design
A retrospective study was performed using data from the institutional electronic medical record system. A search was performed in providers' notes of the child and adolescent psychiatry, pediatric, and family practice clinics of our institution, a large multispecialty group practice affiliated with a university training program, using diagnostic codes for ADHD. Limits were set for ages 5–17, and for the keywords “Atomoxetine” and “Strattera.” Co-morbid diagnoses (Table 1), demographic factors, subtype of ADHD, and additional use of stimulant medications in patients diagnosed with ADHD were also recorded and correlated with success of treatment of ADHD with atomoxetine.
Participants
All children and adolescents aged 5–17 years of all ethnicities who were diagnosed with ADHD by the clinician were included in the study. There were no exclusions.
Measures
International Classification of Diseases, ninth revision (ICD-9) codes for ADHD and the keywords “atomoxetine” and “Strattera” were searched in the electronic medical records of providers from the child and adolescent psychiatry, pediatric, and family practice clinics from dates November 26, 2002 (the date of FDA approval for use of atomoxetine in children and adolescents for treatment of ADHD) to April 20, 2005. Subjects for whom atomoxetine was prescribed were included in the study.
Records were then examined manually for evidence of discontinuation of atomoxetine. Subjects for whom atomoxetine was discontinued due to an adverse effect or for stated ineffectiveness were classified into the treatment failure (TF) group. Subjects for whom atomoxetine was discontinued for reasons excluding ineffectiveness or adverse reactions (e.g., discontinued because no longer needed or for a medication holiday) were classified into the treatment success (TS) group. Subjects for whom there was insufficient information in the chart to determine a reason for discontinuation were classified into the undetermined group.
Records of subjects for whom atomoxetine was not discontinued were then manually analyzed further. Subjects for whom records included subjective evidence of success (statements in the record such as “doing well”, “improved”) were classified into the TS group. Subjects for whom atomoxetine was continued, even without evidence of success noted in the record, were also classified into the TS group. Subjects for whom it could not be determined whether or not atomoxetine was continued were classified into the undetermined group. (Fig. 1 and Table 2).
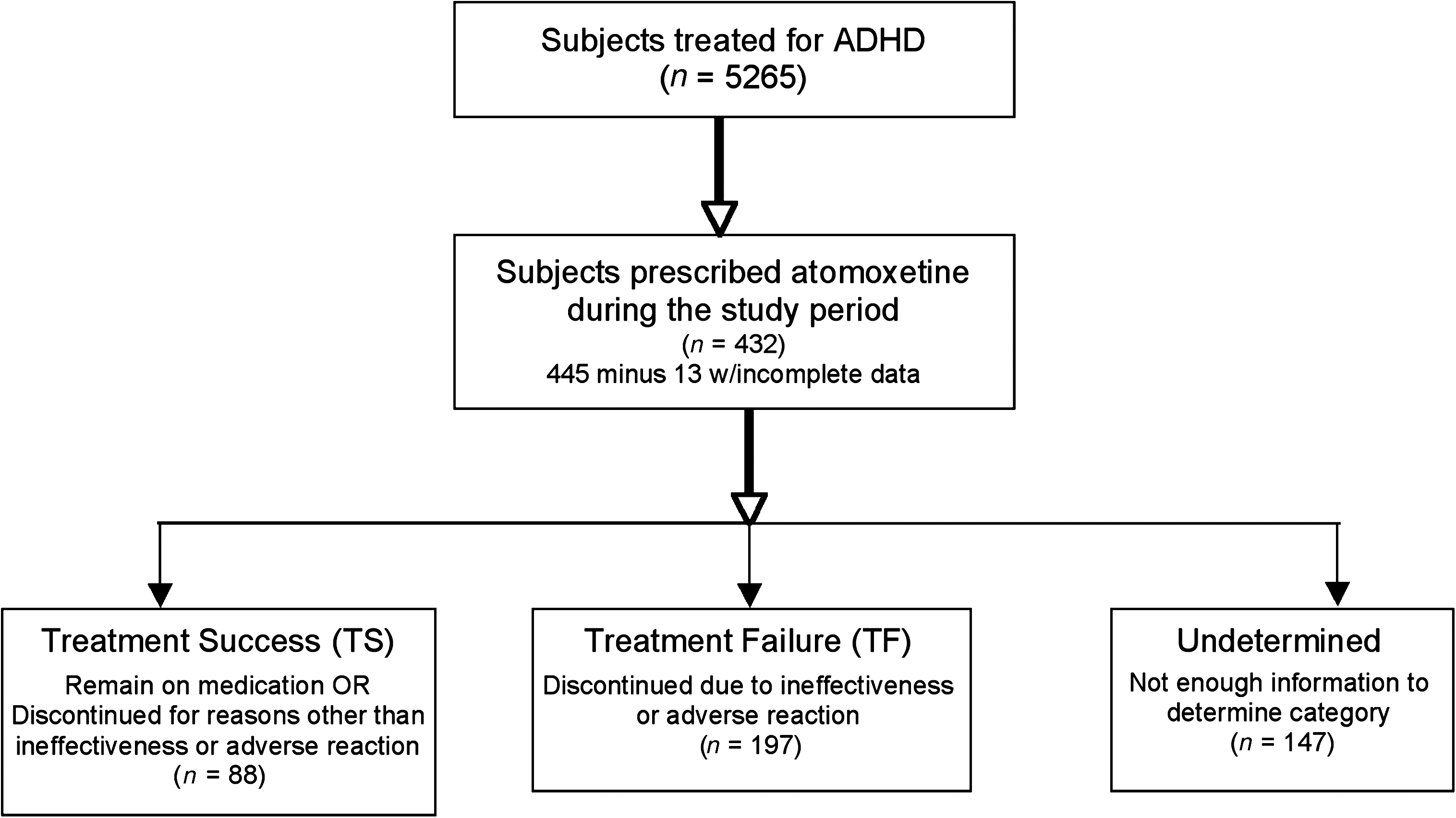
Study set-up. ADHD = Attention-deficit/hyperactivity disorder.
Abbreviations: TS = Treatment success; TF = treatment failure.
Medical records were also analyzed to determine the current age, age at start of atomoxetine, dose, gender, ethnicity, weight, type of ADHD, and co-morbid diagnoses as well as stimulant medication use by subjects.
Data analysis
We used univariate and multivariate logistic regression analysis (Wald statistic), in the analysis of the study main outcome, namely treatment success versus treatment failure. A p value of less than 0.05 indicated a statistical significance. SAS 9.1.3 (SAS Institute Inc., Cary, NC) was used for statistical analysis.
Results
During the time period studied, 5,265 children ages 5–17 years were treated for ADHD in the child psychiatry, pediatric, and family practice clinics. Of these, 445 were prescribed atomoxetine during the study period and 432 had sufficient data for study inclusion. Of these 432 subjects, 147 were categorized into the undetermined group. Of the 285 subjects with sufficient data for inclusion in the study, 88 (30.9%) were judged to have a successful response to atomoxetine (TS) and 197 (69.1%) were judged to have a failed response to atomoxetine (TF). The undetermined group differed significantly from the study group on gender, atomoxetine start age, use of stimulant medication, and presence of any co-morbid disorder (Table 3).
Abbreviations: ADHD = Attention-deficit/hyperactivity disorder; TS =treatment success; TF = treatment failure.
Patient demographics
In the study sample of 285 subjects, 209 (73.3%) were male and 221 (77.5%) were white and 64 (22.5%) were non-white (Table 4). The average age at initiating atomoxetine was 10.6 ± 3.1 and the mean weight was 43.7 kg ± 18.9 (Table 4).
Abbreviations: ADHD = Attention-deficit/hyperactivity disorder; TS =treatment success; TF = treatment failure.
The TS group included 88 patients. Sixty-four (72.7%) of the patients were male, with 62 (70.5%) white patients and 26 (29.6%) non-white patients (Table 4). The average age at initiating atomoxetine was 10.5 years ± 3.2. The mean weight was 47.1 kg ± 20.6 (Table 3).
The TF group included 197 patients. One hundred forty-five (73.6%) of the patients were male, with 159 (80.7%) white patients and 38 (19.3%) non-white patients (Table 4). The average age at initiating atomoxetine was 10.6 (±3.0) years. The mean weight was 42.2 kg (±17.9) (Table 4).
There were no significant differences in demographic characteristics between children in the TS and the TF group (Table 4). The p value for ethnic group was 0.0609, suggesting a marginal association between non-white ethnicity and the TS group (Table 5).
pr > Wald chi-squared.
Abbreviations: ADHD = Attention-deficit/hyperactivity disorder; CI =confidence interval; N.S., not significant.
Co-morbid diagnoses
Of the entire study group, 205 (72%) had any co-morbid diagnosis. In the TS group, 32 (36.4%) had a co-morbid diagnosis of ODD, 21 (23.9%) had depression, 18 (20.5%) had an anxiety disorder, 21 (23.9%) had a learning disorder, 2 (2.3%) had CD, 10 (11.4%) had BD, 6 (6.8%) had enuresis, and 1 (1.1%) had a substance-related disorder. In the TF group, 61 (31.0%) had ODD, 60 (30.5%) had depression, 44 (22.3%) had an anxiety disorder, 47 (23.9%) had a learning disorder, 12 (6.1%) had CD, 22 (11.2%) had BD, 8 (4.1%) had enuresis, and 6 (3.0%) had a substance-related disorder (Table 6). There was no significant difference between groups for the presence of any co-morbid diagnosis (Table 5).
Abbreviations: TS = Treatment success; TF = treatment failure; ODD =oppositional defiant disorder.
Type of ADHD
Of the children in the TS group, 59 (67.0%) had been diagnosed with the combined type of ADHD and none had been diagnosed with the hyperactive-impulsive type of ADHD. Ten (11.4%) had been diagnosed with the inattentive type of ADHD. Of the children in the TF group, 115 (58.7%) had been diagnosed with the combined type of ADHD, whereas10 (5.1%) had been diagnosed with the hyperactive-impulsive type of ADHD. Thirty (15.3%) had been diagnosed with the inattentive type of ADHD (Table 7).
Abbreviations: ADHD = Attention-defict/hyperactivity disorder; TS =treatment success; TF = treatment failure.
In the univariate analysis, there was no significant difference between groups for the type of ADHD diagnosed. For the multivariate analysis, all types of ADHD other than inattentive type were pooled to strengthen a possible association of treatment success with inattentive ADHD. There was no significant difference between the two treatment groups on inattentive or non-inattentive type ADHD.
Additional use of a stimulant medication
Use of any stimulant medication was documented in 54 (18.9%) of the entire sample. In the TS group, 24 (27.3%) of the subjects were prescribed a stimulant medication in addition to atomoxetine, whereas in the TF group, 30 (15.2%) were receiving a stimulant medication in addition to atomoxetine. The multivariate analysis revealed a p value of 0.0319 (95% Wald confidence interval [CI], 1.064–3.972), which suggests that more subjects in the TS group were receiving stimulant medication in addition to the atomoxetine than in the TF group (Table 5). Data on specific stimulants used are described in Table 8.
Abbreviations: TS = Treatment success; TF = treatment failure.
Discussion
We explored the role of a number of potential variables in relation to efficacy of atomoxetine in treating ADHD in children and adolescents. In this naturalistic treatment setting, the overall success of atomoxetine treatment for ADHD was 30.9%, which is similar to the number needed to treat (NNT) of 3.43 reported by Cheng et al. (2007) in their meta analysis. Few factors seemed to be associated with success of atomoxetine treatment for ADHD.
One factor that did seem to be associated with atomoxetine treatment success was use of stimulant medication in addition to atmoxetine. Differences between the TS and TF groups for patients who were also prescribed stimulant medications revealed a p value of 0.0319, which is significant. From a case report (Brown 2004), one small pilot study (Carlson et al. 2007), and an open trial (Wilens et al. 2009), there is evidence that combining atomoxetine and stimulant medication may provide additional improvement in ADHD symptoms for some children. In our study, multivariate analysis revealed that significantly more children who were on atomoxetine plus a stimulant medication were in the TS group (p = 0.0319). Stimulant medications act primarily on the dopaminergic system with some noradrenergic activity, and atomoxetine acts primarily on the noradrenergic system. Thus, the two medications can complement each other, addressing symptoms arising from both neurotransmitter systems. Carlson et al. (2007) suggested that both medications could be used complementarily to reduce exposure to side effects. However, Hammerness et al. (2009b) found an additive effect of adverse events when OROS-methylphenidate was added to atomoxetine for treatment of ADHD. Further trials to determine if the addition of a stimulant to an atomoxetine regimen improves symptoms over use of the stimulant alone will clarify the usefulness of this combination and provide information against which the increase in adverse effects can be weighed.
Univariate analysis of differences between the TS and TF groups for ethnicity revealed a p value of 0.0553, which could represent a marginal association between non-white racial ethnicity and treatment success with atomoxetine. A multivariate analysis showed similarly that the relationship was not significant at the 0.05 value (p value 0.0609; 95% Wald CI, 0.301–1.027). Differences between ethnic groups in response to medications have been documented previously (Agrawal and Khan 2007), however, and may be related to genetic differences. In a multicenter, randomized, open-label study of OROS methylphenidate versus atomoxetine, treatment outcomes in African-American children with ADHD showed a greater response to OROS methylphenidate than atomoxetine at 3 weeks (Starr and Kemner 2005). Bellgrove et al. (2008) found that improvement of certain ADHD symptoms varied as a function of a particular genotype. As in all studies in which efficacy must be determined by subjective outcomes such as an absence of discontinuation of atomoxetine treatment as in this study, some factors other than true efficacy could result in inclusion in the treatment success group. Therefore, factors not included in the multivariate analysis but related to ethnicity, such as communication barriers across cultural groups, may have contributed toward the marginal association of ethnicity to treatment success.
We hypothesized that children and adolescents with anxiety and/or depression co-morbid with their ADHD would be more likely to find success with atomoxetine treatment because symptoms of both their ADHD and their co-morbid disorders would be treated. Residual anxiety or depression symptoms that might confound other ADHD treatments would be treated, and atomoxetine would therefore give the most relief from all of the child's symptoms. Atomoxetine, chemically similar to tricyclic antidepressants, does seem to be effective in treating depression in pediatric patients. A randomized, double-blind trial examined the use of atomoxetine alone or in combination with fluoxetine for treating pediatric patients with ADHD and co-morbid depressive or anxiety symptoms. Atomoxetine monotherapy appeared to be effective for treating both ADHD and anxiety and depressive symptoms (Kratochvil et al. 2005). In addition, a clinical trial on augmentation with atomoxetine for partial or nonresponse to antidepressants demonstrated a significant decrease in Inventory of Depressive Symptomatology-Self Report scores (Carpenter et al. 2005). In adults with ADHD, Spencer et al. (2006) found that the presence of lifetime depression at baseline predicted successful treatment of ADHD symptoms with atomoxetine. There are conflicting studies regarding the effectiveness of atomoxetine in treatment of depression, however. A randomized, double-blind, placebo-controlled study on the addition of atomoxetine for depression incompletely responsive to sertraline demonstrated no improvement more than placebo (Michelson et al. 2007). Also, the Atomoxetine ADHD and Comorbid MDD Study Group et al. (2008) found no improvement in depressive symptoms in adolescents with ADHD and MDD when treated with atomoxetine, although their ADHD symptoms did show improvement. We did not find any significant differences between TS and TF groups with respect to depression or anxiety using multivariate logistic regression analysis or univariate analysis.
A meta-analysis of data reviewing the effect of co-morbid symptoms of ODD on responses to atomoxetine in children with ADHD showed that atomoxetine treatment significantly reduced ADHD symptoms in both ODD co-morbid and non-co-morbid subjects to similar extents (Biederman et al. 2007). An 8-week randomized, double-blind placebo controlled study in children and adolescents ages 8–18 showed that atomoxetine treatment improved ADHD and ODD symptoms in youths with ADHD and ODD, although the co-morbid group may require higher doses (Newcorn et al. 2005). Bangs et al. studied 6- to 12-year-olds with ADHD and ODD and found improvements in ADHD and ODD symptoms early in the study (Bangs et al. 2008). At the end point, however, only improvement in ADHD symptoms remained greater than placebo. Similarly, in our study, the presence of co-morbid ODD predicted neither favorable nor unfavorable responses to atomoxetine treatment.
A randomized controlled trial on the effects of atomoxetine on bladder control in children with nocturnal enuresis showed the medication to be associated with a significant increase in dry nights in children with nocturnal enuresis (Sumner et al. 2006). Our study did not demonstrate any significant difference in efficacy of atomoxetine for treatment of ADHD in children who also have enuresis. We did not investigate the efficacy of the medication in treating enuresis.
The effectiveness of atomoxetine in treating ADHD is described in the literature for all ADHD subtypes (Michelson et al. 2004; Arnold et al. 2006). Our study did not show a difference in the efficacy of atomoxetine in treating ADHD based on subtype of ADHD.
Study Limitations
This was a retrospective study that used patient records for the data source. Although easily searchable to identify potential study subjects and a revealing source of real-world clinical practices, the use of an electronic medical record system did not ensure consistent documentation of data from providers. A number of clinicians had used rating scales to assess response to atomoxetine, but the results of the scales were not routinely included in the progress notes. As a result, treatment success in this study was based on clinicians' subjective impressions regarding atomoxetine effectiveness or continuation of treatment with the atomoxetine. Assuming success of a treatment regimen based on continuation of the regimen presumes that all medications are only continued if effective even when other medications are prescribed at the same time for the same condition. The findings of this study hold only if this assumption is valid. This issue highlights the general need for all clinicians to systematically use objective tools for measuring efficacy of treatments and for recording the resultant data in the progress notes.
In addition, one-third of the potential subjects was excluded from the study because of insufficient data in the chart to determine whether or not the use of atomoxetine was a successful intervention for the child's ADHD. This excluded group differed significantly from the study group on several variables, including gender (more males in undetermined group, p = 0.1), age at atomoxetine start (more started under age 12 years in undetermined droup, p < 0.001), use of stimulant (fewer using stimulant in undetermined group, p = 0.002), and presence of co-morbidities (fewer co-morbidities present in undetermined group, p = 0.034), suggesting that there may be a systematic explanation for the lack of data.
The loss of one-third of the potential subjects due to insufficient data in the record significantly impacted the sample size. With a larger sample size there may have been sufficient power to reveal additional findings.
As discussed above, there remains some question as to whether or not continuation of atomoxetine, while on a stimulant, is actually a reflection of treatment success. Children and adolescents on stimulant and atomoxetine may have been maintained on both because symptoms resolved when the stimulant was added to atomoxetine. In addition to a possible complementary effect of stimulant plus atomoxetine, one must consider the possibility that the stimulant alone provided the benefit. Without objective evidence, there remains uncertainty regarding the source of the symptom resolution that may have been experienced by the clinician as well and thus both medications were continued. Clinicians may be reluctant to discontinue medications thought to be providing some benefit.
Conclusions
The current study failed to find evidence for a relationship between the efficacy of atomoxetine treatment for ADHD and gender, age, or ethnicity, although there was a marginal association between treatment success and ethnicity. No evidence for a relationship between the efficacy of atomoxetine treatment for ADHD and co-morbid diagnoses, including depression or anxiety, or type of ADHD was noted. However, a significant difference was noted between the number of children and adolescents taking stimulants in the TS group compared to the TF group. This statistical finding may suggest some benefit to combining atomoxetine and stimulant. Controlled trials are needed to understand further the potential benefit in clinical practice of combining atomoxetine and stimulant medications. Additional efforts to identify predictors of atomoxetine success will need to be undertaken.
Footnotes
Disclosures
The authors have no conflicts of interest to disclose.