
Abstract
Objectives:
The primary objective of this study was to demonstrate efficacy of Ritalin® LA 20 mg by showing superiority to placebo and noninferiority to Medikinet® Retard in a laboratory classroom setting. Secondary objectives included safety/tolerability and further efficacy parameters.
Methods:
A total of 147 children with attention-deficit/hyperactivity disorder (ADHD) diagnosed by the Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS) and aged 6–14 (81% males) and known to be methylphenidate (MPH) responders were enrolled in this multicenter, double-blind, randomized, placebo/active-controlled, three-period (7 days each) crossover study. The Swanson, Kotlin, Agler, M-Flynn, and Pelham (SKAMP) scale was used for efficacy ratings. The mean of SKAMP Combined ratings performed at 10:30 a.m., at 12:00 a.m., and at 1:30 p.m. was defined as the primary parameter.
Results:
In all, 146 patients completed all treatment periods. Intensity and frequency of adverse events were comparable between the two formulations. Ritalin® LA demonstrated superiority compared to placebo (p < 0.0001). The observed difference in the SKAMP scores between Ritalin® LA and Medikinet® Retard between the hours 1.5 until 4.5 did not exceed the noninferiority margin (p = 0.0003); therefore, the difference is regarded as not clinically relevant. Similar results were obtained for the secondary efficacy variables.
Conclusion:
Ritalin® LA is an efficacious, well-tolerated treatment option for children aged 6–14 with ADHD.
Introduction
Treatment with methylphenidate (MPH) has being applied for more than 50 years and is still considered the gold standard. The longest known treatment consists of immediate-release (IR) MPH. MPH acts mainly on the dopaminergic system in the brain and enhances dopamine concentrations in the synaptic cleft (Volkow et al. 2005). Responder rates reach up to 70% for stimulants (Spencer et al. 1996). However, the pharmacokinetics of IR MPH show a short half-life of 2–3 hours, and therefore several daily doses have to be administered throughout the day (Swanson and Volkow 2002). Common problems are that the subsequent doses are either forgotten or not taken due to social stigmatization in school. During the last years, several new galenic MPH preparations have been introduced that provide the possibility of a once-daily dosing. This approach is supposed to increase the compliance as well as to ensure an optimal supply with MPH throughout the day.
In Germany, three proprietary extended-release (ER) formulations were available before the start of trial. Concerta® is based on an osmotic release system (OROS technology) with a distribution of IR:ER of 22:78 and is considered the longest-acting MPH (Modi et al. 2000). The advantage is a prolonged efficacy that also covers the afternoon. A downside of this distribution is the low concentration and low peak of MPH in the school hours. The efficacy of Concerta® has been demonstrated in various clinical trials (Wolraich et al. 2001; Swanson et al. 2003; Wilens et al. 2005). Medikinet® Retard is currently licensed only in Germany and some other European countries. It contains IR pellets as well as enteric-coated pellets with a 50:50 distribution. The efficacy of Medikinet® Retard has only been demonstrated against placebo and IR MPH (Doepfner et al. 2003; Doepfner et al. 2004). The third licensed formulation is Equasym® Retard (in the United States known as Metadate® CD), which uses a 30:70 distribution. The clinical profile is closer to Concerta®, with a rather low release of MPH during early school hours but a long duration due to the 70% ER part. Efficacy of Equasym® Retard has also been demonstrated in large studies against placebo and IR MPH (Findling et al. 2006; Greenhill et al. 2002).
Ritalin® LA is a modified-release formulation specifically engineered to deliver a bimodal release of MPH to mimic a twice-a-day (b.i.d.) MPH administration regimen (Lyseng-Williamson and Keating 2002). It uses the SODAS® technology composed of 50% IR and 50% ER release beads. The delayed release is mediated via a polymer coating. This robust delivery system offers several advantages, including an independence of food intake (Lee et al. 2003; Haessler et al. 2008) in contrast to Medikinet® Retard, which has to be administered after a full breakfast. The efficacy of Ritalin® LA has been demonstrated against placebo (Biederman et al. 2003) as well as against Concerta® (Lopez et al. 2003; Silva et al. 2005). Ritalin® LA is currently licensed in the United States as well as in several European countries.
The current study was performed to gain regulatory approval and marketing authorization in Germany. The primary objective of the study was to show superiority of treatment with 20 mg of Ritalin® LA once daily versus placebo and to demonstrate noninferiority against treatment with 20 mg of Medikinet® retard in the first 4.5 hours following administration.
Methods
Study design
The study was conducted in a double-blind, randomized, multicenter, triple crossover design in eight study sites in Germany. All investigations were carried out according to European Union legislation and Good Clinical Practice (GCP) requirements and were approved by the respective independent ethics committees before initiation of the study. Written informed consent or assent was obtained from both the child and the parent or legal guardian. The trial has also been registered in the database clinicaltrials.gov (Identifier NCT00254878).
The study design consisted of a prerandomization phase and three treatment periods of 7 days each (see Fig. 1 for details).
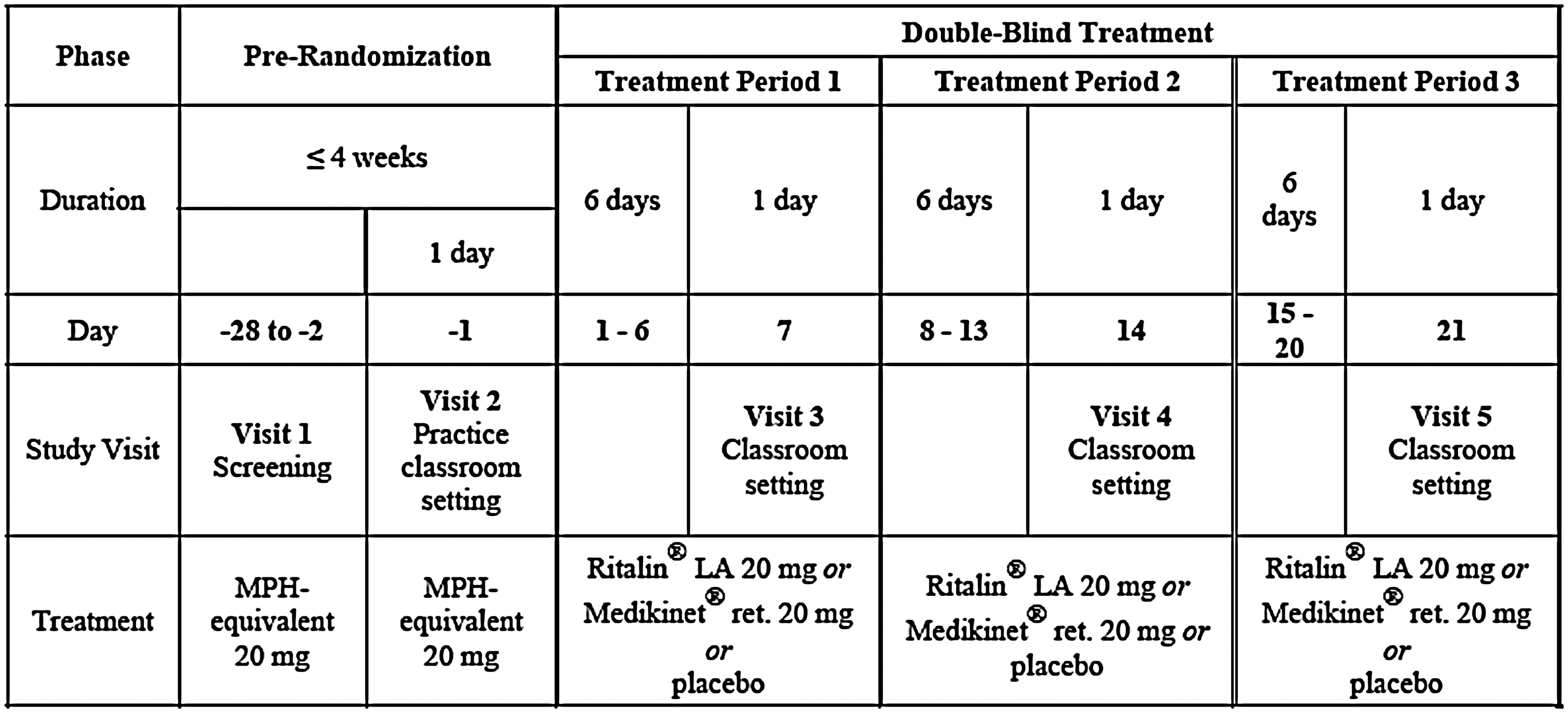
Study outline.
At the end of each 7-day treatment period, a laboratory classroom setting was applied to assess efficacy. Patients were randomized into one of six possible sequences receiving Ritalin® LA 20 mg, Medikinet® Retard 20 mg, and placebo. No washout periods were conducted due to the short half-life of all agents that do not lead to relevant accumulation. Randomization was centrally generated with a validated system that automated the random assignment of treatment sequences to randomization numbers in a specified ratio. All treating physicians, other site staff, and patients, as well as data analysts and Novartis in-house personnel, remained blinded from the time of randomization until database lock. The raters also did not have access to information about adverse events to maintain the blind. Patients with known previous nonresponse to MPH were excluded from the study.
Study population
The study population consisted of children aged 6–14 with a diagnosis of ADHD according to Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) criteria (American Psychiatric Association 1994). The diagnosis was confirmed by a structured diagnostic interview, the Kiddie Schedule for Affective Disorders and Schizophrenia (K-SADS) in the German version (Delmo et al. 2000). All children had to be on a stable and well-tolerated dose of a 20-mg dose equivalent MPH for at least 1 month prior to screening. Children with relevant somatic or psychiatric co-morbidities requiring pharmacological treatment (e.g., psychosis, major depression) were excluded. Patients with co-morbidities like oppositional defiant disorder (ODD), anxiety disorders, or other psychiatric conditions were allowed to participate in the study according to the judgment of the principal investigator. Concomitant medication, like antidepressants, antipsychotics, or non-MPH stimulants, had to be stopped before at predefined time intervals prior to randomization: Tricyclic antidepressants, buproprion, clonidine, buspirone 2 weeks; atomoxetine 2 weeks; fluoxetine or other antipsychotics 1 month; pemoline and other amphetamines 1 week before randomization.
Patients with warnings according to the prescribing information for Ritalin® LA, including tic disorders, were also excluded. No rescue medication was allowed during the study. Predefined concomitant medications known to interfere with the study medication were not allowed during the double-blind treatment phase. Drug accountability was recorded by monitors.
Medication
Ritalin® LA and Medikinet® Retard were obtained as ready-to-use medication. To ensure blinding of the study, all capsules were overencapsulated in an identical optical design. Overencapsulation was carried out by Allphamed Pharbil Arzneimittel GmbH (Göttingen, Germany). Medication intake during the study was in the morning and was supervised by the parents during normal week days; on classroom days, drug intake was at 9 a.m. and was supervised by study personnel.
Rating scales
The laboratory classroom setting was originally designed to investigate relationships between pharmacokinetic parameters and pharmacodynamic effects as well as clinical efficacy (Swanson et al. 2002). The primary output of the classroom setting is the Swanson, Kotkin, Agler, M-Flynn, and Pelham (SKAMP) score (Wigal et al. 1998). SKAMP is a rating scale designed to specifically measure the behavioral manifestations of ADHD in a simulated classroom setting. Ratings were based both on the frequency as well as the quality of behaviors. The scale was rated by three treatment-blinded observers in the classroom who were specifically trained on the SKAMP scale (psychologists, medical doctors, medical students). To ensure consistency, all SKAMP raters had to observe the same group of children at each session. A total of 13 items were rated from 0 (minimal) to 6 (maximum), and mean scores were calculated for every SKAMP session (SKAMP Combined score) as well as for two subscales focusing on inattentive symptoms and hyperactive/impulsive symptoms. The primary parameter was set to the mean SKAMP Combined score over the first three ratings at 10:30 a.m., at 12:00 a.m., and at 1:30 p.m. Secondary objectives included further SKAMP Combined scores at 6 and 7.5 hours as well as a differentiated evaluation of the two subscales for each time point.
All children were familiarized with the setting at baseline and underwent a practice classroom day. Laboratory classroom days started with a generous breakfast buffet because Medikinet® Retard may only be used after a thorough breakfast intake (SPC Medikinet Retard). After that, the predose session was conducted and medication was taken under supervision. SKAMP scores were rated 1.5, 3.0, 4.5, 6.0, and 7.5 hours after drug intake. Each SKAMP session consisted of a math test (10 minutes) and a group game (10 minutes). Efficacy of academic achievement was assessed by a standardized paper-and-pencil math test (Swanson et al. 1998). The test consisted of several pages with 100 math problems each. Problems were presented in ascending difficulty requiring addition, subtraction, multiplication, and division calculating skills. Children were initially sorted into four categories differing by the number of digits per calculation (basic, easy, moderate, difficult) considering intraindividual varities due to age, intelligence quotient (IQ), and calculation abilities. For all future assessments, math tests of an appropriate matching level were used for every child. The number of attempted problems and number of correctly solved problems were evaluated at each session as a surrogate for academic productivity. The Nisonger Child Behavior Rating Form (NCBRF-TIQ) is a well-validated test to assess behavior in children (Aman 2002). It consists of a single-positive social subscale (10 items) and a disruptive behavior scales with a total of 49 items. The NCBRF-TIQ was applied once at the end of each treatment period.
Safety assessments
Safety assessments consisted of monitoring and recording of all adverse events (AEs) sought by nondirective questioning at every visit as well as regular monitoring of vital signs. In the middle of every week, patients were additionally called by phone and asked for AEs. A complete physical examination was performed at baseline and a urine drug screening for other psychotropic drugs was performed. No further laboratory results were obtained. A clinical abnormality in blood pressure was defined as an increase or decrease of at least 20 mmHg from age-dependent norm values (age 6–9: systolic blood pressure [SBP] 90 mmHg, diastolic blood pressure [DBP] 60 mmHg; age >10: SBP 110 mmHg, DBP 75 mmHg).
Statistical analysis
SAS 8.2 was used for statistical analysis of the data. The efficacy analyses were performed comparing treatments in an analysis of variance (ANOVA) model with the factors center, period, patient within center, and treatment. Adjusted least squares (LS) means were provided as point estimates for all pairwise treatment contrast. Two-sided, 95% confidence intervals and p values for the null hypothesis of no treatment difference were calculated. For the comparisons between the two active treatments, an additional p value for the shifted null hypothesis that the difference exceeds the noninferiority margin in favor of Medikinet® Retard was provided.
The significance level was 5% two-sided (numerically equivalent to the one-sided 2.5% level, which is standard for noninferiority settings). To avoid inflation of the type 1 error level, multiple comparisons were hierarchically ordered a priori. A difference <0.25 points on the normalized SKAMP Combined scale was regarded as not clinically relevant and was therefore used as the noninferiority margin. This noninferiority margin was also discussed and agreed upon with the German Health Authority (BfArM) during a scientific advice session prior to study start. All randomized patients were included in the intention-to-treat (ITT) population. Missing values of the primary end point were replaced by the worst value observed in another patient under the same treatment at the same assessment time. For the noninferiority comparisons, the per-protocol (PP) population consisting of patients without major protocol violations was considered primary.
The sample size calculation for this trial was driven by the objective to prove the noninferiority of Ritalin® LA 20 mg versus Medikinet® Retard 20 mg. Assuming a true treatment difference of 0 (mean points, normalized SKAMP Combined scale) and a residual standard deviation (SD) of the (within-patient) differences of 0.75, 97 patients were required to achieve a power 90% to exclude a difference >0.25 in favor of Medikinet® Retard 20 mg on a one-sided significance level of 2.5%. To compensate for some dropouts and other protocol violations, 130 patients were planned to be randomized into this trial.
Results
Population
A total of 147 patients were enrolled into the study. Only 1 patient discontinued the study prematurely due to withdrawal of consent. All patients qualified for analysis in the ITT population. Eight patients had to be excluded from the per protocol (PP) population (see Fig. 2). Study patients were on average 10 years old, and a low proportion of patients were aged 13 and above. More males than females (81% vs. 19%) participated, which is in line with the prevalence of the disease. With 55%, the majority of patients suffered from a combined type ADHD according to DSM-IV. Symptoms had been present for approximately 6 years (median) before entering the study, and an appropriate diagnosis of ADHD was made approximately 2 years (median) before entering the study. Further demographic information is presented in Table 1. The distribution of ADHD subtypes in the sample is consistent with the literature of ADHD clinical samples: 80 patients (54.4%) have been on extended-release MPH formulations, 55 (37.4%) on immediate-release MPH, and 12 (8.2%) on other/combination of ER and IR. One patient had received atomoxetine in the past but without the specified washout period of 2 weeks and was not elegible for this study.
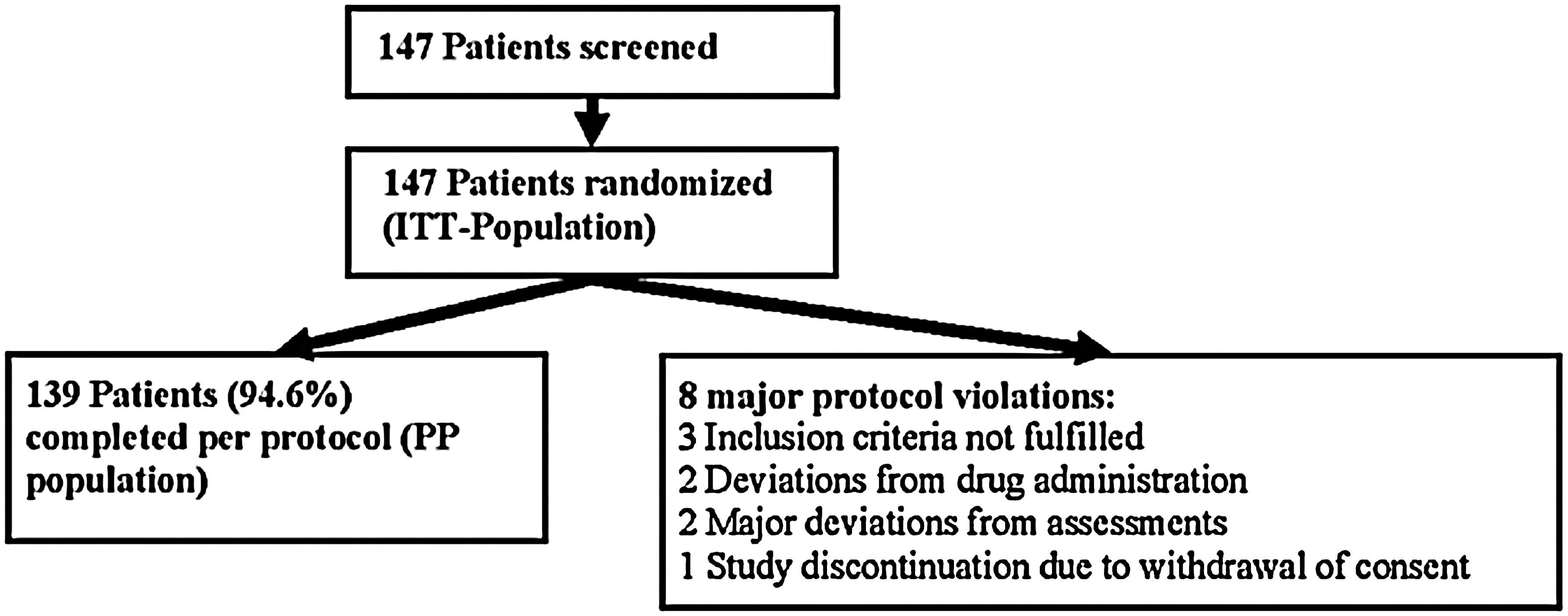
Patient disposition.
SD = standard deviation; ADHD = attention-defict/hyperactivity disorder.
Psychiatric comorbidities included disturbance in social behavior (n = 4), initial insomnia (n = 2), oppositional defiant disorder (n = 2), dysphemia (n = 1), encopresis (n = 1).
Efficacy
The difference between the SKAMP Combined scores of both the Medikinet® Retard and Ritalin® LA treatment period compared to placebo was statistically significant for all measurements (p < 0.0001), indicating a statistical and clinical superiority over placebo. The observed difference in the SKAMP Combined scores between Ritalin® LA and Medikinet® Retard as well as the respective confidence interval (CI) did not exceed the predefined noninferiority margin of 0.25 points (p = 0.0003). This demonstrates that the difference must be regarded as not clinically relevant. The observed difference in the SKAMP Combined scores between Ritalin® LA and Medikinet® Retard as well as the respective CI did not exceed the predefined noninferiority margin of 0.25 points (point estimate for the difference: d = 0.07, 95% CI, −0.17 to +0.03, one-sided p value that the difference exceeds the noninferiority margin: p = 0.0003).
All SKAMP Combined rating values are presented in Table 2. Low SKAMP scores indicate clinical improvement. Under placebo, the SKAMP Combined score deteriorated continuously until 4.5 hours after drug intake, remaining quite stable afterward but on an increased severity level compared to baseline. Both active treatment groups demonstrated comparable improvements until the maximum effect reached at 3 hours following drug intake. A slight worsening was noted afterward, with the Ritalin® LA group being slightly more affected. However, the worsening stopped after 6 hours in the Ritalin® LA group and seemed to continue in the Medikinet® Retard group to the final assessment. In both active treatment groups, the final SKAMP Combined scores after 7.5 hours were still below the baseline values before treatment. The course over time of the SKAMP Combined score for all treatment arms is shown in Fig. 3. The secondary parameters showed similar outcomes. Both SKAMP subscales closely followed the patterns of the SKAMP Combined score (data not shown). Stratified exploratory subgroup analyses pointed out a superior tendency for Ritalin® LA in the group of children with primarily hyperactive/impulsive ADHD, of children aged >12 years and in females. However, the respective subgroups were too small to detect a significant difference.
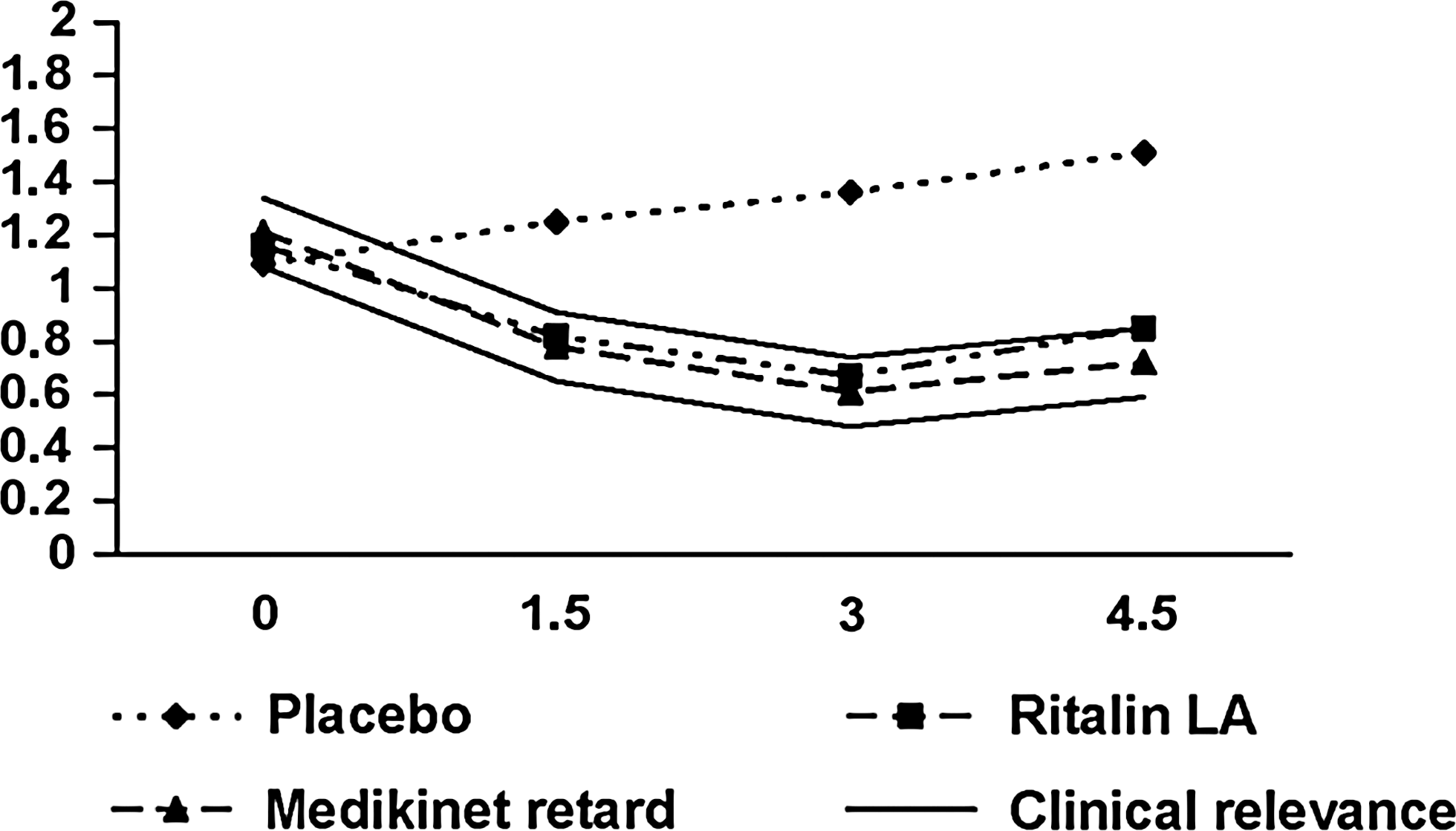
Swanson, Kotlin, Agler, M-Flynn, and Pelham (SKAMP) Combined Score over the first 4.5 hours following drug administration. Low SKAMP scores correlate with better clinical outcome. The “clinical relevance” lines outline the predefined noninferiority margin.
All analyses between Ritalin® LA and Medikinet® retard were carried out in the per = protocol population while for all other comparisons the intent-to-treat (ITT) population was used. Pair-wise comparisons are based on an ANOVA model with factors center, period, treatment and subject (center).
All p-values (diff = 0) from two-sided test for superiority.
P-value (diff = −0.25) from one-sided test for non-inferiority of Ritalin® LA compared to Medikinet® retard.
SKAMP, Swanson, Katkin, Agler, M-Flynn, and Pelham; LS, least squares.
The math tests (Table 3) followed a similar pattern, with a strong increase in both attempted and correctly solved math problems in both active treatment groups compared to a worsening in the placebo group. Peak efficacy was again reached at 3 hours and declined slightly afterward. A tendency toward a superior effect of Medikinet® Retard was observed during the later time points.
Pair-wise comparisons are based on an ANOVA model with factors center, period, treatment, and subject (center).
All p-values (diff = 0) are two-sided test for superiority.
Changes in the NCBRF-TIQ are presented in Tables 4 and 5. The positive social behavior measure remained stable in both active treatment groups and declined in the placebo arm. Medikinet® Retard and Ritalin® LA improved the disruptive behavior compared to the screening visit, whereas no changes were observed in the placebo group.
NCBRF-TIQ = Nisonger Child Behavior Rating Form; ITT = intention-to-treat.
Higher values indicate clinical improvement.
NCBRF-TIQ = Nisonger Child Behavior Rating Form; ITT = intention-to-treat.
Lower values indicate clinical improvement.
Safety
All study medication was well tolerated throughout the study. No patient dropped out due to AEs. Only one serious adverse event (SAE) was reported, a case of acute appendicitis during treatment with Ritalin® LA. This SAE was judged to be not treatment related by the investigator and led to a complete recovery. Four events were reported as “severe” and drug related (two cases of “aggressive behavior” on placebo, one case of “aggressive behavior” on Medikinet® Retard, and one case of “lack of attention” on placebo). Of the 147 patients enrolled in the study, 90 patients (61%) experienced at least one AE. The AEs occurred on treatment with placebo in 38 patients (26%), on Ritalin® LA in 44 patients (30%), and on Medikinet® Retard in 44 patients (30%). Thus, the rates of AEs can be considered similar on all three treatments. Less gastrointestinal disorders were reported on placebo than on any of the two active treatments. Drug-related abdominal pain and anorexia seem to appear more frequently under Medikinet® Retard. The most frequently reported AEs are presented in Table 6.
AE = adverse event.
Only drug-related AEs are considered that occurred in ≥2% of patients.
Clinically notable increased values of SBP were recorded under all three treatments (15% on placebo, 17% on Ritalin® LA, and 18% on Medikinet® Retard). Abnormal increases in DBP were noted in 5% of the patients on placebo and Ritalin® LA and in 3% on Medikinet® Retard. Notably, the SBP had already been increased in 27% of all patients at screening and 23% of all patients at the first practice day. Abnormal values in SBP in patients that had normal values at screening and baseline were only recorded in 7 patients (3 on placebo, 3 on Medikinet® Retard, 2 on Ritalin® LA).
Discussion
Long-acting MPH agents are considered one of the cornerstones of a multimodal treatment for ADHD. It has been shown that long-acting agents in general lead to a better therapy adherence than IR MPH (Marcus et al. 2005). Currently available preparations differ with respect to their galenic formulation, the amount of IR versus ER MPH, their pharmacokinetic profiles, their dependence on food intake, and their clinical efficacy profile (Wolraich and Doffing 2004), and these properties should be considered in the choice of an appropriate agent for an individual patient (Banaschewski et al. 2006).
The study was designed as a pivotal study for obtaining commercial registration for Ritalin® LA in Germany. The SKAMP scale can be considered a gold standard in the assessment of clinical efficacy for ADHD medications, and the period between 10:30 a.m. and 1:30 p.m. adequately reflects the crucial part of the day for most children. The laboratory classroom design provides a controlled study environment that serves as a surrogate measure for the community school classroom setting. It is a well-known concept in the assessment of efficacy for MPH and has been applied in multiple studies before (Pelham et al. 2001; Lopez et al. 2003; Swanson et al. 2004; Silva et al. 2005). The design allows for comparisons both against placebo and standard therapy. Due to the stable nature of the condition and to the short half-life of MPH, a crossover design allows for unbiased and precise estimation of treatment effects. All design aspects have been discussed and agreed upon with the German Health Authority (BfArM) during a scientific advice session prior to study start.
Superiority against placebo in the SKAMP Combined scale could be demonstrated for both Medikinet® Retard and Ritalin® LA, as expected. These findings are in line with previous studies for both Medikinet® Retard (Doepfner et al. 2004) as well as Ritalin® LA (Lopez et al. 2003). For the predefined primary parameter, the noninferiority of Ritalin® LA treatment compared to Medikinet® Retard treatment could also be demonstrated. While a tendency in favor of Medikinet® Retard is observed throughout the whole treatment period, this difference must be regarded as clinically not relevant. The noninferiority margin used in this study was based on previous protocols using the SKAMP scale (Pelham et al. 2001) and is commonly accepted. Similar results were obtained from secondary parameters (SKAMP subscales and math tests).
One possible explanation for the observed differences might have been the encapsulation. Absolute treatment effects for Ritalin® LA on the SKAMP scale were smaller in this trial than in a different trial using comparable methodology but an open-label design (Lopez et al. 2003). One might speculate that the encapsulation might have altered the pharmacokinetic properties of Ritalin® LA capsules more than of Medikinet® Retard capsules, leading to different dissolution levels. Although dissolution tests have been carried out, slight differences in the release of MPH might already lead to a relevant affection of the clinical response. In this context, the observation that neither of the two treatments showed a second peak of efficacy in this study is interesting. Both treatments reached their peak of efficacy at 3 hours and declined afterward. However, it is possible that the observation time was too short to detect a second peak because at least the Ritalin® LA group showed a slight improvement between 6 and 7.5 hours in the SKAMP Combined score. Another possible explanation of the response pattern might be a potential “floor effect,” meaning that the extended release of the drugs might not present in the form of further improvements but rather as a maintenance of the efficacy, preventing the return to the predose level. This explanation is supported by the long duration of the treatment effects, which were still significantly better than placebo at 7.5 hours for both medications and numerically under the respective baseline values.
Treatment with Ritalin® LA and Medikinet® Retard were generally well tolerated. No patient had to discontinue due to AEs from the trial. Although almost every third patient was affected by at least one AE, almost all AEs were of mild intensity. Changes in vital signs were attributed to the sympaticomimetic effect of MPH and were not considered clinically relevant. The AE profile was in line with the well-known AEs for MPH treatment in general (Wolraich et al. 2007). No relevant difference between Ritalin® LA and Medikinet® Retard could be found regarding either the profile, frequency, or intensity of AEs.
The chosen study design has certain limitations. While a laboratory classroom setting is a precise method and closely resembles a real community classroom, the presence of many other children, all with ADHD, as well as other experimental factors might influence the behavior of the individual child. One limitation of the study is the lack of pharmacokinetic correlations. The pharmacokinetics of both agents have been compared before (Haessler et al. 2008), showing distinctive differences in the pharmacokinetic profile. However, encapsulation might alter the pharmacokinetics of the active substances. Therefore, plasma MPH levels obtained in parallel to efficacy designs would have been useful. Furthermore, only one dose (20 mg) has been investigated in this trial for each agent that did not consider the weight of the individual patient. It is known from other trials that higher doses do not necessarily always correlate with a better treatment effect or even show a linear clinical dose–response relationship (Silva et al. 2005).
Dose delivery also depends on the galenic formulation. For the SODAS™ technology used in Ritalin® LA, linear dose-proportional pharmacokinetics have been demonstrated for the active enantiomer dexmethylphenidate in a trial with single doses of Focalin® XR (Tuerck et al. 2007). Investigations concerning a dose proportionality for Medikinet® Retard have not been published. Individual dose titration as a standard approach in everyday practice was not allowed during this trial; therefore, the treatment response might not have been optimal for all children. The results of this trial might therefore be limited to a patient group treated with 20 mg.
For the interpretation of the study results, the breakfast conditions also have to be considered. Due to the limitation of Medikinet® Retard that is only to be administered after a full breakfast (SPC Medikinet Retard) due to a loss of the retardation in the fasted state (Haessler et al. 2008), a generous breakfast buffet was offered to all children and was readily used. The food intake was supervised by study personnel; however, the exact amount of food or calories was not documented for every child. Therefore, no exact correlations between food intake and individual clinical performance could be carried out. In everyday practice, children with ADHD often do not have adequate breakfast in the morning, either due to early pronounced symptoms or due to chronic loss of appetite, which is often observed under long-term stimulation treatment. There is some initial evidence from a preliminary small study that only half of all children have sufficient breakfast according to their parents (Oehler et al. 2007). The results obtained in this study therefore are valid only for children with normal breakfast intake. One other factor to be considered as a limitation is that all patients were known MPH responders. This was necessary to ensure the study objectives with regard to the efficacy. However, it might overestimate the treatment effect and the tolerability in the overall population, as no treatment-naïve patients have been included in this trial.
Conclusion
Although a tendency in favor of Medikinet® Retard was observed throughout the entire treatment period, this difference must be regarded as clinically not relevant. The noninferiority of Ritalin® LA treatment compared to Medikinet® Retard treatment was demonstrated by this study. Ritalin® LA is a new efficacious, safe, and well-tolerated treatment option. Compared with placebo, both Ritalin® LA and Medikinet® Retard demonstrated a robust treatment effect on core inattentive and hyperactive symptoms for up to 7.5 hours in children with ADHD in a laboratory classroom.
Footnotes
Disclosures
Eberhard Schulz received grants from BMBF, Eli Lilly, Janssen-Cilag, Novartis, Pfizer, and Shire. Christian Fleischhaker is on theAdvisory Board of Bristol-Myers Squibb. Philip Heiser received compensation for professional services from Janssen-Cilag, Novartis, and Shire. Klaus-Uwe Oehler received grants from AstraZeneca, Eli Lilly, Glaxo Smith Kline, Janssen-Cilag, Lundbeck, Medice, Novartis, Numico Research, Pfizer, Pierre Fabre Medicament, Sanofi-Aventis, Servier, and Shire. Frank Haessler is on the Advisory Boards of Eli Lilly GmbH Germany and Janssen-Cilag; has received research support from Eli Lilly GmbH Germany, Janssen-Cilag, Novartis Pharmaceuticals, and Bayer Vital; has received travel grants from Novartis Pharmaceuticals, AstraZeneca Pharmaceutical, and UCB; has received consulting fees from Janssen-Cilag, Novartis Pharmaceuticals, and UCB; and has received honoraria from UCB. Andreas Warnke has received grants for scientific presentations, pharmacological research, and scientific meetings from Astra-Zeneca, Eli Lilly, Janssen Cilag, Medice, Novartis, Sanofi, Shire, Solvay, and UCB. Michael Huss currently receives grants from BMBF, BMFT, Eli Lilly, Engelhard-Arznei, Medice, Novartis, Shire, and Steiner-Arznei. Michael Schulte-Markworth received grants from AstraZeneca, BMBF, Bristol-Myer Sqibb, DFG, Eli Lilly, and UKE. Martin Schmidt received grants from Eli Lilly, Janssen-Cilag, and Novartis. Christian Sieder, Jan Klatt, and Ferenc Tracik, are employees of Novartis Pharma GmbH, Germany. Klaus Hennighausen and Martin Linder do not have any relationship to a pharmaceutical company.
The study data were analyzed by Christian Sieder (employee of Novartis Pharma GmbH, Germany). The paper was written by the stated authors. No external medical writer was involved.
Acknowledgments
The authors would like to thank all participating co-investigators and assistant personnel involved in the CRIT124DDE01 trial.
The statistical consultant for this study was Christian Sieder, Novartis Pharma GmbH, Germany.
Novartis Pharma GmbH, Germany, is the manufacturer of Ritalin LA, supplied the drug and financed the study.