
Abstract
Recent preclinical data have raised the possibility that prepubertal treatment of attention-deficit/hyperactivity disorder (ADHD) with stimulant medication might increase risk for later depression. The current longitudinal study investigated whether children with ADHD who were treated with stimulant medication displayed heightened levels of adolescent depression. Adolescents diagnosed with ADHD during childhood who had received a minimum of 1 year of treatment with stimulant medication were compared to adolescents with a childhood history of ADHD who were never treated with stimulants and a demographically matched comparison group on self-reports of depressive symptoms and diagnoses of depressive disorders. Both subgroups with childhood ADHD reported significantly higher dimensional ratings of depression and categorical rates of depressive disorders relative to the comparison group (all p < 0.05), yet those who were and were not medicated did not differ from one another. Results indicate that, while childhood ADHD increases risk for adolescent depression, stimulant treatment for ADHD neither heightens nor protects against such risk.
Introduction
Externalizing disorders, such as oppositional defiant disorder (ODD) and conduct disorder (CD) are the most frequently occurring co-morbid disorders and have been a major focus of empirical attention (Barkley et al. 1990; Gittleman et al. 1985; Loeber et al. 2000; Elia et al. 2008). Although co-morbidity of ADHD with internalizing disorders has been studied less extensively, a substantial proportion of children with ADHD also meets formal criteria for mood and anxiety disorders, and many continue to exhibit clinically significant symptoms during adolescence and adulthood. It has been reported that as many as 75% of youths with ADHD meet formal diagnostic criteria for a mood disorder at some point in their lifetime (Biederman et al. 1991; Spencer et al. 1999), as distinct from patterns of demoralization stemming from ADHD (Biederman et al. 1998); however, most estimates (20–30%) (Jensen et al. 1993; Fischer et al. 2002; Cuffe et al. 2001) have been considerably lower. With respect to anxiety disorders, the rate of co-occurrence with ADHD, on average, is about 25% (Tannock 2000).
Irrespective of the presence or absence of co-morbidity, a substantial proportion of individuals diagnosed with ADHD is treated with stimulant medications, which are considered to be a first-line treatment (Andersen et al. 2004). According to the National Survey of Children's Health of 2003, 56% or 2.5 million children ages 4–17 diagnosed with ADHD are treated with stimulant medication (Centers for Disease Control 2005). Other estimates indicate that as many as 4 million children are prescribed stimulant medications in the United States alone (Connor 2002). Stimulant treatment rates in both children and adults continue to increase, with a large body of evidence supporting the safety and efficacy of stimulants (Castle et al. 2007). In addition to mitigating the core features of ADHD (i.e., inattention, hyperactivity, and impulsivity) (Spencer et al. 1996), stimulants have been found to improve relationships with parents and peers and to decrease the severity of concomitant externalizing behaviors (e.g., aggression and oppositionality) (Wolraich 2003). However, the degree to which stimulant medications are also helpful for alleviating internalizing symptoms in children with ADHD has been less systematically evaluated.
The Multimodal Treatment of Attention Deficit Hyperactivity Disorder (MTA) study was designed to examine treatment response of children randomly assigned to routine community care or treatments provided by the study, which included medication (methylphenidate [MPH]) management, psychosocial (behavioral) treatment, or the combination of the two. The MTA 24-month follow-up results indicated that, although both medication and combined treatment were effective in reducing ADHD symptoms, symptoms of internalizing disorders (anxiety, depression) were most effectively alleviated by combined treatment (Jensen et al. 2001). However, treatment groups did not differ significantly on any measure 12 months later (Jensen et al. 2007). Such discrepancies may have been attributable to an age-related decline in ADHD symptoms, changes in medication management intensity, initiation or mediation of psychopharmacological treatment, or other factors. Results of the MTA 6-year follow up reported that participants who received behavioral treatment had lower rates of depression and anxiety compared to those in the medication management, combined treatment, or community care groups (Molina et al. 2009). However, there were no significant effects of treatment on any of the outcome variables at 8-year follow up (Molina et al. 2009).
Throughout the past several years, a series of animal studies has suggested that preadolescent exposure to MPH may be associated with behavioral changes in adulthood, including decreased sensitivity to rewarding effects of cocaine, sucrose, and sexual behavior (Andersen et al. 2002; Bolaños et al. 2003; Cornish and Kalivas 2001; Mague et al. 2004), characteristics deemed potentially analogous to anhedonia. In line with these findings, a study by Carlezon and colleagues (2003) showed that early exposure to MPH increased depressive-like behavior in adult rats. These investigators administered MPH to rat pups during preadolescence (postnatal days 20–35, corresponding to ages 4–12 years in humans), and examined a number of behavioral responses in the same animals during adulthood (postnatal days 36–60). Depressive-like effects were assessed using a forced swim test (FST), an animal model for depression, during which animals were forced to swim under inescapable conditions. Whereas antidepressant treatment blocks the “immobility posture” normally adopted by animals during FST, early MPH exposure was found to increase immobility posturing, suggestive of depressive-like behavior. MPH-exposed animals also had decreased sensitivity to cocaine and lower locomotor activity compared to saline-treated rats, effects commonly associated with dysphoria and anhedonia. Altogether, preadolescent treatment resulted in what the investigators described as prodepressant changes in behavior that persisted into adulthood. Nevertheless, the extent to which these animal models truly represent the depressive state in humans is difficult to ascertain.
To date, there have been two human studies that have examined the relationship of stimulant medication treatment to depression in youths with ADHD. The first study by Daviss et al. (2008b) provided preliminary evidence that pharmacological treatment for ADHD may be protective against later depression. This study compared ADHD youths with and without a history of depression with regard to lifetime medication treatment. Participants were recruited in adolescence (ages 11–18 years), and information about prior treatment and early symptoms was obtained via retrospective recall. They found that those with a history of ADHD + depression were less likely to have been treated with stimulant medication relative to ADHD youth without a history of depression. However, the study did not directly compare individuals with ADHD who were and were not treated with stimulant medication in childhood. As such it only indirectly addressed the question as to whether early stimulant treatment is associated with later depression.
The second study by Biederman et al. (2009) provided more direct evidence for the “protective” effects of stimulant treatment against later depression. The study is notable for its 10-year prospective design and diagnostic assessments at multiple time points, as well as the direct comparison of individuals with ADHD with and without a history of stimulant treatment. However, a substantial portion of the sample (29%) met criteria for major depressive disorder (MDD) at baseline, making it difficult to ascertain the extent to which childhood treatment impacts upon the emergence of depression. Also complicating the interpretation of findings is the fact that participants with ADHD who were diagnosed with depression prior to the onset of stimulant treatment were included in the “no treatment” group, which could serve to inflate the rate of depressive outcomes in the “no treatment” group. Finally, the samples in both of the above-mentioned studies were almost exclusively comprised of Caucasian middle-class participants, and, as such, may not be fully representative.
The current study was designed to further determine the impact of early psychostimulant treatment on the emergence of later depressive disorder. This initiative was undertaken by prospectively following a cohort of individuals diagnosed with ADHD during childhood and reexamining their psychiatric status during adolescence. Participants included individuals with varied histories of stimulant treatment, as well as those who did not report any medication treatment. A comparison group was recruited from the community that was similar to the ADHD group on most demographic parameters, but never had ADHD. The longitudinal design of the study coupled with clearly defined co-morbidity profiles during childhood provided a unique opportunity to control for childhood mood disorders. Moreover, detailed treatment history data allowed for a comparison of mood disorder outcomes of medicated and unmedicated ADHD groups in relation to a never-ADHD comparison group to examine the effect of childhood stimulant treatment.
Method
Participants
Adolescent probands (n = 97) were initially referred to a study of ADHD between 1990 and 1997 when they were 7–11 years old (mean [standard deviation, SD] age at baseline = 9.09 [1.30] years), and were diagnosed with ADHD according to Diagnostic and Statistical Manual of Mental Disorders, 3rd edition, revised (DSM-III-R) or 4th edition (DSM-IV) (American Psychiatric Association 1987; American Psychiatric Association 1994) criteria (depending upon when they were recruited). They were initially screened for participation using the Inattention-Overactivity with Aggression (IOWA) Conners teacher ratings (Loney and Milich 1982) and parent ratings on the Child Behavior Checklist (CBCL) (Achenbach 1991). A final diagnosis was based upon parent reports on the Diagnostic Interview Schedule for Children (DISC) (Shaffer et al. 1989; Shaffer et al. 2000). During childhood, 76.8% of the children met criteria of ODD, 32.7% for CD, 31.6% for a mood disorder, and 10.2% for an anxiety disorder. The subgroups recruited via DSM-III-R and DSM-IV criteria were quite similar and did not significantly differ on parent or teacher ratings (all p > 0.05). Participants were recontacted as part of a prospective follow-up study on average 9.32 years after their initial evaluation (mean [SD] age at follow up = 18.45 [1.73] years).
Detailed accounts of prior psychopharmacological treatment based on reports from each participant and his/her parent were gathered during a clinical interview and, together with all available historical data, were used to construct treatment history narratives. Following the completion of the narratives, participants were rated on medication use with special attention paid to the type (stimulants, other psychotropic drugs, or both) and duration of treatment. Ratings were completed by four trained graduate research assistants, who worked in independent pairs. Reliability scores between the two teams ranged from 0.79 to 0.95. Cases that had discrepancies between the two rating teams were reviewed by all raters and a group decision was made regarding each participant.
Using information gathered from the medication history inventories, those with childhood histories of ADHD were classified as either medicated (ADHD-M) or unmedicated (ADHD-U). The ADHD-U group included adolescents who were never treated with stimulant medication (n = 28). The ADHD-M group was comprised of individuals who received stimulant treatment during childhood, defined as prior to the age of 12 years, for a period of at least 1 year (n = 50). Among those in the ADHD-M group, the mean (SD; range) duration of stimulant treatment was 5.56 (3.16; 1–12) years. Participants who received stimulant medication treatment for less than 1 year or only after the age of 12 years were eliminated from the study (n = 19). As shown in Table 1, the two ADHD groups did not differ in childhood CBCL ratings of externalizing or internalizing disorders as reported by parents, or in teacher ratings of aggression. However, the ADHD-M group had significantly higher baseline teacher ratings of inattention/overactivity, suggesting that medication treatment may have been related to greater severity of ADHD symptoms. The ADHD-M group was also significantly younger and had higher Full Scale Intelligence Quotient (FSIQ) scores. Three out of 28 children (10.7%) in the ADHD-U group and 5 out of 50 children (10.0%) in the ADHD-M group had a diagnosis of a mood disorder in childhood.
Abbreviations: ADHD-U = Attention-deficit/hyperactivity disorder–unmedicated; ADHD-M = Attention-Deficit/hyperactivity disorder–medicated; SD = standard deviation; SES = socioeconomic status; FSIQ = Full Scale Intelligence Quotient; CBCL = Child Behavior Checklist; IOWA = Inattention-Overactivity with Aggression.
Community comparison (CC; n = 85) participants were recruited as adolescents for the follow-up study from the same neighborhoods as ADHD probands and were required to have had no significant history of inattention, impulsivity, or hyperactivity, or a diagnosis or treatment for ADHD as assessed using a telephone screening interview with the ADHD module from the DISC (Shaffer et al. 1989; Shaffer et al. 2000). ADHD and CC groups were well-matched with respect to demographic variables, such as ethnicity, FSIQ, sex, socioeconomic status (SES), and age (see Table 2).
Abbreviations: ADHD-U = Attention-deficit/hyperactivity disorder–Unmedicated; ADHD-M = attention-deficit/hyperactivity disorder–Medicated; CC = community controls; SD = standard deviation; FSIQ = Full Scale Intelligence Quotient; SES = socioeconomic status.
This study was approved by the Institutional Review Boards of the participating institutions. Participants over 18 years old signed an informed consent. Parents signed written consent for participants under 18 years old, and youths provided written assent. Participants were compensated for time and travel expenses.
Procedures
At follow up, all participants received a comprehensive evaluation that included an array of semistructured psychiatric interviews and rating scales. Affective problems in adolescence were assessed both dimensionally and categorically. Dimensional ratings of depressive symptoms were ascertained via the Beck Depression Inventory, Second Edition (BDI-II) (Beck et al. 1996), a frequently used self-report measure. Categorical assessment was conducted using the Kiddie Schedule for Affective Disorders and Schizophrenia–Present and Lifetime Version (K-SADS-PL) (Kaufman et al. 1997) semistructured interview, which was administered separately to the adolescent and his/her parent by a trained clinician. Summary scores from the K-SADS-PL were used to formulate diagnoses, which took into account all available clinical information (i.e., parent reports, adolescent self-reports, and clinician impressions). For the K-SADS-PL, individuals were dichotomized into those who did and did not meet diagnostic criteria for a depressive disorder, operationalized for the current study as MDD, dysthymic disorder, or depressive disorder not otherwise specified (NOS). Adolescents were considered to have met criteria for a current mood disorder if they received a “probable,” “in partial remission,” or “definite” diagnosis of any of the above disorders, as defined by the K-SADS-PL.
Data analysis
One-way analysis of variance (ANOVA) was used to test for differences between ADHD-U, ADHD-M, and CC groups with respect to dimensional severity of adolescent depression, as assessed by the BDI-II. Post hoc analyses were carried out using the Tukey procedure. Chi square procedures were employed to compare the proportion of each group that met criteria for a depressive disorder as determined by the K-SADS-PL, both current and lifetime episodes. Given the racial imbalance among the groups, chi-squared procedures were used to compare rates of depressive disorders among white and nonwhite participants. Furthermore, rates of depression of depression were compared among the ADHD-M, ADHD-U, and CC groups among nonwhite participants. Subsequently, a separate analysis of covariance (ANCOVA) controlling for childhood age, FSIQ, and IOWA Conners I/O score (not available for the CC group) was used to compare the two ADHD groups (i.e., ADHD-U and ADHD-M). Chi-squared procedures were also used to compare rates of depressive disorders among ADHD participants who did and did not meet criteria for a mood disorder in childhood.
Results
As depicted in Fig. 1, a significant group difference was observed in adolescent BDI-II ratings (F = 9.61, p < 0.001). Post hoc analyses indicated that, at follow up, controls had significantly lower BDI-II scores than both ADHD groups, whose scores did not differ significantly from each other (mean [SD]ADHD-U = 9.12 [9.14]; mean [SD]ADHD-M = 10.13 [10.54]; mean [SD]CC = 4.39 [4.92]). Differences between the two ADHD subgroups remained nonsignificant after controlling for childhood age, FSIQ, and IOWA Conners I/O scores. Furthermore, among those with childhood ADHD, the duration of medication treatment did not significantly correlate with later BDI-II scores (r = 0.135, p < 0.10).
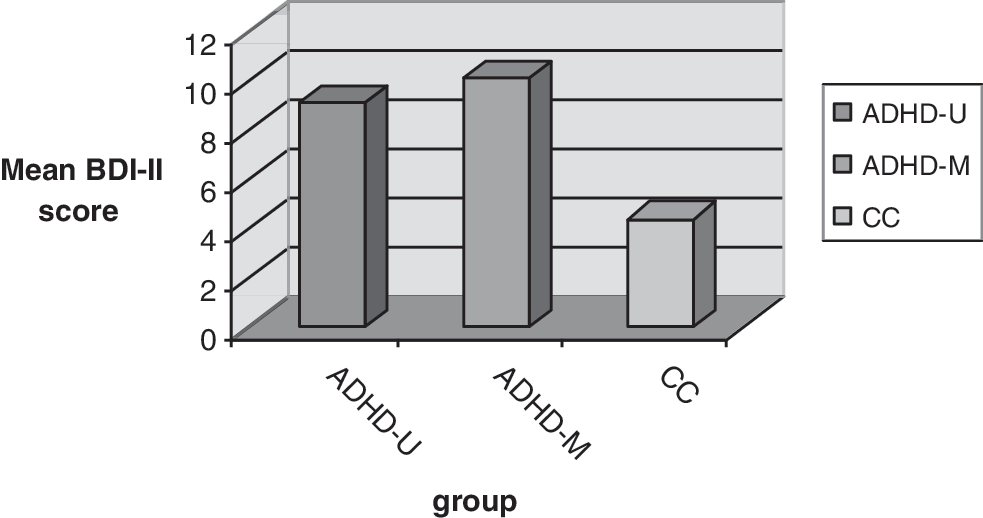
Both ADHD-U and ADHD-M participants reported significantly more symptoms of depressive disorders, compared to community controls on the BDI-II (F = 9.61, p < 0.001). ADHD-U = ADHD-M > Community controls; p < 0.001. ADHD-U = attention-deficit/hyperactivity disorder–unmedicated; ADHD-M = attention-deficit/hyperactivity disorder–medicated; CC = Community Controls; BDI-II = Beck Depression Inventory, Second Edition.
A similar pattern was evident using a categorical approach, with 17.9% of ADHD-U participants meeting criteria for a depressive disorder, compared to 18% of ADHD-M individuals and 4.7% of CC participants (χ2 = 7.26, p = 0.026; see Fig. 2). Follow-up testing revealed that the CC group differed significantly from both the medicated and unmedicated ADHD groups. Results were similar for the current and lifetime episodes of depressive disorders. The rates of depression did not differ among white and non-white participants (χ2 = 0.10, p = 0.75) or among ADHD-M, ADHD-U, and CC nonwhite youngsters.
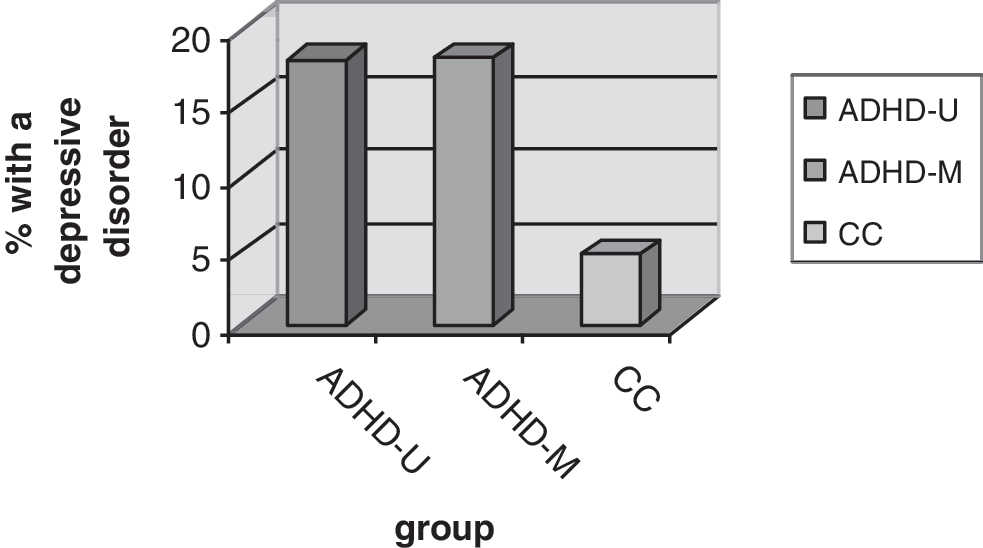
The percentage of participants who met criteria for depressive disorders was significantly higher for ADHD participants than controls (χ2 = 7.26, p = 0.026). There was no difference between ADHD-U and ADHD-M groups. ADHD-U = ADHD-M > Community controls; p < 0.05. ADHD-U = attention-deficit-hyperactivity disorder–unmedicated; ADHD-M = attention-deficit-hyperactivity disorder–medicated; CC = Community Controls.
Finally, among those adolescents with ADHD who met criteria for a depressive disorder, 25% also had a depressive disorder in childhood, compared to 6.5% among those who did not have a depressive disorder in adolescence (χ2 = 5.88, p = 0.029).
Discussion
The current study was designed to evaluate the extent to which childhood treatment with psychostimulant medication portends heightened risk for adolescent depressive disorder, as suggested by a prior study in animals (rats) (Carlezon et al. 2003), or serves to protect against later depression as suggested by some studies in humans (Daviss et al. 2008b; Biederman et al. 2009). Results of the present investigation did not support either of these positions. Children with ADHD who received treatment with stimulant medication for at least 1 year did not show higher dimensional or categorical levels of depression in adolescence compared to those who did not receive any stimulant treatment. Rather, youngsters with ADHD exhibited elevated levels of adolescent depression irrespective of whether or not they received such treatment.
The results of our study point to a dissociation between suggestive findings in animal models and data from humans. One possibility is that an animal model of depression does not adequately reflect adolescent depression. Variability and a change in the manifestation of symptoms over the life span are common in psychiatric disorders, including depression. For example, instead of dysphoria or anhedonia, adolescents may experience irritability, which may be attributed to adolescents' moodiness rather than depression.
In contrast to the findings of Daviss et al. (2008b) and Biederman et al. (2009), we did not find that childhood stimulant treatment protects against the emergence of adolescent depression. This may be due to several methodological differences across the studies. First, and perhaps most importantly, is the age range of the samples. Those in the Daviss et al. study were adolescents at the time of recruitment, and those in the Biederman et al. study ranged in age from 6 to17 years at the time of their baseline assessment. Such age variability could obfuscate the distinction between childhood and adolescent treatment, an issue of key importance to the animal models, which clearly focused on prepubertal medication administration (Carlezon et al. 2003). Stimulant treatment for all medicated children in our sample was initiated prior to the age of 12 years. Second, in contrast to the other studies, we had relatively lower rates of depression in childhood and at follow up. At least at follow up, this difference is likely attributable to the fact that we focused on current depression (defined as an episode within the past 6 months or current treatment for depression) rather than a lifetime history. This decision was made specifically because we were interested in following the paradigm of the animal models by examining depressive outcomes in adolescence, rather than whether the individual ever met criteria for depression (i.e., in childhood). However, rates of lifetime depression were similar to those of current depression. Third, a substantial portion of adolescents in the other studies were still being treated with stimulants. As such, it is possible that concurrent treatment has a positive effect on mood in adolescence, particularly when/if depressive symptoms are secondary to ADHD. In contrast, in our study, most participants were not being treated at follow up. Finally, our sample was quite ethnically and socioeconomically diverse, a key difference from the other studies.
The results of the present study should be interpreted in the context of several limitations. First, because the study constitutes a naturalistic follow up of ADHD probands (as opposed to a true experimental design), participants were not randomly assigned to medicated versus unmedicated conditions; thus, the results may have been affected by a self-selection bias, where parents of children with more severe psychopathology were more likely to try pharmacological treatment. However, comparisons across our medicated and unmedicated groups suggest only minimal differences in severity, and where baseline measures differed significantly, covariation did not alter the findings.
Second, while animal research has an advantage in that pubertal developmental stages in rodents have been established with precision, it is impossible to reach the same degree of accuracy in human research. Pubertal milestones are often highly subjective and vary substantially from individual to individual. In addition, pubertal status was not systematically assessed during childhood, so while a commonly adopted 12-year-old cutoff was used to define treatment in childhood, it is likely that some participants were pubertal prior to that age, and others were still prepubertal. It is also worth noting that the current study differed from that of Carlezon et al. in that some participants in the ADHD-M group were treated not only during childhood, but also received such treatment during adolescence. However, in all cases, treatment was initiated prior to 12 years of age.
Third, while the exact age of treatment onset is important in assessing treatment effects, based on retrospective parental reports, we could not reliably gauge the exact age at which participants began receiving treatment. However, we believe that using childhood or “prepubertal” treatment was appropriate for the purpose of this study.
Similar to the findings of others (Daviss, 2008b; Biederman et al. 2009), the results show that childhood stimulant treatment did not increase the likelihood of developing mood disorders in adolescence. As such, physicians and parents should not be hesitant about treating children with stimulant medication for ADHD because of concerns regarding the emergence of subsequent mood disorders. Consistent with reports from other investigators (Daviss 2008a), children with ADHD appear to be at heightened risk for adolescent depression regardless of whether they were depressed in childhood, and more so if they were depressed. Given the observed associations between depression, substance use, and suicidality (Kovacs et al. 1993; Currie et al. 2005), this finding has important implications for clinical practice and suggests that it is important to monitor adolescents with ADHD for other forms of psychopathology.
Future research should further examine the discrepancy among findings as to whether or not stimulant medication is protective against later depression. It may be that in contrast to treatment during childhood, adolescent treatment of ADHD symptoms with stimulant medication reduces the likelihood of an emergent depressive disorder or demoralization, which masks as depression. A mechanism for such an effect might be that the medication has a positive effect on academic and psychosocial functioning, thus reducing environmental stressors.
Disclosures
Dr. Newcorn is a recipient of grants for research support from Eli Lilly and McNeil Pediatrics; an advisor/consultant for Astra Zeneca, Eli Lilly, Novartis, Ortho-McNeil Janssen, Shire; and a speaker for McNeil Pediatrics. Dr. Halperin has consulted for Shire. The other authors have no financial relationships to disclose.
Footnotes
Acknowledgments
The authors would like to acknowledge Tobey Busch and Dana Barowsky for their help and support throughout this project.
This research was funded by grant # R01 MH060698 from the National Institute of Mental Health.