
Abstract
Objectives:
The aim of this study was to evaluate the efficacy of aripiprazole in the treatment of discrete symptoms of irritability associated with autistic disorder, as well as other symptoms captured on the Aberrant Behavior Checklist (ABC).
Methods:
This was a post hoc analysis of data from two 8-week, randomized, double-blind, multicenter trials to evaluate the efficacy of aripiprazole dosed flexibly (2–15 mg/day, n = 47) or fixed (5, 10,or 15 mg/day, n = 166) versus placebo (flexibly dosed, n = 51; fixed dose, n = 52). The effects of treatment on the 58 ABC items were evaluated.
Results:
Statistically significantly greater improvement was seen with aripiprazole versus placebo (p < 0.05) for all arms in both trials on the ABC–Irritability total subscale score and on the following individual ABC–Irritability items: Mood changes quickly, cries/screams inappropriately, and stamps feet/bangs objects. Several additional items measuring tantrum-like behaviors improved in the flexibly dosed trial and at least one arm of the fixed-dose trial (p < 0.05). Measures of self-injurious behavior, which had low baseline values, demonstrated numerical, but not statistically significant, improvement in both trials. Statistically significantly greater improvement in ABC Stereotypic Behavior and Hyperactivity total subscale scores was also consistent across all arms in both trials. In particular, there was a cluster of items related to hyperkinesis that were consistently sensitive to treatment.
Conclusions:
Aripiprazole is efficacious in the treatment of irritability in children and adolescents with autistic disorder, particularly with respect to symptoms associated with tantrum behavior.
Clinical trials information:
Analysis of Study CN138-179 (NCT00337571) and Study CN138-178 (NCT00332241).
Introduction
The primary focus of treatment should be to maximize functional independence and quality of life and alleviate family distress; these treatments may involve a combination of both behavioral and pharmacologic approaches. Although there are no approved medications to treat the core deficits of autistic disorder, associated behavioral disturbances may benefit from pharmacologic interventions, including the use of atypical antipsychotics (Posey et al. 2008). Risperidone and aripiprazole are approved by the U.S. Food and Drug Administration for the treatment of pediatric patients with irritability associated with autistic disorder, including symptoms of aggression toward others, self-injury, temper tantrums and rapidly changing moods (Aripiprazole 2009; Risperidone 2009).
Recently, the results from two 8-week, multicenter, randomized, double-blind, placebo-controlled trials demonstrated that aripiprazole is efficacious and generally safe and well tolerated in the treatment of children and adolescents with severe behavior problems associated with autistic disorder (Marcus et al. 2009; Owen et al. 2009). In both studies, the primary efficacy outcome was change from baseline in the Aberrant Behavior Checklist–Irritability subscale (ABC-I) (Aman et al. 1986) total score with treatment. The ABC-I total subscale comprises 15 items and includes behaviors such as injures self, physical violence to self, aggressive to other children and adults, irritable, temper outbursts, depressed mood, mood changes, and cries/screams inappropriately. Each item is rated on a scale ranging from 0 (not at all a problem) to 3 (severe). In both studies, all aripiprazole treatment arms resulted in significantly greater improvement compared with placebo on the mean change from baseline in ABC-I total subscale scores. In addition to evaluating changes in ABC-I total subscale scores, both studies also evaluated the change from baseline on the four other ABC total subscales (Lethargy/Social Withdrawal, Stereotypic Behavior, Hyperactivity and Inappropriate Speech) as secondary efficacy outcomes. Here, we report findings from an exploratory, post hoc analysis of data from these studies to evaluate more discretely which specific symptoms of irritability responded to treatment with aripiprazole. The effects of aripiprazole on other ABC subscale item scores were also evaluated.
Methods
This was an exploratory, post hoc analysis of data from two randomized, double-blind, placebo-controlled studies conducted at multiple sites within the United States. Both studies were conducted in accordance with the Declaration of Helsinki and received appropriate approval by the institutional review board or independent ethics committee. All parents/guardians provided written informed consent to participate and subjects provided written, informed assent when possible. Subjects were enrolled between June, 2006, and February, 2008, in the flexibly dosed study (Owen et al. 2009), and between June, 2006, and June, 2008, in the fixed-dose study (Marcus et al. 2009).
Study design and treatments
Details of the study design have been reported previously. Briefly, two 8-week, double-blind, randomized, placebo-controlled, multicenter studies were conducted to assess the efficacy, safety, and tolerability of aripiprazole in children and adolescents aged 6–17 years, inclusive, with irritability associated with autistic disorder. Both studies consisted of a screening phase (up to 42 days) followed by an 8-week double-blind treatment phase. In the flexibly dosed study, subjects were randomized (1:1) to treatment with aripiprazole (2–15 mg/day, target dose 5, 10, or 15 mg/day) or placebo. In the fixed-dose study, subjects were randomized to receive aripiprazole (5, 10, or 15 mg/day) or placebo in a 1:1:1:1 ratio. In both studies, aripiprazole was initiated at 2 mg/day for the first week and increased to 5 mg/day for the second week; dose increases in 5-mg increments (if deemed appropriate in the flexibly dosed study/to assigned dose in the fixed-dose study) occurred at weekly study visits. No dose increases were permitted in the flexibly dosed study after week 6 and no dose adjustments were permitted in the fixed-dose study at any point.
Subjects
Study inclusion and exclusion criteria were identical in the two trials. Subjects were aged 6–17 years, inclusive, who met Diagnostic and Statistical Manual of Mental Disorders, 4th edition Text Revision (DSM-IV-TR) criteria (American Psychiatric Association 2000) for autistic disorder and demonstrated behaviors such as tantrums, aggression, self-injurious behavior, or a combination of these symptoms. Diagnosis was confirmed using the Autism Diagnostic Interview–Revised (ADI-R) (Lord et al. 1994), which was administered by an experienced interviewer who had been previously trained and approved as “Research Reliable” on the ADI-R or who had been approved following successful completion of a 2-day rater training course conducted by an ADI-R–certified trainer. Subjects were also required to have a Clinical Global Impressions–Severity (CGI-S) score ≥4 (Arnold, et al. 2000) and ABC-I (Aman et al. 1986) total subscale score ≥18 at screening and baseline. Subjects were required to have a mental age greater than 18 months. Further details of the exclusion criteria have been reported elsewhere (Marcus et al. 2009; Owen et al. 2009).
Assessments and data analysis
Subjects were evaluated at the end of treatment weeks 1, 2, 3, 4, 5, 6, and 8, or at the time of early termination. The primary efficacy measure in these studies was the mean change from baseline to end point in the caregiver-rated ABC-I total subscale score (subscale I, 15 items). Additional secondary efficacy outcomes included the mean change from baseline in the following ABC subscale scores: Lethargy/Social Withdrawal (subscale II, 16 items), Stereotypic Behavior (subscale III, 7 items), Hyperactivity (subscale IV, 16 items), and Inappropriate Speech (subscale V, 4 items). All items are rated on a 4-point Likert scale ranging from 0 (not at all a problem) to 3 (the problem is severe in degree). Although prospective testing of cognitive ability was not systematically performed in these studies, cognitive ability was determined by clinical judgment using results from standardized tests or school performance records where available. Cognitive ability was classified as: Average/above average, borderline, mild-to-moderate impairment, or severe impairment.
All analyses were conducted on the efficacy sample, which included all patients randomized to treatment that took at least one dose of study medication during the double-blind treatment phase and had at least one post-randomization efficacy evaluation and corresponding baseline value. Adjusted mean change from baseline to end point (week 8) in ABC total subscale scores and individual items of the ABC were evaluated using the last observation carried forward (LOCF) data set, by analysis of covariance (ANCOVA), controlling for treatment, study center, weight category (<40 kg or ≥40 kg) and baseline value. To evaluate the potential clinical meaningfulness of the line item changes, we also calculated between-group (aripiprazole vs. placebo) effect sizes for both subscale scores. Individual items were also calculated by dividing the difference of treatment-specific mean estimates by the square root of the mean square error (MSE) from the corresponding ANCOVA model. An effect size of ≥0.8 is considered large, an effect size of ≥0.5 is considered moderate, and an effect size of ≥0.2 is considered small (Cohen 1988). All treatment comparisons are interpreted at the 5% significance level, and all findings reported as significant were statistically significant at this level. No adjustments for multiple comparisons have been applied since all analyses performed are considered exploratory in nature.
Results
Patient disposition and demographics
A total of 316 subjects were randomized to receive treatment with placebo (fixed-dose study, n = 52; flexibly dosed study, n = 51) or aripiprazole (fixed-dose study, n = 166; flexibly dosed study, n = 47) in these two studies. Subject disposition for individuals included in these studies have been presented previously. Overall, 77% of the flexibly dosed study subjects and 82% of fixed-dose study subjects completed the randomized, double-blind treatment phase; completion rates were similar between treatment arms in both studies. In the fixed-dose study, the most common reason for withdrawal in all treatment groups was adverse events (AEs): Placebo, n = 4 (7.7%); aripiprazole 5 mg, n = 5 (9.4%); aripiprazole 10 mg, n = 8 (13.6%); and aripiprazole 15 mg, n = 4 (7.4%). In the flexibly dosed study, the most common reason for withdrawal for aripiprazole was adverse events (10.6%) and for placebo, lack of efficacy (11.8%). In the flexibly dosed study, the distribution of aripiprazole dosing during the last week of treatment (n = 39) was as follows: 2 mg/day, n = 2 (5%); 5 mg/day, n = 13 (33%); 10 mg/day, n = 16 (41%); and 15 mg/day, n = 8 (21%).
Baseline characteristics of subjects included in each study are shown in Table 1; subject baseline characteristics by treatment arm have been presented previously (Marcus et al. 2009; Owen et al. 2009). In both studies, the majority of subjects was male aged 6–12 years; demographic characteristics were similar between aripiprazole and placebo groups in both studies. At baseline, more than two-thirds of patients had borderline, mild, or moderate cognitive impairment (69.6%); the remainder had either no impairment (21.6%) or severe impairment (8.8%).
Abbreviations: ABC-I, Aberrant Behavior Checklist Irritability subscale; SD, standard deviation.
ABC–Irritability total subscale and items
Aripiprazole produced significantly greater improvements in the mean change from baseline to week 8 on the ABC-I total subscale scores compared with placebo in both studies (Table 2). Adjusted mean change from baseline to week 8 in the 15 individual items on the ABC-I total subscale are shown in Table 2. Statistically significantly greater improvement with aripiprazole versus placebo (p < 0.05) was seen in the following ABC-I items in both trials across all treatment arms: Mood changes quickly, cries/screams inappropriately, and stamps feet/bangs objects. Significantly greater improvement with aripiprazole versus placebo (p < 0.05) was also seen in the flexibly dosed trial and at least one arm of the fixed-dose trial for these items: Aggressive toward others, screams inappropriately, temper tantrums, irritable, yells, demands must be met immediately, cries over minor hurts, and temper outbursts. Aripiprazole produced modest improvements in measures of self-injurious behavior (injures self, hurts him/herself, physical violence), but these improvements were not significantly greater than placebo in either study. However, it should be noted that baseline values for these self-injury items were lower than those that measured tantrum-like behaviors. Effect sizes for each of the ABC-I items are shown in Fig. 1, and most demonstrated a moderate-to-large effect of treatment.
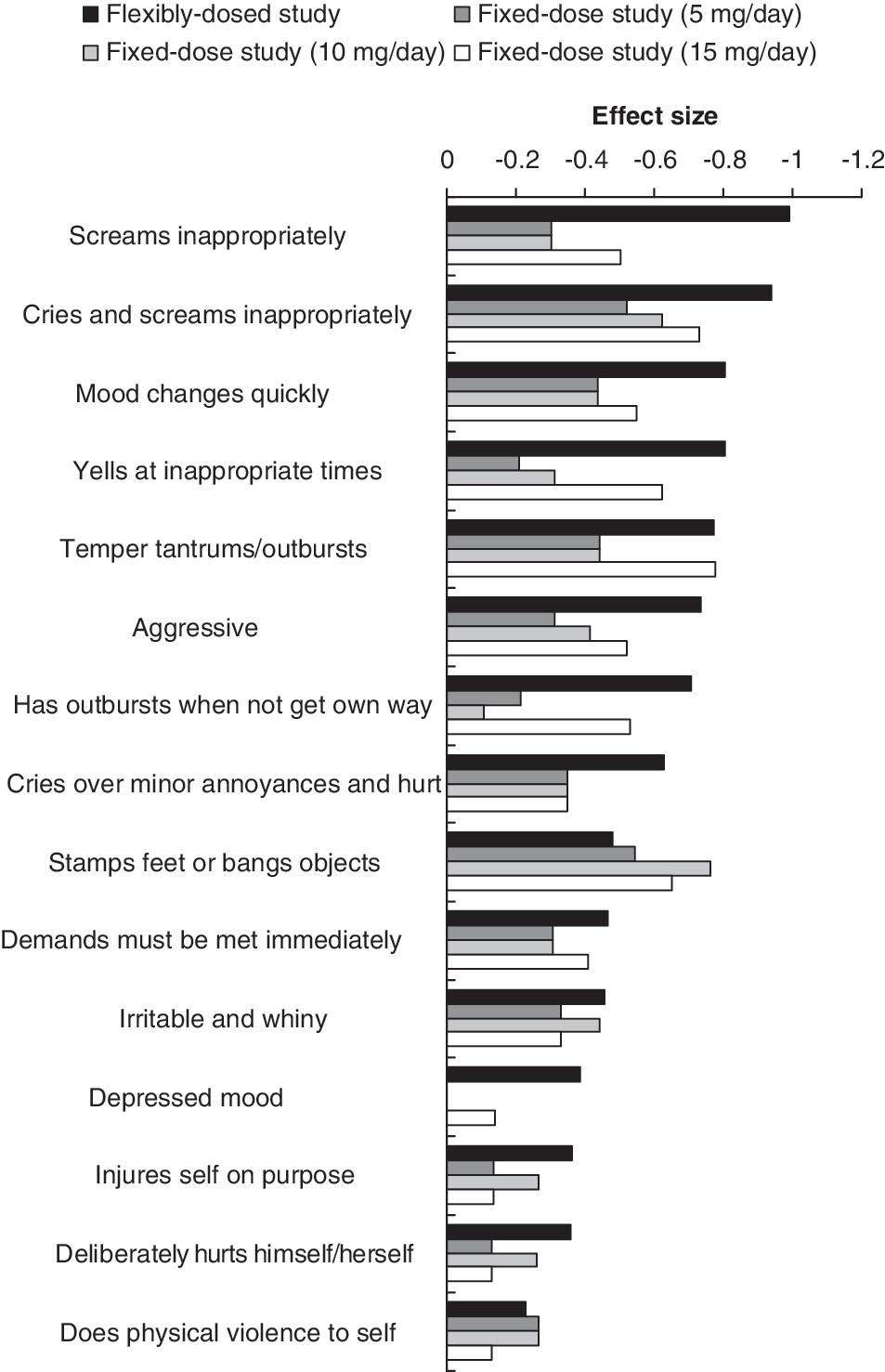
Effect sizes for Aberrant Behavior Checklist–Irritability subscale (ABC-I) items.
Shaded boxes, p < 0.05 versus placebo.
p ≤ 0.10 versus placebo.
Abbreviations: ABC-I, Aberrant Behavior Checklist–Irritability subscale; SE, standard error.
ABC Social Withdrawal total subscale and items
Aripiprazole did not demonstrate statistically significant improvements in the mean change from baseline to week 8 on the ABC Social Withdrawal total subscale scores compared with placebo in either study (see Table 3). Consistent with changes in the Social Withdrawal subscale score, repeated improvements on Social Withdrawal items were not seen with aripiprazole compared to placebo. Only one item (difficult to reach) resulted in statistically significant greater improvement with aripiprazole versus placebo (p < 0.05) in the flexibly dosed trial and at least one arm of the fixed-dose trial.
Shaded boxes, p < 0.05 versus placebo.
p ≤ 0.10 versus placebo.
Abbreviations: ABC, Aberrant Behavior Checklist; SE, standard error.
ABC Stereotypic Behavior total subscale and items
Aripiprazole produced significantly greater improvements in the mean change from baseline to week 8 on the ABC Stereotypic Behavior total subscale scores compared with placebo in both studies (see Table 3). Adjusted mean change from baseline to week 8 in the 7 individual items on the ABC Stereotypic subscale is shown in Table 3. One item—repetitive hand, body, or head movements—showed significantly greater improvement with aripiprazole versus placebo (p < 0.05) in both trials and across all treatment arms in the fixed-dose study. The ABC Stereotypic Behavior subscale item “moves or head movements” showed significantly greater improvement with aripiprazole versus placebo (p < 0.05) in both trials and across all treatment arms in the fixed-dose study. The ABC Stereotypic Behavior subscale items “odd, bizarre behavior” and “waves or shakes extremities” also produced greater improvements with aripiprazole than placebo in the flexibly dosed study and one arm (15 mg/day) of the fixed-dose study.
ABC Hyperactivity total subscale and items
Aripiprazole produced significantly greater improvements in the mean change from baseline to week 8 on the ABC Hyperactivity total subscale scores compared with placebo in both studies (see Table 3). Adjusted mean change from baseline to week 8 in the 16 individual items on the ABC Hyperactivity subscale is shown in Table 3. Significantly greater improvement with aripiprazole versus placebo (p < 0.05) was seen in the following ABC Hyperactivity items in both trials across all treatment arms: Boisterous, constantly runs or jumps, and tends to be excessively active. In addition, the following ABC Hyperactivity subscale items also showed significantly greater improvement with aripiprazole than placebo in the flexibly dosed study and at least one arm of the fixed-dose study: Excessively active; impulsive, acts without thinking; restless, unable to sit still; disobedient, difficult to control; uncooperative; disrupts group activities; does not stay in seat; will not sit still; easily distractible; pays no attention when spoken to; deliberately ignores directions. In addition, the ABC item “does not pay attention” produced significantly greater improvement with aripiprazole versus placebo in two treatment arms of the fixed-dose study.
ABC Inappropriate Speech total subscale and items
Aripiprazole produced significantly greater improvements in the mean change from baseline to week 8 on the ABC Inappropriate Speech total subscale scores compared with placebo in the flexibly dosed study and one treatment arm of the fixed-dose study (see Table 3). Only one item (talks excessively) produced significantly greater improvements with aripiprazole than placebo in the flexibly dosed study and at least one treatment arm of the fixed-dose study.
Discussion
Aripiprazole was previously shown to be effective at reducing irritability in children and adolescents with autistic disorder who also demonstrate irritability, aggression, self-injurious behavior, or a combination of these symptoms, as shown by statistically significantly greater improvement on the caregiver-rated ABC–Irritability total score compared with placebo in two placebo-controlled studies (Marcus et al. 2009; Owen et al. 2009). This exploratory analysis of the individual items of the ABC-I subscale from these studies provides the opportunity to review the discrete symptoms of irritability associated with autistic disorder and how these were affected by treatment with aripiprazole. The findings reported here suggest that improvements in irritability were due primarily to improvements in behaviors related to tantrums, including “rapid mood changes, cries/screams inappropriately, and stamps feet/bangs objects”; these items were significantly improved with aripiprazole treatment across both studies compared to placebo. This analysis also showed that aripiprazole resulted in improvements in other tantrum-like behaviors, including “aggressive toward others, screams inappropriately, temper tantrums, irritable, yells, demands must be met immediately, cries over minor hurts, and temper outbursts,” although these improvements were not consistently observed across all treatment arms in both studies.
Whereas tantrum-like symptoms improved with aripiprazole treatment, improvements in measures of self-injurious behavior, which had low baseline values relative to tantrum-like behaviors, did not show statistically significant improvement with aripiprazole compared to placebo, although numerical improvements were observed. As the basal rates of self-injury were quite low in this study, it is difficult to determine precisely the consistency and magnitude of aripiprazole's effects for these types of behaviors.
Aripiprazole also resulted in improvements in items related to excessive physical activity—for example, items such as “excessively active, boisterous, restless, unable to sit still, constantly runs or jumps, and tends to be excessively active”; all are individual items of the ABC Hyperactivity subscale. However, it is important to note that this study was not designed or intended to measure the effects of aripiprazole on items of hyperactivity per se and definitive conclusions regarding hyperactivity should not be drawn from this analysis. One item from the Lethargy/Social Withdrawal subscale “difficult to reach” also emerged as sensitive to treatment, which caregivers may have interpreted as reflective of less excessive physical activity-related behaviors in the active treatment groups. The same can be said of the only Repetitive Speech item to improve across studies, “talks excessively.” This has been observed to cross over to ratings of Hyperactivity in some psychometric studies (Marshburn et al. 1992). The tendency of both the Irritability and the Hyperactivity subscales to show the most consistent and marked therapeutic effects is also noteworthy for psychometric reasons; almost all factor analytic studies of the ABC have shown these two domains to correlate strongly and positively with each other (Aman et al. 1985; Marshburn et al. 1992; Brown et al. 2002).
Regarding the Stereotypic Behavior subscale, the item that showed the most consistent improvement across active treatments was “repetitive hand, body, or head movement.” Caregivers were less likely to report treatment effects for "stereotypic behavior" and “rocks body back and forth.”
Aripiprazole was generally well tolerated in these short-term studies (Marcus et al. 2009; Owen et al. 2009). In a post hoc safety analysis of pooled data from these two studies, the most commonly reported AEs (>10% of subjects) with aripiprazole (vs. placebo) were sedation (20.8% vs. 4.0%), fatigue (16.5% vs. 2.0%), vomiting (13.7% vs. 6.9%), increased appetite (12.7% vs. 6.9%), and somnolence (10.4% vs. 4.0%). Most AEs were mild or moderate and occurred early in treatment (Robb et al., unpublished). Although sedation and somnolence were commonly reported with aripiprazole treatment, both events tended to resolve over time. The median time to resolution was 19 and 23 days for sedation and somnolence, respectively (Robb et al., unpublished). Thus, it seems unlikely that the sedative effects of treatment would account for the improvement aripiprazole produced on several ABC line items at week 8. Furthermore, additional analyses of the potential effects of sedation and somnolence on efficacy, as measured using ABC-I subscale scores, showed no overall treatment effect.
As with all medical treatments, medication treatment for pediatric patients with irritability associated with autistic disorder should be considered as part of a total treatment program that includes psychological, educational, and social interventions. The decision to initiate medication treatment in children with irritability associated with autistic disorder should be made between health-care providers and caregivers only after a thorough diagnostic evaluation and discussion of both the benefits and risks. The purpose of this analysis is to provide data that can be used to help clinicians and caregivers to evaluate the appropriateness of aripiprazole therapy based on each individual's clinical symptom presentation.
The findings reported here should be considered in light of the post hoc and exploratory nature of these analyses, as neither study was powered to detect differences in individual ABC line items. Furthermore, analyses for each of the individual ABC items reported here did not include adjustments for multiple testing, and thus all significant values should be considered exploratory and with this limitation in mind. However, some level of reassurance may be derived by the tendency of comparisons to emerge as consistently significant across doses and studies for many items, as the likelihood of multiple significant findings across different dose groups is relatively small. It should also be considered that the majority of subjects in these studies was male, as would be expected based on the higher prevalence of autistic disorder in males than females. As such, the generalizability of our findings to a predominantly female population is unknown. Finally, this was also a short-term study and, although improvements in some ABC-items were seen during the 8-week study duration, the effects of aripiprazole on these symptoms longer term could not be evaluated in the present analysis.
In conclusion, the results of this post hoc analysis suggest that aripiprazole has its most consistent effects on symptoms associated with tantrum behavior. Improvement was also seen on items related to excessive physical activity. Interestingly, these symptoms have been observed to co-vary in past psychometric research.
Footnotes
Disclosures
Michael Aman was a consultant to and received grant support from Bristol-Myers Squibb.
Raymond Mankoski, George Manos, and Ronald Marcus are employees of Bristol-Myers Squibb, as was Randall Owen at the time of the study. Suja Mathew and William Kasper are employees of Otsuka America Pharmaceutical, Inc.
This study was supported by Bristol-Myers Squibb (Princeton, NJ) and Otsuka Pharmaceutical Co., Ltd. (Tokyo, Japan). Editorial support for the preparation of this manuscript was provided by Ogilvy Healthworld Medical Education; funding was provided by Bristol-Myers Squibb.