
Abstract
Background:
Patients receiving second-generation antipsychotics (SGAs) may experience secondary metabolic effects such as weight gain, as well as changes in lipid and glucose metabolism. These effects are well documented in adults; however, fewer studies are available concerning their occurrence and their evolution in children and adolescents.
Objective:
The aim of this study was to determine if there is an age-dependent variation in the metabolic effects of SGAs in a drug-naïve population.
Methods:
Charts of 232 French Canadian patients participating in a program monitoring the metabolic effects of SGAs were retrospectively reviewed. A total of 85 SGA-naïve patients were selected, including 58 youths and 27 adults. Changes, relative to baseline, in weight, body mass index, lipid metabolism (total cholesterol, low-density lipoprotein, high-density lipoprotein, and triglyceride), and fasting blood glucose were assessed, with follow-up at 3, 6, 12, and 24 months.
Results:
With respect to weight gain, in both the youth and adult groups, body mass index significantly increased from baseline at 3 months (10.1% [p < 0.0001] and 12.2% [p < 0.0001], respectively) and 6 months (11.8% [p < 0.0001] and 13.1% [p < 0.0001], respectively). With respect to lipid metabolism, in the youth group, there was no significant change. In the adult group, there was a significant increase at 3 and 6 months in total cholesterol (24.0% [p = 0.004] and 24.1% [p = 0.0006], respectively), low-density lipoprotein (26.8% [p = 0.019] and 30.1% [p = 0.010], respectively), and high-density lipoprotein (10.2% [p = 0.04] and 17.1% [p = 0.005], respectively). There was no significant change in triglyceride and glucose metabolism in both groups.
Conclusions:
Our results confirm the age-independent effects of SGA on weight gain. However, more data are needed to explore the age effect on glucose and lipid metabolism.
Introduction
Although, in the last 15 years, we have seen a steady increase in the number of SGA prescriptions written for children and adolescents (Alessi-Severini et al. 2008; Domino and Swartz 2008; Kalverdijk et al. 2008; Cascade et al. 2009; Schubert and Lehmkuhl 2009), there is little reliable data concerning the metabolic effects of this drug class in this population. Initially, reports on the metabolic effects of SGAs in children and adolescents were based primarily on case reports. Recently, a number of studies and trials have reported metabolic effects in youths on SGAs (Stigler et al. 2004; Toren et al. 2004; Fedorowicz and Fombonne 2005; Correll and Carlson 2006; Correll 2007; Jensen et al. 2007; Castro-Fornieles et al. 2008; Dittmann et al. 2008; Fraguas et al. 2008; Correll et al. 2009).
Similar to observations of weight gain in adults, these studies found that SGAs tend to induce weight gain in children and adolescents and that this propensity differs among SGAs (Stigler et al. 2004; Fedorowicz and Fombonne 2005). It is important to mention that earlier studies did not take into account the growth process occurring in children and adolescents by reporting only weight change in kilograms, although recent studies are using body mass index (BMI) or BMI Z-score (Reyes et al. 2006; DelBello et al. 2007; Schimmelmann et al. 2007; Kapetanovic et al. 2009). In fact, from childhood to the end of adolescence, there is a normal weight gain attributed to growth and a physiological increase in the BMI, which is taken into consideration by the age- and sex-adjusted BMI Z-score. Given the growth process, body composition change appears to be a more accurate concept than weight gain for describing the morphologic change that occurs in young patients treated with SGAs.
Similarly, there is no clear, accepted definition of clinically significant weight gain during development. However, a set of criteria for clinically significant weight changes has been recently suggested by Correll and Carlson (2006), namely a relative weight gain of 5% compared with baseline in the first 3 months of treatment and, for longer observation periods, an increase of ≥0.5 in the BMI Z-score.
To our knowledge, in the rare studies that have evaluated lipid levels in children and adolescents treated with SGAs (Shaw et al. 2001; Martin and L'Ecuyer 2002; Turgay et al. 2002; Sikich et al. 2004; Biederman et al. 2005a, 2005b), there was no significant change seen in youth populations, with the exception of two studies (Sikich et al. 2008; Correll et al. 2009).
With respect to the effects of SGAs on fasting blood glucose levels (FBG) in children and adolescents, here again, very few studies have been published (Fedorowicz and Fombonne 2005; Correll 2007; Sikich et al. 2008). Most studies that have assessed glucose levels as a secondary outcome measurement have only measured random glucose levels and have not reported a significant change (Frazier et al. 2001; Cesena et al. 2002; Turgay et al. 2002; Ross et al. 2003; Sikich et al. 2004; Biederman et al. 2005a, 2005b; DelBello et al. 2007; McCracken et al. 2008). However, there are many case reports of SGA-induced diabetes. For example, between January 1993 and February 2002, 12 cases of newly diagnosed risperidone-associated diabetes were reported to the Food and Drug Administration's Medwatch Drug Surveillance System (Koller et al. 2004a). Between January 1997 and February 2002, 24 newly diagnosed quetiapine-induced hyperglycemias were reported to the same administration (Koller et al. 2004a). Most cases appeared within 6 months of treatment initiation, and severity of hyperglycemia ranged from mild glucose intolerance to diabetic ketoacidosis or hyperosmolar coma.
Despite the limited reports of lipid and glucose changes in the youth population when compared with adult studies, some studies suggest that children and adolescents might be at a higher risk than adults for developing SGA-related metabolic side effects (Hellings et al. 2001; Woods et al. 2002; Safer 2004; Fedorowicz and Fombonne 2005; Correll and Carlson 2006).
It is important to mention that comparison between adults and youths is based on different studies using different designs and populations. It is then possible that these differences are due to factors, other than treatment or age, which are different in the studies but not taken into account during the comparison (i.e., genetic background, population, and protocols).
To our knowledge, there is no previous study that has compared the effect of three SGAs on BMI, FBG, and lipids between youths and adults in the same population and with the same protocol for up to 24 months.
The purpose of this study was to explore the age-dependent metabolic effects of SGAs in a homogenous, SGA-naïve population, which includes both youths and adults, as well as the time-dependent nature of such effects by specifically investigating these effects after 3, 6, 12, and 24 months on an SGA.
Methods
This study retrospectively reviews the charts from patients treated with SGAs and participating in a program to monitor metabolic effects of SGAs at the Hôtel-Dieu de Lévis hospital, an affiliated university hospital center with adult psychiatric and child and adolescent psychiatric units near Quebec City, Canada. This clinical program called the “Second-Generation Antipsychotic Monitoring Program” was established to systematically and closely monitor the occurrence of metabolic effects in patients using SGA treatment for the first time. The four SGAs approved by Health Canada when the program started were olanzapine, risperidone, quetiapine, and clozapine. During the period from October 2003 to May 2007, when referred by their psychiatrist to the program before starting SGAs, patients were seen by a psychiatric nurse who measured baseline weight and height and took a 12-hour fasting blood sample to assess total cholesterol (TC), triglycerides (TG), low-density lipoprotein (LDL), high-density lipoprotein (HDL), and FBG. Patients were contacted systematically for follow-up assessment where the same measures were taken, with the exception of height in adults, at 3, 6, 12, and 24 months after treatment initiation.
All study procedures were reviewed and approved by the institution's ethics and research committee. Because this was a retrospective study using data contained in medical charts, patients were not required to give informed consent. All medical charts were reviewed by the principal investigator.
To be included in the study, patients had to be naïve to SGAs, that is, they had never taken antipsychotics before, and must have received treatment for at least 3 months. Only patients for whom laboratory values or parametric values (weight and height) were available before treatment initiation and at least 3 months later were included in the present study. We excluded patients who were diagnosed with diabetes or dyslipidemia before starting treatment.
The variables studied for metabolic effects were weight, BMI (calculated as weight in kilograms divided by height in square meters), glucose, TC, LDL, HDL, and TG. For the pediatric group, to take into account age-dependent variations in body composition, we obtained standardized BMI Z-scores using the children's BMI percentile-for-age calculator on the USDA/ARS Children's Nutrition Research Center at Baylor College of Medicine website (
For all patients, diagnoses were made by an experienced psychiatrist or child psychiatrist in accordance with the Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision (DSM-IV-TR) criteria (2000). Clinical data were obtained from chart notes before starting SGAs. We considered the main diagnosis as the diagnosis for which the patient received an SGA and all other diagnoses were considered as co-morbid disorders. In some cases, there was no clear diagnosis, but we obtained the diagnosis from the symptom list based on the DSM-IV criteria. For a clear presentation, we regrouped the main diagnoses into the following categories: Psychotic disorder, mood disorder, tic disorder, disruptive behavior disorder or impulsivity, and other disorders (includes pervasive developmental disorder, mental retardation, and obsessive-compulsive disorder).
Statistical analyses
For demographic and clinical characteristics of the study population, we provide percentages as descriptive statistics. Mean dosage of medication was calculated on a monthly basis. The outcome measures studied were changes at 3 and 6 months compared with baseline for weight, BMI, BMI Z-score, TC, HDL, LDL, TG, and FBG; Student's t-test was used for these analyses. Because these data were originally collected to clinically monitor metabolic effects, the time frame of the measures was not adhered to strictly. Therefore, we accepted data rounded off to 1 month for the 3 and 6 months intervals. Exploratory analyses were made with analysis of variance (ANOVA) to examine the effect of other variables (i.e., type of SGA, use of other treatment, and type of diagnosis on weight and BMI change). ANOVA with a Fisher test was used to examine if there was a difference between the three SGAs on their propensity to change weight and BMI. The statistical significance α-level (two-sided) was set at 0.05. All statistical analyses were performed using SAS 9.1.
Results
Demographic and clinical characteristics
A total of 232 charts of patients participating in a program to monitor the metabolic effects of SGAs was reviewed. They started SGA treatment between October 2003 and May 2007. Of these, 145 patients were excluded because of a previous trial with an SGA or an insufficient treatment duration or follow-up. Two patients were excluded because they were taking a hypolipidemic and an oral hypoglycemic at baseline. Thus, we selected 85 patients: 23 children (aged from 4 to 12 years), 35 adolescents (aged from 13 to 17 years), and 27 adults (aged from 18 to 62 years). We pooled the data of children and adolescents (referred to as youths, n = 58), as there was no difference in metabolic effects between these two groups. For many patients, data were missing at some time points during follow-up for either weight, lipids, or FBG measures, which is attributable to failure to show up for their appointment or having only either a measure of weight or a blood sample taken at some follow-up appointment. Therefore, weight was measured at baseline for 54 youths and 27 adults (total = 81), at 3 months for 38 youths and 17 adults (total = 55), and at 6 months for 37 youths and 17 adults (total = 54). Lipids were measured at baseline for 43 youths and 24 adults (total = 67), at 3 months for 29 youths and 18 adults (total = 47), and at 6 months for 27 youths and 16 adults (total = 43). FBG was measured at baseline for 42 youths and 25 adults (total = 67), at 3 months for 28 youths and 16 adults (total = 44), and at 6 months for 24 youths and 16 adults (total = 40).
Demographic and clinical characteristics of the study population are presented in Table 1. All of the patients were French Canadian Caucasians; 27 patients were adults and 58 patients were youths. In both groups, the majority of patients were male, 79% and 63% in the youth and adult groups, respectively. There was a notable difference in the proportions of main diagnoses for which patients were receiving SGAs between the two groups. The most frequent main diagnosis in the pediatric group was disruptive behavior disorder (34%), whereas it was psychosis (67%) in the adult group. Only 31% of the pediatric group was treated for psychosis. Attention-deficit/hyperactivity (ADHD) and disruptive behavior disorder other than ADHD were frequent co-morbidities for children and adolescents (55% and 26%), whereas only one adult (3%) had ADHD and none had disruptive behavior disorder. Personality traits or disorder and substance abuse or dependence were more frequent in adults (37% and 52%, respectively) than in youths (21% and 15%, respectively).
The assumption for chi-square has not been met: Expected counts are lower than 5 in a group.
Abbreviation: ADHD = attention-deficit/hyperactivity; PDD = pervasive developmental disorder.
In both groups, the majority of patients was treated with risperidone, 69% and 56% in the youth and adult groups, respectively. Only 4% of adults were treated with quetiapine compared with 21% of youths, whereas only 10% of youths were treated with olanzapine compared with 41% of adults. No patient was treated with clozapine, which was expected, because trials with other SGAs must be conducted before starting this second-line medication. Mean dosages were higher in the adult group than in the youth group for all three SGAs.
The following results summarize the principal findings from the data listed in Tables 2 and 3. To compare metabolic effects between adults and youths, we took only the first 6 months into account because only 6 (22%) and 1 (4%) of the adults were followed at 12 and 24 months, respectively, whereas monitoring was continued in 20 (34.5%) and 15 (25.9%) youths at these intervals. First, we compared adults' and youths' weight, BMI, lipid, and glucose changes from baseline to 3 and 6 months. We then did a second analysis in the youth group at 12 and 24 months for weight, BMI, and BMI Z-score changes.
Degrees of freedom = n − 1.
Abbreviation: BMI = body mass index; Δ = change (in).
Degrees of freedom = n − 1.
Statistically significant change, p < 0.05.
Abbreviations: HDL = high-density lipoprotein; LDL = low-density lipoprotein; TG = triglyceride; Δ = change (in).
Effect of SGA on weight, BMI, and BMI Z-score at 3 and 6 months
There were significant weight and BMI changes at 3 and 6 months in both groups (Table 2). To take into account morphologic differences between the youth and adult groups, changes relative to baseline (in percentage) appeared to be a more accurate way to compare these two populations than absolute weight change. Indeed, considering that youths have weight and BMI values that are clearly smaller than that of adults, absolute weight change can underestimate body composition change in youths compared with adults.
At 3 months, in the pediatric group, the mean weight change was 11.8% (t = 10.88, degrees of freedom [df] = 37, p < 0.0001) and the mean BMI change was 10.1% (t = 9.71, df = 37, p < 0.0001) compared with a mean weight change of 12.2% (t = 4.40, df = 16, p < 0.0001) in the adult group. For adults, the BMI change, which is weight in kilogram divided by the square of height, is always the same as the weight change because height is constant.
At 6 months, in the youth group, the mean weight change was 16.2% (t = 10.17, df = 36, p < 0.0001), and the mean BMI change was 11.8% (t = 8.58, df = 36, p < 0.0001), when compared with a mean weight—and BMI—change of 13.1% (t = 6.99, df = 15, p < 0.0001) in the adult group.
In youths, the mean BMI Z-scores were 0.02 at baseline, 0.63 at 3 months (change of 0.61, t = 9.03, df = 37, p < 0.0001), and 0.67 (change of 0.65, t = 7.59, df = 36, p < 0.0001) at 6 months. As mentioned above, BMI Z-scores were not used for adults.
Effect of SGA on weight, BMI, and BMI Z-score in youth group at 12 and 24 months
The first subgroup was followed for 12 months (n = 20), and the mean BMI Z-score change was 0.76 (t = 4.95, df = 19, p < 0.0001), increasing from −0.20 at baseline to 0.56 (Fig. 1). For the second subgroup, followed for 24 months (n = 15), the mean BMI Z-score change was 0.25 (t = 1.71, df = 14, p = 0.11), increasing from 0.29 at baseline to 0.54 (Fig. 2).
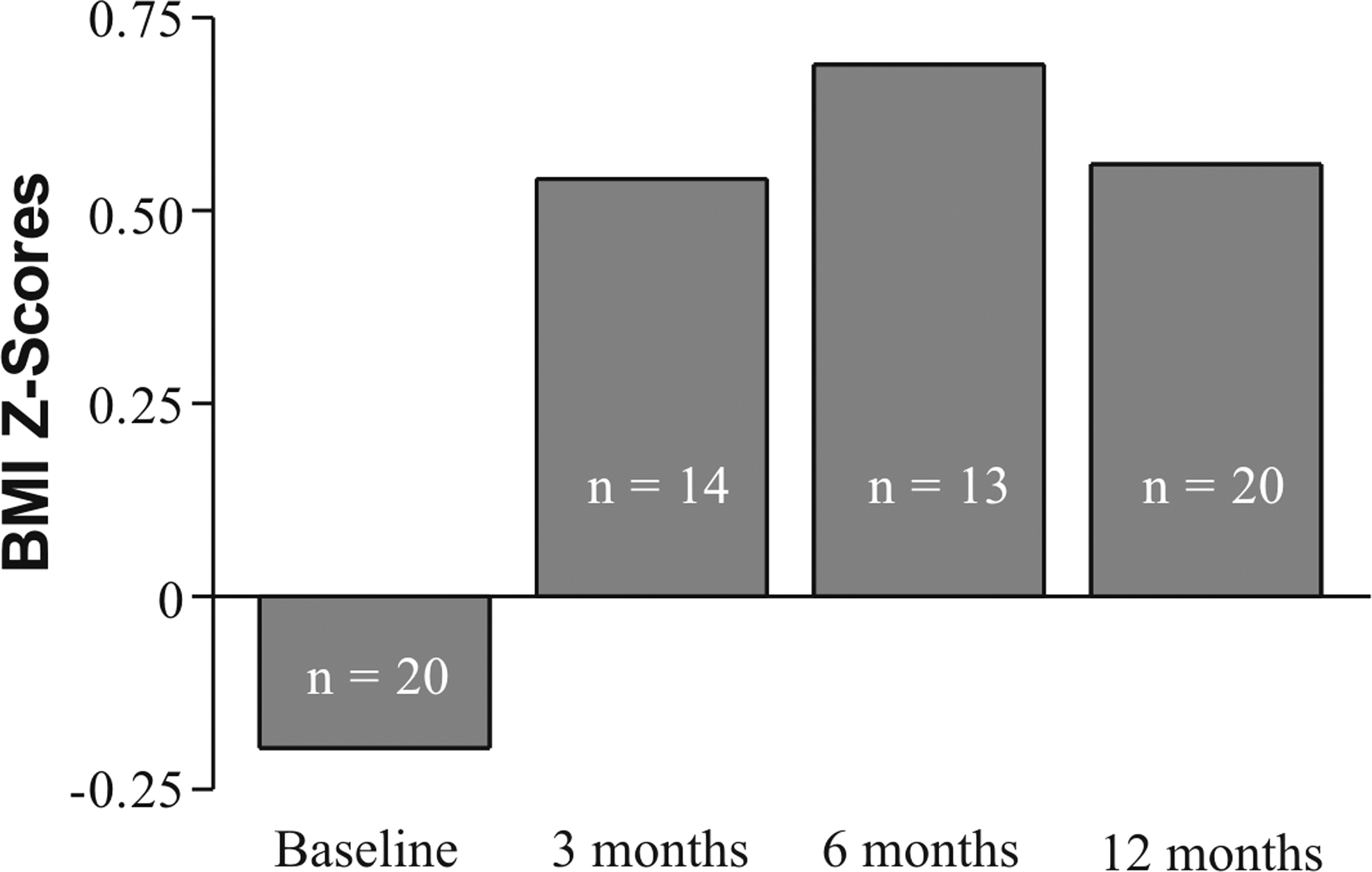
Body mass index (BMI) Z-score for patients followed at 12 months.
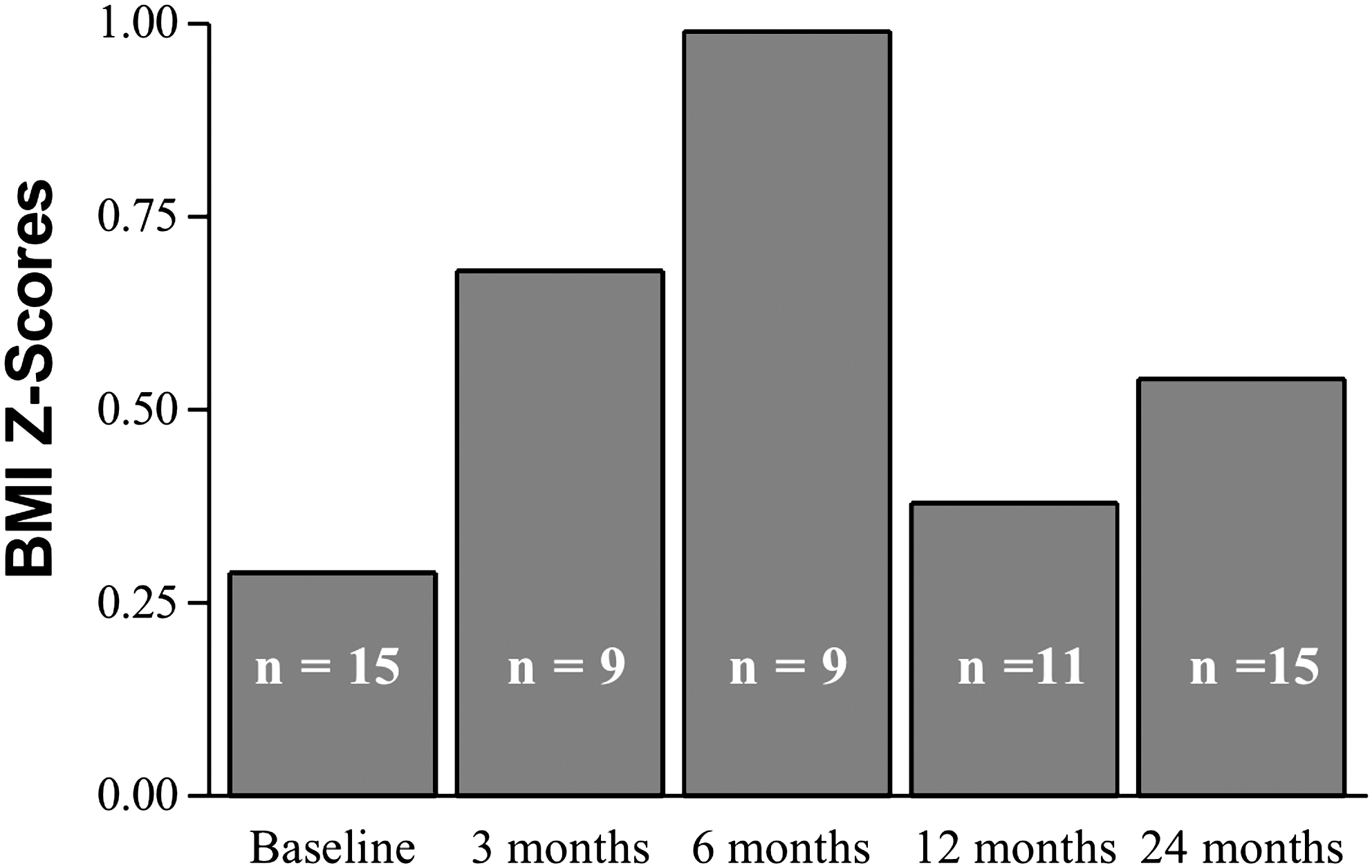
Body mass index (BMI) Z-Score for patients followed at 24 months.
For both groups that had follow-up, the highest level of BMI Z-score was at 6 months and the value decreased at time points after 6 months. However, at the endpoint, a difference persisted in BMI Z-scores compared with baseline.
Lipid metabolism
In the youth group, there was no significant change in levels of TC, HDL, and LDL, but there was a trend toward an increase in TG levels (18.2% [t = 1.94, df = 28, p = 0.06] and 38.1% [t = 1.67, df = 26, p = 0.11] at 3 and 6 months, respectively). In the adult group, there was a significant change in lipids: An increase in TC of 24.0% (t = 3.18, df = 17, p = 0.005) and 24.1% (t = 4.82, df = 14, p = 0.0003) at 3 and 6 months, an HDL increase of 10.2% (t = 2.28, df = 17, p = 0.04) and 17.1% (t = 3.22, df = 15, p = 0.006) at 3 and 6 months, and an increase of 26.8% (t = 2.98, df = 16, p = 0.009) and 30.1% (t = 2.94, df = 14, p = 0.01) in LDL at 3 and 6 months, respectively. Variation in TG remained nonsignificant (Table 3).
Glucose metabolism
In the youth group, there was no significant change in FBG at 3 and 6 months. In the adult group, there was a trend toward a significant increase of 4.8% (t = 1.94, df = 15, p = 0.07) in FBG at 3 months (Table 3).
Other analyses
For the youth group, ANOVA revealed a significant difference between the three antipsychotics in their propensity to change BMI Z-score at 3 months (F [1,2] = 4.67, p = 0.01) and 6 months (F [1,2] = 5.39, p = 0.009); at 3 months, the change from baseline in BMI Z-score was 1.11 for olanzapine, 0.65 for risperidone, and 0.38 for quetiapine; at 6 months, the change from baseline in BMI Z-score was 1.51 for olanzapine, 0.64 for risperidone, and 0.46 for quetiapine.
ADHD was a frequent co-morbidity in the youth group, and the frequent treatment for this condition was a psychostimulant. Because stimulants may reduce weight gain, we compared BMI changes between youths with and without stimulants. We found no difference in weight and BMI changes in patients treated with psychostimulants compared with those not treated with these medications (F = 1.15, p = 0.78).
There was also no difference in weight and BMI change between patients treated for psychotic disorders and those treated for other conditions.
Discussion
To our knowledge, this is the first study to evaluate metabolic effects in both SGA-naïve adults and youths from the same Caucasian homogenous population with the same standardized monitoring protocol and includes patients treated with three first-line SGAs with a follow-up to 24 months.
Weight gain
Our results showed that there is no age-dependent effect in weight changes among SGA-naïve patients. Youths experience a similar BMI change compared with adults after 3 and 6 months of treatment on SGA. The only other study that directly compares weight gain secondary to SGAs between youths and adults treated only by risperidone found a greater absolute weight gain in youths compared with adults after 1 year of treatment (Hellings et al. 2001). In contrast, we did find greater absolute weight gain in adults than in youths. However, in our study, when we consider BMI change and relative weight gain, which take into account morphologic changes in youths, we found no differences between youths and adults. Moreover, some studies including only patients naïve to antipsychotics have found greater weight gain than in studies including patients who have been previously exposed to antipsychotics (Perez-Iglesias et al. 2008; Correll et al. 2009). As suggested in a recent paper (Correll et al. 2009), greater weight gain reported in studies of youths treated with SGA compared with adult studies might be due to less previous exposure to antipsychotics in youths compared with adults. Our study confirms Correll's findings as our youth and adult groups, both naïves to SGAs, had similar body change composition. In opposition to what it was first thought (Ratzoni et al. 2002; Woods et al. 2002; Safer 2004; Sikich et al. 2004), it appears that youths treated with SGA are probably not more vulnerable than adults for weight gain.
In fact, other studies including pediatric patients, however, without an adult comparison, confirm our results of body changes by using BMI Z-score or BMI change (Reyes et al. 2006; Fraguas et al. 2008; Sikich et al. 2008; Kapetanovic et al. 2009). Sikich et al. (2008) found a BMI increase of 1.3 and 2.2 kg/m2, respectively, for risperidone and olanzapine, and a BMI Z-score increase of 0.23 and 0.39. These changes were found after an 8-week trial with risperidone and olanzapine. In our study, BMI Z-scores were not assessed at 2 months, but were higher at 3 months. Because we obtained the maximum increase of BMI at 6 months, it is possible to suggest that the BMI increases progressively from baseline each month until 6 months. This hypothesis needs to be confirmed by a closer monitoring of SGA weight changes. Another possible explanation would be the difference in patient clinical characteristics. Indeed, the Sikich study is limited to early onset schizophrenia disorder, whereas two-thirds of our youth population had a nonpsychosis diagnosis. It is possible that metabolic effects in youths could be different in nonpsychotic children and adolescents, but this also needs to be confirmed.
The relative weight gain of 11.8% and 16.2% and the BMI Z-score change of 0.61 and 0.65 at, respectively, 3 and 6 months, fulfills the set of criteria for a clinically significant weight gain, as described by Correll and Carlson (2006). However, in the longer-term follow-up at 12 and 24 months, we observed that body composition was only partially reversed and did not return to the baseline level. As described in other studies as a plateau effect of weight gain occurring around 6 months with SGAs (Jones et al. 2001; Kinon et al. 2001; Wetterling 2001), it also appears in our population that the peak change in body composition occurs at around the 6th month. This confirms a time-dependent SGA effect of weight gain in youths.
Of the four SGAs available in Canada in recent years (except ziprasidone), studies report that the highest weight gain is observed in youths treated with clozapine, followed by olanzapine and risperidone, whereas quetiapine causes the smallest weight gain (Fedorowicz and Fombonne 2005), which corresponds to observations in adults, except that risperidone ranks last in adults, just after quetiapine (Newcomer 2005). Our results confirm the greater tendency for olanzapine to increase weight when compared with both quetiapine and risperidone.
Our results confirm an age-independent effect of SGAs on weight gain. We also confirm in children and adolescents, a time-dependent effect of SGAs on weight gain, a finding which had already been reported in adults.
Lipid and glucose metabolism
For glucose and lipid levels in pediatric groups after 3 and 6 months of treatment on SGAs, our results are consistent with other studies (Shaw et al. 2001; Martin and L'Ecuyer 2002; Turgay et al. 2002; Sikich et al. 2004; Biederman et al. 2005a, 2005b), as we found no significant change for either of these variables as is the case in most studies on pediatric patients. Recently, Correll et al. (2009) reported significant lipid changes in drug-naïve children and adolescents after 8 weeks of SGA treatment. With olanzapine and quetiapine, significantly increased levels of TC and TG were reported; however, only TG increased significantly on risperidone. It is then possible that our varied results are due to the fact that the majority of our sample received risperidone. It is also possible to suggest a time-dependent effect on lipid metabolism with a peak at 8 weeks, followed by a rapid normalization, but this needs to be confirmed.
In contrast to the youth group, the adult group had significant lipid changes and a tendency toward glucose change even with a very small number of participants, as seen in many studies conducted with adult populations (Casey 2004; Newcomer 2005; Haddad and Sharma 2007).
The difference in the effect of SGAs on lipids and glucose between youths and adults might be due to a difference between the two groups studied in terms of diagnosis or treatment. Indeed, more adults were treated with SGAs because of a psychotic disorder than youths, and psychotic patients are more vulnerable to diabetes than the general population even when not treated with antipsychotics (Casey et al. 2004). However, in other reported studies (Sikich et al. 2004, 2008), pediatric patients were mainly but not exclusively psychotic, and the results, which are still similar to those of our study, indicate that the metabolic effects of SGAs may be independent of diagnosis. Also, the higher proportion of adults over youths treated with olanzapine, for which the literature reports more significant glucose and lipid changes than with risperidone and quetiapine (Newcomer 2005), may also have contributed to this difference. Lastly, because of the small size of our sample and some attrition during follow-up, we could not conclude that there was an age-dependant effect of SGAs on changes in glucose and lipid metabolism.
In summary, our original results confirm, in the same Caucasian homogenous population and with the same monitoring protocol, the age-independent effect of SGAs on weight gain, but we cannot conclude if there is an age effect for glucose and lipids changes. These results are difficult to interpret with respect to the controversy in the literature. In fact, it has been first hypothesized that the glucose and lipids effects of SGAs are the consequence of adiposity induced by weight gain, but this has been now brought into question as some reported cases of diabetic ketoacidosis associated with SGAs have occurred independently of weight gain (Koller et al. 2004b). Other published data have shown that these effects may be due to the receptor-binding affinity of the different antipsychotics (Simon et al. 2009).
Several limitations in this study deserve attention. Even if the data were collected prospectively by the clinical monitoring program, the retrospective design of the study contributed to the fact that data were missing at some time points. Owing to the small sample size, we pooled together patients taking three different SGAs to be able to detect the most important changes. However, the propensity to induce metabolic changes differs among these three SGAs and the proportion of patients taking each treatment varies between the adult and youth groups. Within the youth group, the small number of children and adolescents did not allow us to determine whether there was a difference between SGAs in causing metabolic effects. The lack of a control group taking different medication did not allow us to compare these metabolic effects in other psychiatric or therapeutic conditions. Also, the issues of the Z-scores for weight could have been somewhat addressed by having a comparison group of youth not taking medication as typical weight gain controls. Given that our Caucasian study population is in the lowest genetic risk group for metabolic dysregulation (Ananth et al. 2005), this might have contributed to fewer adverse metabolic effects by SGAs compared with studies with a genetically heterogeneous population.
Despite its limitations, this is the first study to directly assess the age-dependent metabolic effects of SGAs in SGA-naïve Caucasian homogenous population by evaluating youth and adult patients from a French Canadian population with the same clinical monitoring protocol. The use of relative BMI change and relative weight change, rather than reporting only absolute weight change to compare pediatric and adult populations, took into consideration the growth and morphologic differences between these groups. Reporting the BMI Z-score for youths also ensured that a true body composition change occurred, rather than only a change attributable to growth. This is also one of the rare studies to report long-term BMI Z-score data for patients treated with SGAs.
Conclusion
From the data presented in this study, it appears that there was likely no age-dependent effect on weight gain. Consequently, like adults, the weight of youths treated with SGAs should be monitored systematically. Even though we did not observe significant changes in FBG and lipids in youths compared to adults, given our small study population and the scarcity of published reports, more studies are needed to better understand SGA-related changes in FBG and lipids in youths.
Clinical monitoring programs should be adapted with respect to all of the variables influencing these metabolic effects, especially the age and time variables. In the lack of such protocols, these adverse effects might otherwise go unrecognized and remain unaddressed by the clinician. In addition, special health education programs (nutrition, fat consumption) will probably be helpful for individuals starting SGAs. Future research needs to focus on the effect of combination of education programs and pharmacotherapy.
Footnotes
Disclosures
Dr. Ben Amor serves on speaker's bureau for Eli-Lilly, Shire, Janssen-Ortho, and Purdue-Pharma. She has served as a consultant for Eli-Lilly, Shire, and Jansen-Ortho. She has received travel grants from Eli-Lilly, Shire, and Purdue. She has received research grant from the Canadian Institute for Health Research (CIHR).
Drs. Roy, Bedard, and Desmarais and Mrs. Jourdain, Allen, and Michaud have no conflicts of interest or financial ties to disclose.
Acknowledgments
This work was done at CHAU Hotel Dieu de Levis, Department of Psychiatry, Laval University, Levis, Quebec, Canada. Statistical assistance was provided by Mr. Paul-Marie Bernard, who is from the methodological support bureau at Laval University.