
Abstract
The study assessed competencies and practices of a large group of healthcare providers in childhood attention-deficit/hyperactivity disorder (ADHD), and identified barriers to improving care. Methods were self-assessment using an Internet questionnaire with a standardized patient case; analysis compared with professional association recommendations; and measurement of provider self-efficacy levels. Of 2,103 participants who completed the assessment, 44% were only “somewhat confident” and 20% “not at all confident” in being up-to-date in diagnosis and management of ADHD. Based on American Board of Psychiatry and Neurology's Child and Adolescent Core Competencies and American Academy of Child and Adolescent Psychiatry Practice Parameters, participants selected appropriate responses 60% of the time, 57% for items on diagnosis, and 62% for treatment. Providers under-used the family interview, and relied on ADHD rating scales for diagnosis. Lack of effective communication between provider, child, family, and teachers was the top barrier cited, yet participants rated involving the child and family as very important. In conclusion, education should include training on effective communication with the family to improve care for children with ADHD and dedication of further health education resources in the area of ADHD is needed.
Introduction
Assessment and treatment of symptoms that impair functioning are important because behavioral difficulties interfere with learning and friendships, and are associated with poorer health outcomes due to increased rates of nonfatal injuries, major injuries, hospitalizations, and emergency room (ER) visits as compared with peers (CDC 2007). Although effective treatments are available (Biederman et al. 1996), on average only 56% of the ∼4.4 million school-aged children who had ever had ADHD actually ever received treatment, according to a Centers for Disease Control survey of 100,000 families (CDC 2005). Analysis of the National Health and Nutrition Examination Survey spanning 2001 to 2004 shows that only half of those with ADHD who were 8 to 12 years of age sought treatment with a mental health professional (Merikangas et al. 2010). An important open question is, where are the current gaps in clinical practices that fail to meet healthcare needs of these children?
The standards for clinical practices are defined by professional associations, including the American Academy of Pediatrics (AAP) and the American Academy of Child and Adolescent Psychiatry (AACAP), as evidence-based guidelines on patient care, medical knowledge, and communication skills for ADHD assessment and treatment (AAP 2001; Pliszka et al. 2007). Clinical abilities are also defined in The American Board of Psychiatry and Neurology (ABPN) Child and Adolescent Core Competencies in the area of Patient Care (Board Core Competencies) (The ABPN 2005). Involving the child's family is central to both professional association recommendations and the Board Competencies—for example, interviewing children and their families, recognition of how family impacts consent and compliance, and education of patients and families on evidence-based medication use for ADHD. Effective communication, creating a therapeutic alliance, partnering to develop the management plan, and education are all recommended practices that specifically involve both patients and their families.
Competencies that could be assessed for future improvement include communication, diagnosis, treatment, and continuously monitoring the child's progress to update the differential diagnosis and treatment plan. The Board Core Competencies in practice-based learning and improvement further address the importance of recognizing limitations in the provider's own knowledge and skills, the need for life-long learning and active participation in educational activities.
The goal of this study was to assess competencies in ADHD assessment and treatment of children in a large group of healthcare providers, using an Internet educational activity designed as a case-based, self-assessment questionnaire. The objective was to uncover any gaps in current practices that could be addressed in the future with continuing educational resources and training to improve care, and ultimately child health outcomes.
Methods
Design and measures
We developed an Internet clinical practice self-assessment questionnaire to assess core competencies relevant to ADHD found in the Board Core Competencies (The ABPN 2005). The complete assessment is shown in Table 1 (Findling 2008). The assessment included a standardized child patient case vignette of a hyperactive, inattentive boy accompanied by his parents at a provider visit. Patient case vignettes are valid, noninvasive assessments that accurately reflect provider practices (Peabody et al. 2004; DeSanto-Madeya 2007). The 15 questions were in a multiple-choice, single-best-answer format on knowledge, diagnosis, communication skills, treatment, and follow-up care. The most appropriate answers designated correspond to Board Core Competencies and AACAP Practice Parameters for Assessment and Treatment of ADHD (The ABPN 2005; Pliszka et al. 2007) reviewed by the continuing medical education (CME) reviewer at Medscape, and the CME faculty coauthors. The AACAP guidelines were selected for comparisons, as representative of professional recommendations and as similar to those of the AAP. Polling questions assessed perceptions of self-efficacy as levels of confidence in practice and also respondent-based barriers to optimal management of ADHD.
The Internet Assessment patient case-based questions and appropriate answers used to score the assessment are shown. The questions correspond to ABPN core competencies.
Abbreviations: ABPN = American Board of Psychiatry and Neurology; ADHD = attention-deficit/hyperactivity disorder; CME = continuing medical education.
Medscape, LLC, is accredited by the Accreditation Council for Continuing Medical Education to provide CME for physicians, and certified this assessment for 0.25 hours of CME credit. The activity was available to all providers with free, online access beginning December 9, 2008, and continued to be available online through December 2009 for credit, at MedscapeCME:
Polling results displayed after questions showed immediate feedback to each participant, using averages of aggregate data from all participants. A postactivity, online evaluation survey assessed whether the activity supported the learning objectives, was clearly organized, presented objectively and free of commercial bias, would impact clinical practice, and would be recommended to others. Multiple-choice answer options were five responses from “strongly agree” to “strongly disagree.”
Participants
Inclusion criteria for a participant in this study were registration at MedscapeCME as a U.S. healthcare provider and completion of the CME activity for credit, which is free of charge. No clinical specialties or professions were excluded. Participant subgroups defined based on the highest numbers of providers' responses were 1st, psychiatry/mental health; 2nd, primary care providers (PCPs), including family medicine, general practice, and internal medicine; and 3rd, pediatrics. Exclusion criteria were nonclinical registration information or noncompletion of the CME activity.
Statistical approach
To collect participant data, we tracked completion of the assessment for CME credit (Findling 2008). We de-identified data and analyzed it in aggregate to maintain confidentiality of participants' information. Data included responses from December 9, 2008, to January 15, 2009, from all participants who completed the CME activity. We scored responses according to concordance with evidence-based recommendations and citations, and calculated overall mean scores. We compared the percent correct responses to assessment questions to identify areas of competence and to identify practice gaps.
Results
Participation
Overall, 2,103 participants completed the Internet assessment for CME credit during the first 5 weeks. Participation was highest in the first 15 days, an average of 106 participants per day. The majority identified their profession as physician (71%), with the next largest group psychologist (7%), and nursing (7%) (shown in Table 2). Clinical specialties of the participants were relevant to care of children with ADHD, 57% in the specialty of psychiatry (including mental health and psychology), 12% in pediatrics, and 10% PCPs. “Child and adolescent psychiatry” and “child psychology” were not specified as categories. Pediatrics included subspecialties of general pediatric, allergy, and cardiology pediatrics. We chose psychiatry, PCPs, and pediatrics as the three participant specialty subgroups for further analysis and likely to reflect the population of providers who manage pediatric patients with ADHD.
Participants who completed the Internet assessment by profession, occupation, and specialty are shown.
Other “professions and occupations” identified by participants included <1% each of Chiropractor, Clinical Case Manager, Clinical Nurse Specialist, Clinical Researcher, Health-Business, Health IT, Lab Technician, Medical Educator, Nutritionist, Optometrist, Paramedic, Pharmacist, Physical Therapist, Podiatrist, Rehabilitation Specialist, Senior Executive, and Senior Manager.
Other specialties identified by participants included <15 each of Administration, Anesthesiology, Cardiology, Critical Care, Dermatology, Diabetes, Emergency Medicine, Endocrinology, Education/Teaching, Gastroenterology, Geriatrics, Hematology, HIV/AIDS, Infectious Diseases, Neonatal, Neurosurgery, Nutrition, Obstetrics/Gynecology, Occupational Health, Oncology, Ophthalmology, Orthopedic Surgery, Otolaryngology, Pain Management, Pathology, Patient Education, Pharmacotherapy, Physical Medicine, Preventative Medicine, Public Health, Pulmonary Medicine, Radiology, Research, Rheumatology, School Health, Sports Medicine, Surgery, Urology, and Wound/Ostomy.
Evaluation
Responses to the CME evaluations indicate high participant satisfaction. These questions were not required for awarding CME credit; however, each of the evaluation questions was answered by from 1,197 to 1,236 of the total 2,103 participants. On a 5-point scale of agreement, 93% “strongly agreed” or agreed that the activity supported the learning objectives, and 91% that it was organized clearly. In addition, 86% “strongly agreed” or agreed that the activity content will impact their clinical practice, and 89% that they would recommend the activity to others. Further, 92% of respondents “strongly agreed” or agreed that the activity was presented objectively and free of commercial bias. Participants provided open text comments about the educational format in the activity evaluation including that comparison with colleagues was a good learning experience, and that immediate feedback showing online polling results of peers was helpful.
Competence and gaps in ADHD assessment and treatment
The majority (64%) of participants were only “somewhat confident” or “not at all confident” (44% and 20%, respectively) in being up-to-date in diagnosis and management of ADHD (assessment question 16), a measure of self-efficacy. Only 26% of participants identified themselves as “confident” and even fewer, 10% as “very confident.” This shows recognition of limitations and underscores a need for lifelong learning, as recommended in the ABPN Core Competencies (competency IVA) (The ABPN 2005).
Surprisingly, low percentages of appropriate responses were seen for some of the assessment questions, based on the corresponding Board Core Competencies. Participants (N = 2,103) selected appropriate responses 60% of the time on average, 57% for items on diagnosis and 62% for treatment. The results varied widely from a low of 14% to a high of 93% (shown in Table 3). Analysis of provider specialties shows similar percentages of appropriate responses on average for competence and practices, psychiatry at 66% (n = 1,197) and pediatrics at 61% (n = 252), with PCPs lower at 54% (n = 203), summarized in Figure 1: Provider Responses on Case-Based, ADHD Clinical Practice Self-Assessment (% appropriate response).
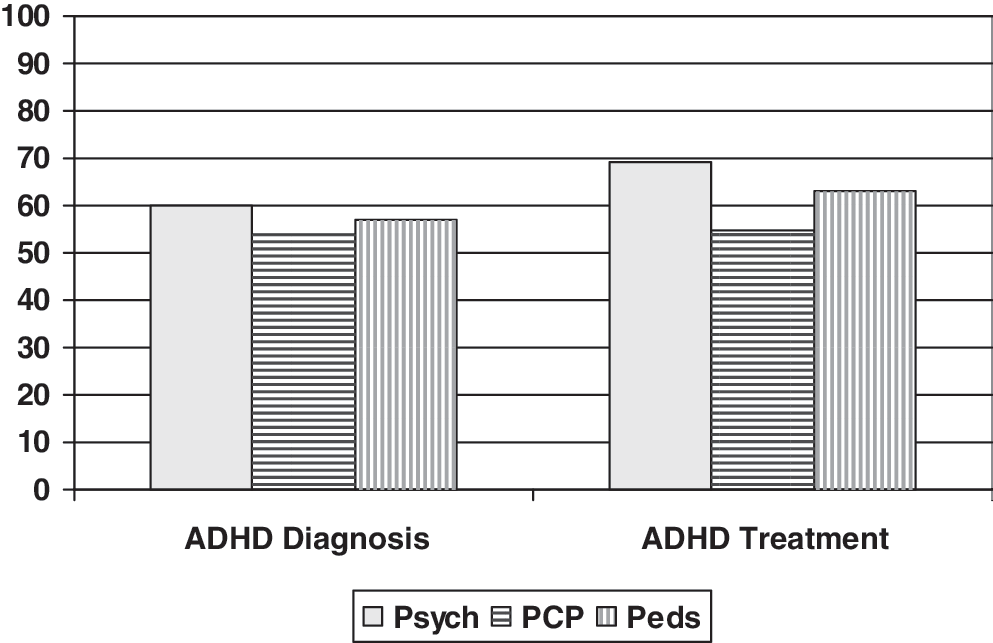
Provider responses on case-based, ADHD clinical practice self-assessment (% appropriate response). Average appropriate responses percentages for the assessment questions in areas of ADHD diagnosis and ADHD treatment are shown by specialty. Appropriate response is based on the corresponding Board Core Competencies for ADHD (ABPN 2005). Psychiatry, n = 1,197; PCP, n = 203; Pediatrics, n = 252. ADHD = attention-deficit/hyperactivity disorder; Psych = psychiatry; PCP = primary care provider; Peds = pediatrics.
Average appropriate responses of participants in the Internet ADHD assessment are shown by specialty. Psychiatry n = 1197; PCP n = 203; Pediatrics n = 252; All N = 2,103.
Not averaged due to overlap of answer values, that is, validity issue.
Abbreviations: FDA = Food and Drug Administration; PCP, primary care provider; Peds = pediatrics; Psych = psychiatry; Q = question.
ADHD assessment
For competence related to diagnostic skills and knowledge of ADHD epidemiology in children, overall participants selected appropriate responses 57% of the time on average, and the psychiatry subgroup 60% (Table 3A). On average, 90% chose to conduct a mental health assessment including screening the child with hyperactivity for ADHD and for impairment (assessment question 1; based on ABPN Core Competency IB1a, the Diagnostic and Statistical Manual of Mental Disorders, 4th edition [American Psychiatric Association 1994] multi-axial differential diagnosis). Fewer participants understood that ADHD rating scales cannot be used as a sole basis for diagnosis, at 68% correct overall, 72% correct for psychiatry (question 12; competency IIB3f, knowledge of clinical rating scales). Only 34% recognized impairment in two settings is required for ADHD diagnosis, but severe impairment of the child in any one setting warrants treatment (question 10, competency IB1a). These data may reflect difference of opinion within the provider community rather than a gap in best practices.
For diagnosis, only 59% overall chose the important next step of performing a detailed interview with the parent to define the child's symptoms, duration, severity, and frequency (assessment question 2). The interview relates to competency IB4: Enhance the ability to collect and use clinically relevant material. This result shows a gap in communication with the family, vital to diagnosis of disorders in children.
Knowledge of ADHD epidemiology and comorbid conditions was unexpectedly low, at 35% appropriate response overall, 37% for psychiatry (question 9; ABPN competency IIB2g, knowledge of epidemiology). Most participants overestimated the numbers of patients with ADHD who meet diagnostic criteria for bipolar disorder. Further, only 19% overall correctly identified high incidence of ADHD in the teenage years (question 8; competency IIB2g). The majority of participants in all specialties underestimated continuation of ADHD symptoms into adolescence. However, due to overlapping answer ranges, this question may have limited accuracy and was not factored into the overall results analysis.
ADHD treatment
For competence related to ADHD treatment and knowledge of neuroscience, 62% of participants overall selected appropriate responses, 69% in psychiatry, 55% in PCP, and 63% in pediatrics. Following diagnosis of ADHD, 67% of participants chose discussing a comprehensive pharmacologic and nonpharmacologic plan with the child and family, an important communication-related competency (question 3, ABPN competency IIIA4). Fewer chose to consider a range of therapies for children with ADHD and comorbidities (38% overall and 44% of psychiatry), including combining behavioral and pharmacology treatment (question 13, competency IB5). On the best initial approach to therapy, only 35% of participants chose the response “any medication approved by FDA” for ADHD, which is recommendation 7 of the AACAP (Pliszka et al. 2007), in favor of other choices of particular medications. This may reflect provider preferences rather than a difference in competence.
Overall, 85% of participants chose stimulants as the treatment choice for children found to have ADHD to decrease overall aggressive acts and antisocial behavior. In addition, 81% identified the side effect profile of stimulant use in children as insomnia, headache, irritability, and emotional lability. Fewer PCP and pediatric participants chose nonstimulant therapy options in cases when the child with ADHD also has substance abuse, comorbid anxiety, or tics (55% and 70% vs. 89% of psychiatrists). Similarly, when selecting a nonstimulant, 52% of PCP and 66% of pediatrics groups chose appropriate Food and Drug Administration–approved nonstimulant atomoxetine, approved for children with ADHD versus 75% of psychiatry participants (question 6, competency IB7).
We tested the competency of monitoring progress of the child to integrate new information and changes in clinical presentation into an update differential diagnosis and treatment plan (question 5 and ABPN competency IB8). The patient case we presented was a child who failed to respond to several trials of Food and Drug Administration–approved therapies for ADHD over time. Only 45% overall chose the appropriate response, to review the diagnosis of ADHD (52% of psychiatry, 46% of PCPs, and 50% of pediatrics subgroups). Most choices were in favor of further medication, without a review of the diagnosis.
Medical knowledge of ADHD-related abnormalities of neurotransmitters dopamine and norepinephrine associated with the disorder was high, at 81% among psychiatry but lower at 50% in PCP, and 62% in pediatrics participant groups (question 14 and competency IID16), which may be expected based on the training for each specialty.
Clinical barriers to care
To assess barriers to providers' experience in their own practices, we provided 5 common barrier choices, and an open category (question 17, competencies IVA and IVE2). While this question was not required, response was high (n = 2,089 of N = 2,103). Lack of effective communication between provider, child, family, and teachers was by far the top barrier at 54% overall, psychiatry 55%, PCP 53%, and pediatric groups 53% (Table 4). Other barriers cited included side effects of therapies (12%–18%) and for PCP's, staying up-to-date with new treatment data (17%). However, ∼10% indicated efficacy of therapy as a barrier, and 3% treatment disparities based on race and ethnicity. Barriers of effective communication and concern about side effects are likely to represent the most significant barriers experienced, as <10% of participants selected the open category “other barrier.”
Barriers to optimal management of ADHD that healthcare providers report experiencing in their practices are shown by specialty.
We included a polling question on perceptions of the importance of involving the child and family in the decision-making process for the ADHD treatment plan. The overwhelming majority, ∼90% of participants, rated involving the child and family as “very important.” The perceived importance of involving the family is particularly striking as communication is also a top barrier identified in the assessment results.
Discussion
Evidence for competency and gaps in clinical practice skills related to ADHD are provided in this Internet assessment of over 2,000 providers: Psychiatrists and psychologists, pediatricians, and primary care healthcare providers. Reducing the burden of childhood ADHD on the child, family, healthcare system, and society is a challenge. Clinical practices can improve with continued training of healthcare professionals; however, recognition of particular areas of ongoing educational need is required.
Surprisingly, the majority of providers in the study reported low levels of confidence in being up-to-date in the therapeutic area of ADHD. Core competencies address the importance of recognizing limitations in a provider's own knowledge and skills, and the need for life-long learning. The results of the Internet assessment uncover areas where practices are not yet in accord with the Board Core Competencies and professional society recommendations for patient care.
Strengths and limitations of the study
One limitation of the study design is that for self-efficacy measures and barriers to improving practice, we used providers' self-reported information, which might be biased toward the socially desirable choice. In addition, providers who chose to complete the assessment may have felt a particular need to update their practice, introducing a potential for selection bias. Clarity of the questions and response choices may have been limiting in one question (question number 8), where an overlapping ranges of answer choices reduced response validity for that item.
Strengths of the study include linking test items to specific core board clinical competencies. Use of a standardized child patient case vignette as the basis for questions eliminated inter-patient variability as found in chart reviews (Peabody et al. 2004; DeSanto-Madeya 2007). The large study group and participation by psychiatry and mental health providers are central strengths of the study. In addition, the participation by primary care and pediatrics who may first encounter children with ADHD symptoms adds to the strength of the study.
The effectiveness of CME in improving knowledge and practices has been demonstrated in numerous trials (Casebeer et al. 2008; Cook et al. 2008; Lam-Antoniades et al. 2009; Mazmanian et al. 2009); however, questions of objectivity sometimes arise. For this CME activity, over half of the participants completed the optional section evaluating the activity for potential bias. The data show that these participants found the activity objective and free from commercial bias, and believed that the assessment would impact their clinical practices.
Competence and performance gaps
Overall measures of provider competence and performance gave similar average results for ADHD diagnosis as for treatment, 57% and 62% appropriate responses, respectively. Medical knowledge assessed was highest in pharmacologic therapy, including effects of stimulants on behavior, and side effect profiles, 85% and 81%. Participants demonstrated knowledge of the biochemical basis of disease, abnormalities in dopamine, and norepinephrine neurotransmitters associated with ADHD, at 70% appropriate responses. Knowledge of appropriate uses of nonstimulant medications was slightly lower. The largest practice gaps identified by appropriate response percentages related to effective communication with the family (59%), knowledge of ADHD epidemiology, comorbidities and diagnostic criteria in childhood and adolescence (35%), and, importantly, the review of diagnosis when approved treatments fail (45%).
Screening of the child for ADHD symptoms of hyperactivity was well understood and implemented, based on the assessment. However, providers demonstrated under-use of the family interview, and over-reliance on ADHD rating scales for diagnosis. In contrast, the AACAP recommendations and Board Core Competencies emphasize importance of interviewing both children and their families. In this assessment, lack of effective communication between provider, child, family, and teachers was also the barrier to improving care most frequently reported by providers. In addition, nearly all participants rated involving the child and family as very important to them. This indicates a need for education on when and how to use the family interview and to improve family communication during assessment and follow-up care. Due to reimbursement patterns in ambulatory care, constraints on PCP and pediatrician time may influence the ability to engage in effective communication with the family.
A second important competency is discussion of a comprehensive ADHD treatment plan with the child and family. Up to 33% of providers did not opt to discuss treatment options with the family before prescription of therapy. Including family discussion in the treatment decision impacts consent and compliance, and creates a therapeutic alliance. AAP Guidelines direct inclusion of the parents, child, and teacher in the identification of target outcomes, development of treatment plans, and assessment of response to treatment (AAP 2001).
The majority of providers completing the assessment failed to revisit the diagnosis of ADHD and reassess the child, when treatment failed. Providers were more likely to modify medication than to update the differential diagnosis. This may indicate a construct bias toward ADHD over other potential disorders in the differential diagnosis when symptoms of hyperactivity are seen.
In the assessment reported here, the majority of providers underestimated the proportion of children with ADHD who will continue to meet criteria for ADHD in their teenage years. Long-term, 8-year, follow-up studies of children with ADHD in the Multimodal Treatment of Children with ADHO (MTA) study show that functional impairment continues relative to local normative comparison group, in 19 of 21 variables tested (Molina et al. 2009). These include important areas of antisocial behavior, academic achievement, and social functioning, underscoring the need for comprehensive treatment of ADHD. Yet, only 32% of the children in the study were medicated over 50% of days in the past year. This is consistent with the Centers for Disease Control survey of families, and National Health and Nutrition Examination Survey data analysis showing that only approximately half of those children with ADHD actually receive treatment (CDC 2005; Merikangas et al. 2010).
Barriers to pharmacologic treatment of ADHD may include perceptions of potential cardiovascular risk associated with stimulant use for children and adolescents with or without prior heart problems (Kuehn 2009). Labeling of methylphenidate and amphetamine agents advise against use in patients with serious structural abnormalities, cardiomyopathy, or seriously abnormal heart rhythm. Careful screening for cardiovascular disease during the patient and family history is an important aspect of evaluation before treatment. However, reports of serious cardiovascular events and sudden death, and recent associations between sudden unexplained death in those without cardiovascular disease show adverse events are rare (Gould et al. 2009). From a 10-year observational study, 1.8% of sudden unexplained deaths, youths were taking stimulants, whereas in a comparison group of accidental deaths, 0.4% were taking stimulants (Gould et al. 2009). The benefit–risk ratio remains positive, considering the effects of treatment on functioning, and the low rate of adverse events.
In the clinical practice assessment reported here, providers cite side effects of therapies as a barrier to improving clinical care at only 12% to 18%. This indicates that cardiovascular safety concerns are unlikely to be the sole cause of childhood ADHD undertreatment. In comparison, the majority of psychiatrists, pediatricians, and PCP participants noted ineffective communication with the child, family, and teachers as a top barrier to care.
In conclusion, the assessment results show that improving practices of providers who care for children with ADHD should be a priority. Effective remedies are needed to bridge the gap between the number of children with ADHD and the number of these children who actually receive evidence-based interventions. Further education is important, considering the competence and practice gaps identified and the disruptive effects of the disorder on children's functioning, along with the tremendous associated societal costs, estimated at over $42 billion per year (Pelham et al. 2007). Education should include training on effective communication with the family to improve care for children with ADHD. The study results advocate for dedication of further health education resources in the area of ADHD.
Footnotes
Disclosures
Dr. Brown is an employee of Medscape LLC and has no financial relationship with any pharmaceutical company. Dr. Hertzer has no financial relationship with any pharmaceutical company. Dr. Findling has received research grants from Abbott, Addrenex, AstraZeneca, Bristol-Myers Squibb, Forest, GlaxoSmithKline, Johnson & Johnson, Lilly, Neuropharm, Otsuka, Pfizer, Shire, Supernus Pharmaceuticals, and Wyeth and served as a consultant for Abbott, AstraZeneca, Biovail, Bristol-Myers Squibb, Forest, GlaxoSmithKline, Johnson & Johnson, KemPharm, Lilly, Lundbeck, Novartis, Organon, Otsuka, Pfizer, Sanofi-Aventis, Sepracor, Shire, Solvay, Supernus Pharmaceuticals, Validus, and Wyeth and speakers' bureau for Bristol-Myers Squibb, Johnson & Johnson, and Shire.