
Abstract
Background:
Methylphenidate (MPH) is an efficient treatment to reduce behavioral symptoms of attention-deficit/hyperactivity disorder (ADHD); however, its impact on cognitive functioning has not been sufficiently demonstrated so far. This study investigates the hypothesis that MPH improves attention-related cognitive functions.
Methods:
Sixty-seven medication-naive boys aged 6–13, with newly diagnosed ADHD, were tested before treatment with a neuropsychological assessment battery, including the Wechsler Intelligence Scales for Children (WISC-IV) and the Test of Attentional Performance for Children (KITAP). A follow-up assessment was performed after 8–12 weeks, with 37 participants receiving MPH treatment and 30 controls without medication. The effect of MPH on test performance was analyzed by repeated measures analyses of variance.
Results:
Both groups improved significantly across a broad range of psychometric measures of cognitive performance. There were no significant interaction effects of group and time on attention-related cognitive functions. Exploratory analyses revealed an effect of MPH on verbal comprehension in the WISC-IV.
Conclusion:
The study results do not support that MPH improves attention-related cognitive functions of boys with ADHD. The potential effect of MPH on verbal abilities deserves further research.
Introduction
Methylphenidate (MPH) is known as an effective treatment (Biederman 2005); it reduces especially symptoms of hyperactivity and impulsivity in children (Santosh and Taylor 2000). The stimulant drug acts on the dopamine and norepinephrine systems (Pliszka et al. 2006) and increases frontal and striatal activation in children with ADHD (Vaidya et al. 1998). Since the frontal-striatal circuit is relevant for various attention functions (Eslinger and Grattan 1993; Sturm et al. 1999; Chamberlain and Sahakian 2007), it can be suggested that MPH improves corresponding cognitive abilities.
Regarding direct evidence for the influence of MPH on cognitive abilities and attention, many previous studies found no effect, among them the most rigorous studies. Taking a possible publication bias toward positive findings, the current literature provides no consistent information of the benefit of MPH regarding cognitive abilities of children with ADHD. In a review of about 40 placebo-controlled studies measuring various neuropsychological parameters, Pietrzak et al. (2006) conclude that MPH improves task performance in 63.5% of studies, whereas the remaining studies found no change or a even a decline of performance. If positive effects are reported, they tend to be specific rather than generalized. Positive effects have been found for sustained attention/vigilance (Zeiner 1999; Riccio et al. 2001; Konrad et al. 2004, 2005; Epstein et al. 2006; Tucha et al. 2006) and inhibition (Vaidya et al. 1998; Konrad et al. 2004, 2005). There are also studies describing a positive effect of MPH in working memory (Zeiner 1999), processing speed (Bedard et al. 2002, Epstein et al. 2006), variability of reaction time (Epstein et al. 2006), and set shifting (Konrad et al. 2004, 2005; Pietrzak et al. 2006).
However, positive findings are rarely replicated. For example, Kempton and her colleagues describe an improvement of cognitive abilities in nearly all investigated parameters, whereas Rhodes et al., using the same tasks, describe only very specific effects (Kempton et al. 1999; Rhodes et al. 2006). Further, some other authors describe a missing effect of MPH at least on specific abilities (Van der Meere et al. 1999; Tucha et al. 2006; McInnes et al. 2007). Even negative effects of MPH are reported (Sprague and Sleator 1977).
The neuropsychological outcomes included in previous studies are often very specific, which might be responsible for the inconsistent findings and further limits external validity. Most of the studies addressing cognitive functions in children with ADHD analyzed only executive functions, and for some specific skills (e.g., set shifting) there are fewer studies available. To gain more insight into the influence of MPH on cognitive functions of patients with ADHD, it is essential to investigate the influence of MPH on a broad range of cognitive abilities in one and the same sample and to include analyses of effect size estimates. To this aim, we investigated the effects of MPH in individually tailored and clinically appropriate doses. Given that the deficits of children with ADHD described above encompass attention as well as intelligence components, we concentrated on both domains, the more so as they are highly interacting (Fry and Hale 2000; Schweizer et al. 2005).
As MPH influences networks associated with attention (Vaidya et al. 1998; Pliszka 2005), we expected an improvement in the MPH group compared with the control group in multiple cognitive abilities, despite some contradictory results affecting specific neuropsychological measures. Specifically, we expected an improvement in 1. intelligence components: Working memory and processing speed, as well as 2. attention skills: Stability of attention (variability of attention), inhibition, attentional set-shifting (cognitive flexibility), and sustained attention.
Additionally, we measured other components of intelligence (verbal abilities and fluid intelligence) for exploratory analyses. Since some authors describe reaction time as a critical factor assessing attention skills, we explored reaction times in attention tasks in order to reveal a possible speed-accuracy trade-off (Koschack et al. 2003; Lajoie et al. 2005). Finally, because very few studies investigated the relationship between behavioral symptoms and cognitive aspects, we decided to address this question.
Materials and Methods
Recruitment and procedure
Subjects were recruited from the Outpatient Clinic for Child and Adolescent Psychiatry/Psychotherapy at the University of Ulm and from a cooperating office-based child and adolescent psychiatrist. The study protocol was approved by the local ethics committee. Inclusion criteria were (1) meeting Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association 1994) criteria for ADHD based on a parent report and/or teacher report, (2) a clinical diagnosis of ADHD based on questionnaires and unstructured clinical interview by the treating therapist, who was not involved in the study, (3) being medication-naive, (4) an IQ of 80 minimum, (5) sufficient command of the German language, and (6) no other predominant diseases. Between February 2007 and December 2009, all male patients aged 6–13 who met the eligibility criteria were informed about the study and included by given written consent. We did not include girls because of sex differences in respect to prevalence (Faraone et al. 2003; Polanczyk et al. 2007), ADHD symptoms (Gershon 2002), and performance in neuropsychological assessment (Goldbeck et al. 2010). We compared two groups, in terms of the change of cognitive performance between two assessment times with an interval of 3–4 months. Both groups were medication-naive at the first assessment. At the second measurement, one of the groups had been treated with MPH and the other had received no medical treatment. For those who consented to participate, the baseline assessment was conducted in the context of standard diagnostic procedures.
After confirmation of the diagnosis, parents and children were educated about treatment options for ADHD, based on current guidelines (Taylor et al. 2004), and a joint decision was made regarding pharmacological treatment. Depending on this decision, children were allocated either to the MPH group or to the control group. A randomized allocation was declined because of ethical concerns about withholding an effective treatment from a group of children. Both groups were compared in terms of sociodemographic parameters, baseline cognitive abilities, ADHD symptoms, and co-morbid symptoms.
Neuropsychological assessment was usually spread across two morning sessions within each time-window of assessment. Parents of children in the MPH group were instructed to give medication one hour before testing to guarantee an optimal release of the drug during the course of the session (Banaschewski et al. 2008). MPH dosage and medication time were noted. The minimum time between baseline and follow-up measurements was 8 weeks, with the condition of a parent-reported symptom-reduction for the MPH group. The number of weeks was 11.5 (for intelligence) and 10.6 (for attention) in the control group, and 16 (for intelligence) and 14.5 (for attention) in the MPH group.
Instruments
DISYPS
German questionnaires evaluating DSM-IV and ICD-10-criteria of specific mental disorders were used (DISYPS) (Döpfner and Lehmkuhl 2000; Döpfner et al. 2008). Parents and teachers were asked to rate the behavior of participants with respect to ADHD symptoms at both assessment times. Further, parents rated level of symptoms of common co-morbid disorders, that is, conduct disorder/oppositional defiant disorder, depression, and anxiety. The rating scale for each symptom ranges from 0 to 3. All questionnaires have high internal consistency, with Cronbach's α ranging from 0.89 to 0.94 for the mean score (Döpfner et al. 2008).
Wechsler Intelligence Scales for Children-IV
The German version of the Wechsler Intelligence Scales for Children (WISC) in its recently revised version (HAWIK-IV) (Petermann and Petermann 2007, 2008) was used. The WISC-IV (Wechsler 2003) measures the Full-Scale (FS) IQ, which is calculated from four composite scores each comprehending two or three core subtests: “Verbal Comprehension Index” (VCI; subtests “Similarities,” “Vocabulary,” “Comprehension”), “Perceptual Reasoning Index” (PRI; subtests “Block Design,” “Picture Concepts,” “Matrix Reasoning”), “Working Memory Index” (WMI; subtests “Digit Span,” “Letter-Number-Sequencing”) and “Processing Speed Index” (PSI; subtests “Coding,” Symbol Search”). The reliability coefficients are high, with 0.97 for the FS IQ and values ranging from 0.87 to 0.94 for the composite scores (Petermann and Petermann 2007). In the context of the present study, retest analyses conducted with 20 healthy children (age: M = 9.88 years, SD = 0.56; IQ: M = 19.75, SD = 10.38) and a time interval of approximately 6 weeks between measurements showed high reliability for the four indices VCI (0.97), PRI (0.88), WMI (0.89), PSI (0.84), and the FS IQ (0.94).
Test of Attentional Performance for Children
The Test of Attentional Performance for Children (KITAP) (Zimmermann et al. 2002) is a standardized computer-based test battery that measures various attention skills based on the model by Van Zomeren and Brouwer (1994). All KITAP tasks are embedded in a virtual environment of an enchanted castle to ensure the motivation of the children. We selected four tasks: 1. Flexibility: Set-shifting task, requiring redirecting attention to the current tasks demands 2. Go/Nogo: Participants have to react to one sort of stimulus but ignore another sort of stimulus 3. Distractibility: Task based on the Go/Nogo-paradigm, supplemented with distracting conditions 4. Sustained Attention: Task requiring effortful maintenance of selective attention over 10 minutes.
Standardization of the KITAP was achieved with healthy children aged 6–10, who were separated into a younger (6–7) and older (8–10) group. Depending on test and age group, the standardization sample comprised 130–340 children. The selection of parameters for the present study (a list can be seen in Table 3 in the result section) was based on the a priori hypotheses, given the precondition that the parameter shows satisfying reliability according to the test authors. The split-half reliability for variability of reaction time lies between 0.64 and 0.85, for the errors (including omission and commission errors) between 0.65 and 0.97, with the exception of errors in the flexibility task in the age group 8–10, for which it is 0.55 (Zimmermann et al. 2002).
Retest analyses (6 weeks interval) with 20 healthy children showed medium to strong correlations in the used parameters standard deviation Flexibility (0.93), errors Flexibility (0.87), commission errors Distractibility (0.63), commission errors Go/Nogo (0.60), commission errors Sustained Attention (55), and omission errors Sustained Attention (0.60).
Data analyses
Statistical analyses were carried out with PASW (SPSS 18®) for Windows. To compare sociodemographic variables and frequency/intensity of symptoms between the MPH group and control group, χ 2-tests or t-tests for independent samples (Welch tests) were conducted. For the WISC-IV-analyses, standardized scores were used. Since KITAP standardization data are only available for children aged 6–10, KITAP raw data were used after controlling for plausibility and exclusion of extreme outliers. Repeated measures analyses of variance with time (baseline, follow-up) and group (MPH, control group) as independent variables were conducted for each dependent variable as proposed in the hypotheses. Because of multiple comparisons, the Bonferroni-Holm procedure for multiple tests was applied (Holm 1979). Further, as a measure of effect size, Cohen's d was computed (Cohen 1988), based on the F-values of the group × time interaction effects. Additional exploratory analyses of variance were performed with the WISC-IV VCI and PRI as dependent variables. A multivariate repeated measures analysis of variance was conducted including reaction times of all investigated KITAP tasks. Finally, differences of the scores of both measurements for parent ratings and cognitive parameters and Pearson correlation coefficients for them were calculated to investigate relationships between behavioral and cognitive changes.
Since the control group was nonrandomized and there may exist differences on observed covariates between the two groups, these differences could lead to biased estimates of treatment effects. Although the univariate comparisons of means for the variables in Table 1 give no strong hints on that, these comparisons are not sufficient, because these differences do not account for correlations among the covariates (Schafer and Kang 2008). Rosenbaum and Rubin (1983) suggested the use of propensity score techniques to aid in the evaluation of cause–effect hypotheses in nonrandomized (observational) studies. The propensity score for an individual, defined as the conditional probability of being treated given the individual's covariates, can be used to balance the covariates in the two groups, and thus reduce this bias (D'Agostino 19981). Several strategies are available to estimate causal effects (Schafer and Kang 2008) and to combine propensity score estimation and application methods (Harder et al. 2010).
Patients receiving MPH after baseline assessment.
Control group: patients without medication.
ADHD = attention-deficit/hyperactivity disorder; ODD/CD = oppositional defiant disorder/conduct disorder; MPH = methylphenidate.
In our study, propensity scores were calculated by using a logistic regression analysis with the covariates listed in Table 1. Missing data in the covariates have been estimated by multiple imputation with five replications. The mean propensity score of the MPH group was 0.40 (SD = 0.14), and the mean score of the control group was 0.51 (SD = 0.17). The distributions showed a sufficient overlap (Fig. 1) and group differences in all of the variables in Table 1 increased to p > 0.75. Thus, the propensity score seems to balance the covariates in the two groups well, and was included as a covariate in the analyses of variance in Tables 2 and 3.

Box plots representing the distribution of propensity scores in the group with MPH and in the control group without MPH (CG). CG = control group; MPH = methylphenidate group.
p < 0.05, adjusted p (Bonferroni-Holm).
t = assessment time; t1 = baseline; t2 = follow-up; MPH = methylphenidate group, CG = control group.
t = assessment time; t1 = baseline; t2 = follow-up.
p < 0.05, alpha level adjusted for multiple tests (Bonferroni-Holm).
Results
Sample description
Sixty-seven boys completed the study, comprising 37 boys assigned to the MPH group and 30 boys assigned to the control group. A detailed overview of recruited patients and drop-outs can be seen in the diagram based on the CONSORT statement (Schulz et al. 2010) in Figure 2. Sociodemographic characteristics and severity of ADHD symptoms rated by parents and teachers are presented in Table 1.
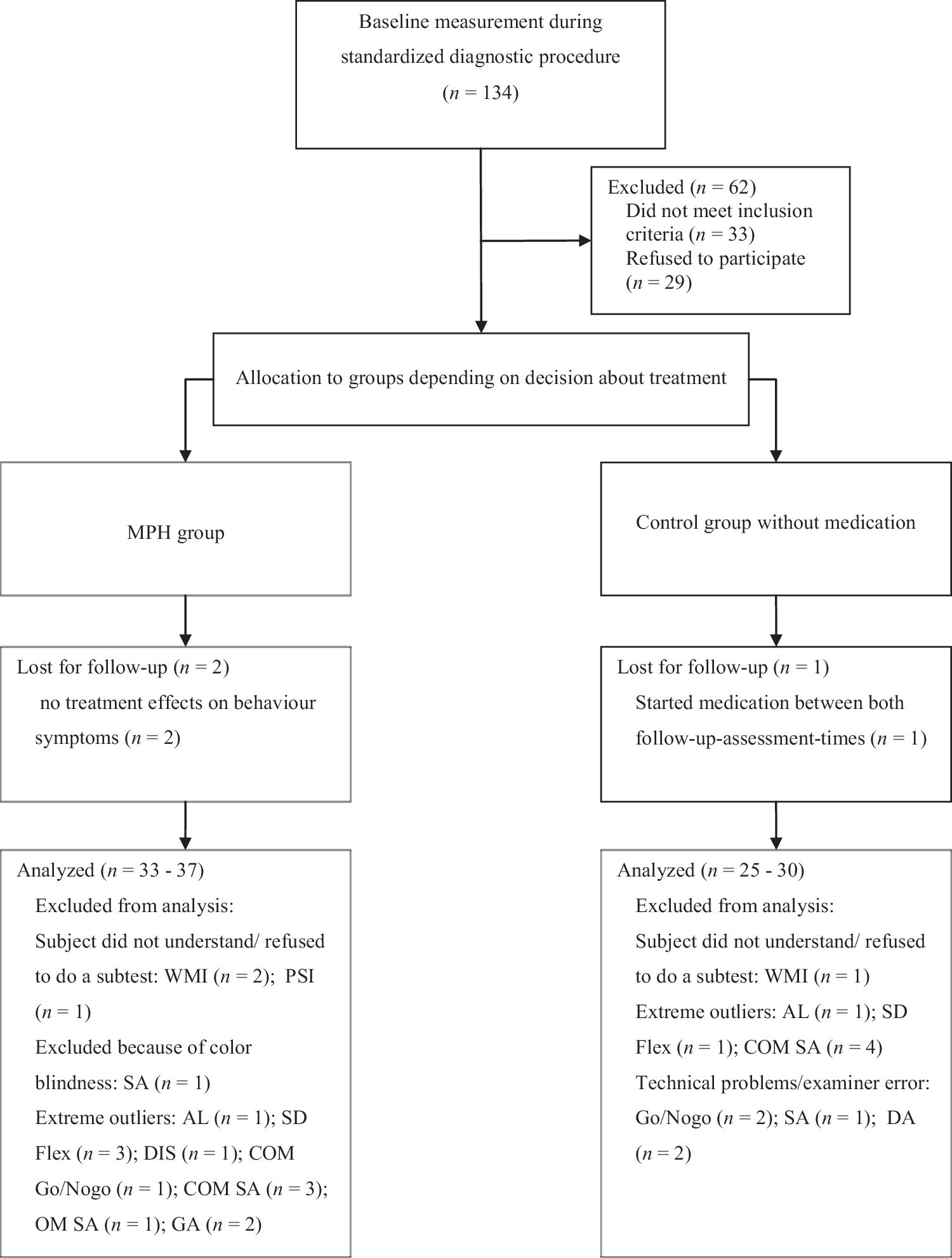
CONSORT diagram showing flow of participants
Neither age nor IQ was significantly different between the MPH and control groups. Further, there were no group differences in severity of ADHD symptoms as rated by parents and teachers (see Table 1). Regarding the complete sample and according to parent ratings, 28 (41.8%) of children were allocated to the primarily inattentive subtype, 10 (14.9%) to the hyperactive subtype, and 21 (31.3%) to the combined subtype. According to teachers, 30 (44.4%) of the participants belonged to the primarily inattentive subtype, 5 (7.5%) to the hyperactive subtype, and 16 (23.9%) to the combined subtype. Groups did not differ regarding ADHD subtype as rated by parents [χ 2 (4, 67) = 2.278, p = 0.60] or teachers [χ 2 (4, 67) = 0.79, p = 0.94]. As can be seen in Table 1, there were also no group differences in co-morbid symptoms of oppositional defiant disorder/conduct disorder, depression, or anxiety.
Behavioral treatment response was validated by parent and teacher ratings. These ratings showed, as expected, a more remarkable remission of ADHD symptoms in the MPH group compared with the control group. Parent questionnaires of both measurement times were available for 32 participants in the MPH group (t1: M = 1.8, SD = 0.5; t2: M = 0.9, SD = 0.5) and 25 in the control group (t1: M = 1.7, SD = 0.4; t2: M = 1.4, SD = 0.7), teacher questionnaires for 28 participants in the MPH group (t1: M = 1.8, SD = 0.4; t2: M = 0.7, SD = 0.5), and 21 in the control group (t1: M = 1.8, SD = 0.6; t2: M = 1.6, SD = 0.7). Repeated measures analysis of variance for these parent ratings revealed a main effect of time [F(1, 55) = 62.12, p < 0.001] and a significant interaction group × time interaction effect [F(1, 55) = 18.93, p < 0.001]. Teacher ratings showed significant main effects of group [F(1, 47) = 9.26, p = 0.004] and time [F(1, 47) = 66.46, p < 0.001] as well as a significant group × time interaction effect [F(1, 47) = 37.47, p < 0.001]. Effect sizes were large, according to parent (d = 1.20) as well as teacher ratings (d = 1.20).
Ceiling effects in cognitive outcomes occurred in less than 5% of the study participants at pretest except the errors in the Go/Nogo test with a 7.6% ceiling effect. At the second assessment, ceiling effects varied between 0 (SD Flexibility) and 19% (Errors Flexibility).
Changes of performance in working memory and processing speed
The results of the repeated measures analyses of variance including covariate analyses adjusting for possible baseline differences are shown in Table 2. None of the analyses showed a main effect of group, but both parameters showed significant main effects of time indicating an improvement with time. There were no significant interaction effects of group and time.
Since the subtests of the WMI differ in complexity, additional analyses were carried out for both subtests. The subtest Digit Span showed neither significant main effects of group or time nor a significant interaction effect of group and time. The analyses of the subtest Letter-Number-Sequencing revealed a significant main effect of time in the direction of improvement and a significant main effect of group, with better performance of the MPH group, and again no interaction effect of time and group.
Changes of performance in attention parameters
To examine our hypotheses concerning attention parameters, six parameters of the KITAP were analyzed. An overview of the results including covariate analysis to adjust for possible baseline differences can be seen in Table 3.
Again, they showed no main effects of group, but significant main effects of time in all investigated attention parameters, with better performance by the participants at the second compared with the first measurement. Time effects stayed significant after Bonferroni-Holm correction. Further, there remained no significant interaction effect of group and time after correction of alpha level for multiple tests.
Additional exploratory analyses
Exploratory repeated measure analyses of variance were conducted with the VCI and the PRI of the WISC-IV. The only significant interaction effect of group and time, with more prominent improvement in the MPH group, occurred in the VCI. Detailed results and effect sizes are shown in Table 2. Subtests of the VCI were analyzed separately. Significant interaction effects with more prominent improvement in the MPH group were found in the subtests Vocabulary and Comprehension.
A multivariate repeated measure analysis of variance including reaction times of the four KITAP tasks was conducted for those participants with complete data (32 participants in the MPH group and 27 in the control group). The results showed no significant main effects of time or group or an interaction effect of time and group.
Pearson correlation coefficients between changes in behavioral and cognitive outcomes were not significant.
Discussion
The aim of the present study was to investigate the effects of MPH on intelligence components and attention skills, measured with well-established psychometric tests. We compared the performance of boys with ADHD treated with MPH to that of boys with ADHD without pharmacological treatment.
As expected, the treatment with MPH showed a significant reduction of behavioral symptoms according to parents' and teachers' ratings. Summarizing the results of cognitive outcomes, all parameters showed main effects for time, mostly highly significant, indicating a remarkable improvement with time across all participants of the study regardless of treatment with MPH. These effects can be interpreted as due to training with repeated assessments, which is known to be relevant, especially in processing speed (Lipsius and Petermann 2009). After correcting the significance level for multiple tests, there were no significant interaction effects of time and treatment group in the primary outcome variables based on our hypotheses. Thus, our results indicate that individually tailored doses of MPH do not improve these cognitive deficits typically associated with ADHD. Nevertheless, exploratory analyses gave first clues on enhancement of verbal abilities by treatment with MPH. In the following section our results concerning intelligence and attention are discussed more extensively.
Effect of MPH on working memory and processing speed
We proposed that treatment with MPH would improve working memory and processing speed. However, children with or without MPH treatment did not differ in enhancement of these abilities between baseline and follow-up assessment. Thus, some previous findings of positive effects on working memory at least in subgroups of patients (Tannock et al. 1995; Zeiner 1999) are not supported by our results. Bedard et al. (2007) found the influence of MPH limited to more effortful verbal working memory tasks. Similar to Bedard et al. (2007), we used two different verbal working memory tasks varying in complexity; nevertheless, none of our tasks showed an influence of MPH. Regarding processing speed, the partially positive findings of previous studies (Reid and Borkowski 1984; Riccio et al. 2001; Bedard et al. 2002; Whyte et al. 2004; Epstein et al. 2006) are not supported by our results. However, since our sample did not show baseline deficits in processing speed, we cannot exclude that children with clinically relevant deficits could benefit from medical treatment.
Effect of MPH on attention
We expected an MPH-induced improvement in attention skills measured by six parameters concerning the stability of attention as well as accuracy of task performance. Contradicting our hypotheses, no interaction effects of time and group emerged. Before correcting the significance level for multiple tests, there was an interaction effect of group and time in omission errors in the Sustained Attention task, indicating superiority of the MPH group; however, this effect did not survive adjustment of the alpha level.
Our results are consistent with those previous studies showing absent or very limited and specific effects of MPH on performance in attention tests (Scheres et al. 2003; Boonstra et al. 2005; Rhodes et al. 2006; Coghill et al. 2007). In contrast to some previous studies (Konrad et al. 2004, 2005; Tucha et al. 2006), we found similar improvement of attentional performance in the MPH group and in the control group without medication. Methodological differences make comparisons between studies difficult. For example, Tucha et al. (2006) used the Test of Attentional Performance (TAP) (Zimmermann and Fimm 1992), which was originally designed for adults and is therefore much less motivating for children than the instrument we used, which was derived from TAP, but especially developed for children. Further, it has to be noted that the authors of the cited study did not adapt the significance level of their analyses in spite of analyzing multiple parameters, and most of their effect sizes ranged from small to medium. Konrad et al. (2004) suggested differential dose-response correlations, which might further explain inconsistent findings.
Effect of MPH on other intelligence components
Exploratory analyses showed no impact of MPH on the perceptional reasoning index, measuring fluid intelligence. However, our results revealed a significantly greater improvement of verbal abilities in the MPH group compared with the control group. This effect was especially apparent in the areas of vocabulary and perception of social life and is worth further investigation. In the literature there are emerging signs of a positive influence of MPH on higher verbal processes. Francis et al. (2001) found an enhancement in story retelling, specifically in the recognition and/or expression of internal responses and attempts of characters in story narratives under MPH. Also, McInnes et al. (2007) reported a positive influence of MPH on the ability to make inferences from complex explanations, which is an important skill needed to comprehend language successfully. In line with these findings, it could be suggested that MPH improves the ability to understand language—that is, to clearly comprehend the actual meaning of a question—as well as the organization and recall of verbally coded information.
Interaction of the effect of MPH on behavioral symptoms with cognitive changes
There were no correlations between the improvements in behavioral symptoms and changes in cognitive parameters, indicating distinct mechanisms of the influence of MPH on behavior and cognition. This finding is consistent with other studies that found nearly no relationships between these areas (Aman et al. 1991; Konrad et al. 2005; Coghill et al. 2007) and with the results of Konrad and coauthors (2005), who found that the behavior ratings of inattentive symptoms are more strongly related to objective measures of motor activity than with objective measures of attention.
In this study, we evaluated a broad range of cognitive outcomes, whereas many other studies targeted only very narrow outcomes. Accounting for possible baseline differences between the MPH and the control group concerning sociodemographic variables, intensity/severity and type of ADHD, co-morbid symptoms, and general cognitive abilities, the analyses were adjusted using propensity scores as covariate. Another strength is the naturalistic design of our study with the inclusion of real-world patients treated according to current clinical guidelines. However, some methodical limitations of our study have to be considered. First of all, due to ethical reasons we were not able to randomize the study subjects to either condition. However, calculation of propensity scores and inclusion of propensity scores in a covariate adjustment did not significantly change the results. Therefore, it is unlikely that baseline differences between groups might have impacted upon our findings. Definitely, our results should be interpreted with caution, until the findings are replicated in a randomized controlled study. Second, our sample size was quite small, limiting the statistical power of the analyses. Thus, some small to moderate effects as indicated by out effect size estimates may have been undetected by the statistical tests, especially after the necessary adjustment of the alpha level due to multiple tests. Moreover, the mean retest interval in the control group was about 4 weeks shorter compared to the MPH group. Because the duration of the interval between measurements is a critical factor for practice effects in cognitive tasks (Hausknecht et al. 2007), it cannot be excluded that this difference possibly led to an advantage for the control group. Finally, concerning the tasks used, current theories of ADHD including motivation as important component (Sergeant 2005) have to be considered. Although in general a motivating design of performance tasks as in the KITAP is helpful to engage children in psychological tests, it might be that it masks specific deficits particularly of children with ADHD that would occur rather in more boring tasks (Drechsler et al. 2009).
In conclusion, our results suggest no substantial specific effect of MPH concerning the performance of boys with ADHD in standardized psychometric measures of working memory, processing speed, and in multiple attentional functions. Findings of previous studies that reported the efficacy of MPH to improve very specific cognitive functions should not be over-generalized. The potential of MPH to induce an improvement of verbal abilities should be analyzed in future studies with larger samples and with longer follow-up intervals.
In absence of significant effects of MPH on the neuropsychological outcomes in this study we can also conclude that our findings do not provide any evidence for clinically relevant improvement of cognitive functioning of boys with ADHD by individually tailored pharmacological treatment with MPH. The potential of MPH to enhance cognitive performance in this population within a follow-up interval of 8–12 weeks appears limited. Thus, clinical decisions on treatment and evaluation of treatment effects have to be based on the core behavioral symptoms of ADHD and not on cognitive performance.
Footnotes
Disclosures
Dr. Hellwig-Brida, Dr. Daseking, Prof. Keller, Prof. Petermann, and Prof. Goldbeck declare that they have no financial interests and no other potential conflicts of interest.