
Abstract
Objective:
To examine the pharmacokinetics (PKs) and pharmacodynamics (PDs) of OROS® methylphenidate (OROS MPH) dosed once daily (QD) versus an early standard regimen (immediate-release [IR] MPH dosed three times daily [TID]) under various breakfast conditions.
Methods:
This single-center, double-blind, double-dummy, randomized, crossover study of OROS MPH (NCT00269815) in children aged 6 to 12 years with attention-deficit/hyperactivity disorder evaluated the PKs and PDs of MPH given with different breakfast conditions: OROS MPH administered after a high-fat breakfast, after a normal breakfast, or after fasting and IR MPH administered after a normal breakfast or after fasting in the morning and at two subsequent time points during the day. To maximize information, patients were divided into two groups, each receiving three of the five treatments for 1 day in a three-period, randomized, crossover design. Patients were assigned to 1 of 3 dosage levels (OROS MPH 18, 36, and 54 mg QD, and an assumed equivalent regimen of IR MPH 5, 10, and 15 mg given TID) based on their prestudy established clinical dose of IR MPH. PD measurements included Combined-Attention and Deportment scores on a rating scale of school behavior (the Swanson, Kotkin, Agler, M-Flynn, and Pelham), global assessments of efficacy, and activity monitor levels during academic seatwork. Serial blood samples for PK analysis were taken predose, and then every 60 to 90 minutes until 11.5 hours postdose. Vital signs were assessed predose, and then every 1.5 to 2.5 hours until 11.5 hours postdose.
Results:
Of the 32 patients enrolled, 31 completed the study. The PK profiles for MPH after OROS MPH administration were similar under all conditions (with normal, high-fat breakfast, or fasting). No bioequivalence tests of OROS MPH and IR MPH under various breakfast conditions were done because there were so few patients in each dose level of treatment. The two IR MPH conditions (after normal breakfast and fasting) were not compared. The drug-to-metabolite ratios (area under the curve) for all OROS MPH and IR MPH treatments were similar. OROS MPH and IR MPH provided a similar therapeutic effect, irrespective of breakfast conditions, as demonstrated by the Swanson, Kotkin, Agler, M-Flynn, and Pelham Attention and Deportment measures and global assessments. No serious adverse events, no deaths, and no clinically significant changes in vital signs were reported, except for one patient who was discontinued early because of repeated systolic blood pressure elevations on study day 1.
Conclusions:
The results of this study demonstrate that in children with attention-deficit/hyperactivity disorder, administering OROS MPH with or without food produces similar PK and PD profiles.
Introduction
The development of long-acting formulations has led to reduced need for multiple daily dosing, greater convenience and adherence, and enhanced confidentiality for school-aged children during the school day (AACAP 2007). OROS MPH (Concerta®, Raritan, NJ) is an osmotic controlled-release formulation of MPH with a 12-hour duration of effect in children with ADHD (Pelham et al. 2001; Swanson et al. 2003; Coghill and Seth 2006; Wigal et al. 2006). The OROS MPH formulation has been demonstrated to provide efficacy over a 12-hour period with minimal fluctuation, attributed to its unique ascending profile, which delivers escalating but controlled amounts of MPH to overcome the tachyphylaxis (Pelham et al. 2001; Swanson et al. 2003). After oral administration of OROS MPH, plasma MPH concentrations reach an initial peak at ∼1 hour, followed by a gradually ascending profile with peak concentrations occurring ∼6 to 10 hours after administration (Concerta [package insert] 2010). Clinical studies have established the safety and efficacy of once-daily (QD) dosing of OROS MPH in the treatment of ADHD in children, adolescents, and adults (Pelham et al. 2001; Wolraich et al. 2001; Swanson et al. 2003; Wilens et al. 2005, 2006; Medori et al. 2008; Adler et al. 2009). However, this is the first report of the pharmacokinetic (PK) profile of this medication in relation to diet and pharmacodynamics (PD) in children with ADHD. To minimize unnecessary procedures in the special population of pediatrics, and because the primary comparison of interest was the evaluation of food on the PK and PD of MPH, inclusion of a placebo arm was not considered essential.
Previous literature has demonstrated that food did not alter the PK or PD properties of an acute dose of IR MPH (Chan et al. 1983), but the effect of food on the OROS delivery technology had not been evaluated. Because OROS MPH is administered in the morning, the impact on therapeutic effect of administering the drug concurrently with breakfast may be important. The objective of this study, therefore, was to evaluate the effects of various breakfast conditions on the PK and PD of OROS MPH administered QD. IR MPH was used as the standard. This study also introduced an evaluation of the potential effect of the fat content of breakfast on PK and PD properties of the OROS MPH formulation. The design of this study allowed for the evaluation of the PK and PD of OROS MPH taken either fasting or after a normal breakfast and administered after a high-fat breakfast. Because this study was designed to evaluate the drug delivery technology (i.e., OROS formulation), the impact of other meals provided during the day was not considered to have as important an effect.
Methods
The protocol and consent/assent forms were reviewed and approved by the University of California, Irvine (UC Irvine), institutional review board. Each study participant and his or her parent(s) or guardian(s) were required to be informed of the nature, purpose, risks, and duration of the study; sign a written assent form; and freely agree to participation in the study. No study procedures were performed until consent was obtained.
Patients
Otherwise healthy boys and girls aged 6 to 12 years at the time of consent with a diagnosis of one of the three subtypes of ADHD verified by a parent interview and a teacher assessment were eligible for enrollment in the study. Patients were required to have received MPH for ≥3 months at some time in the past at a dose of IR MPH 5 to 20 mg at least twice daily or SR MPH 20 to 60 mg/day (alone or in combination with IR MPH). Patients were required to have been on a stable dose of MPH within these dose specifications for at least 4 weeks before enrollment and considered to be positive responders to MPH therapy.
Patients with any clinical condition that would interfere with the conduct of the study, those with known clinically significant gastrointestinal conditions (including narrowing of the gastrointestinal tract), marked anxiety, tension, agitation, depression, or a psychotic disorder, and patients with a history of seizures or Tourette's syndrome were excluded from the study. Patients with hypertension, defined as a mean of two blood pressure measurements (systolic or diastolic) greater than the 95th percentile for age, sex, and height at screening, were excluded as well. Further, patients whose primary focus of treatment was oppositional defiant disorder, conduct disorder, tics, or mood disorders also were excluded.
Within the 4 weeks before study enrollment, patients were not allowed to have received medication for MPH-related insomnia, anticonvulsants, or any investigational medication. Within 7 days before study enrollment, patients were not allowed to have received other medications that affect central nervous system performance (e.g., sedating antihistamines) or blood pressure, and they were not permitted to have changes in prescribed therapy.
Study design
This was a single-center, double-blind, double-dummy, randomized, crossover study. Patients were assigned to receive 1 of 3 dosages of OROS MPH based on their prestudy, clinically established IR MPH dose (both the morning dose and the total daily dose), with an emphasis on the morning dose. Patients previously receiving IR MPH were converted to an OROS MPH total daily dose approximately three times their morning IR MPH dose (e.g., a patient who received 5 or 10 mg three times daily [TID] of IR MPH would be converted to a dose of 18 or 36 mg of OROS MPH, respectively). For patients previously receiving SR MPH, it was assumed that a morning dose of 20-mg SR MPH would be equivalent to 5-mg IR MPH administered TID (thus, a morning dose of 40-mg SR MPH would be converted to a morning dose of ≥5-mg IR MPH and a total daily dose of 36 or 54 mg of OROS MPH per day). Dose conversions are given in Table 1.
IR = immediate-release; SR = sustained-release; QD = once daily.
Study medications were administered in a blinded fashion using a double-dummy technique: Active and placebo medications were identical in appearance for OROS MPH and IR MPH. To establish the double-dummy, double-blind conditions, placebo controls of the alternate treatment were administered simultaneously with active treatment. For example, a subject receiving 36-mg OROS MPH would receive two active OROS MPH tablets, one placebo OROS MPH tablet, and three placebo IR MPH tablets in the morning; three placebo OROS MPH and three placebo IR MPH tablets 4 hours later; and three placebo OROS MPH and three placebo IR MPH tablets 4 hours after that. Each treatment began on day 1, and the laboratory school evaluations (reported here) were obtained 7 days later.
Patients were divided into two groups and then randomized into one of three treatment regimens in a crossover design, with at least 5 days between treatments, during which patients received their prestudy medication dose and regimen. Study treatment regimens were as follows:
Group 1
OROS MPH QD after a high-fat breakfast
OROS MPH QD administered in a fasted state
IR MPH TID administered in a fasted state
Group 2
OROS MPH QD after a high-fat breakfast
OROS MPH QD after a normal breakfast
IR MPH TID with the first dose given after a normal breakfast
The normal breakfast consisted of 1 cup of cereal with a 4-oz cup of 2% milk with an estimated 4 g of fat; the high-fat breakfast consisted of 1.5 to 2 doughnuts (∼26 g of total fat) plus 8 oz of whole milk (8 g of fat) for an estimated total of 34 g of fat. The fasted condition consisted of no food intake overnight or in the morning before dosing; however, ½ cup of water was provided to swallow medication and ½ cup of orange juice was allowed before catheterization. The patients in the fasted condition also received a normal breakfast ∼1.5 hours after the first dose.
Lunch and dinner were provided in the laboratory school setting. Each treatment lasted 1 day and took place in a laboratory school setting at a single site under the supervision of experienced medical staff, psychologists, counselors, and laboratory classroom teachers. Children were assigned to 1 of 2 classrooms based on age (6–9 years and 10–12 years).
Assessments
Pharmacokinetics
Serial blood samples were collected via a catheter placed in the antecubital vein in each subject's forearm to measure the plasma MPH and major metabolite (α-phenyl-2-piperidineacetic acid [PPAA]) concentrations at 0 (predose), 1.5, 2.5, 4.0, 5.5, 6.5, 8.0, 9.5, and 11.5 hours after the morning dose. After centrifuging the blood samples, the plasma was removed, placed into a vial, frozen, and shipped to a central laboratory (Triangle Laboratories, Inc., Durham, NC) for analysis. Plasma samples were analyzed simultaneously for MPH and PPAA by a validated high-performance liquid chromatography tandem mass spectrometry using multiple reaction monitoring method developed for this study. Samples were spiked with the deuterated analogs of d3-MPH and d5-PPAA and extracted using solid-phase extraction cartridges.
The purpose of PK analysis is to describe the time course of plasma drug concentration–time profiles, and there are several ways to describe the PK. Noncompartmental analyses, the approach used in the current study, typically are observation-based and no prediction is done; the PK parameters are descriptive in nature. In a compartmental model analysis, a set of processes are assumed and are described by mathematical models. These models are fitted to the data and parameters are used for both summarizing and predicting exposure statistics. In fitting a model, limited data can sometimes lead to oversimplification of the model describing the true plasma drug concentration–time profile.
In this study, the PK parameters for MPH and PPAA were calculated using noncompartmental methods. A 1-compartment PK model was used to estimate the relative bioavailability for OROS treatments. A population approach utilizing nonlinear mixed modeling (NONMEM®) was used to obtain population estimates.
Pharmacodynamics
Treatment assessments were conducted on Saturdays according to the UC Irvine laboratory school protocol (Swanson et al. 2000, 2002; Wigal and Wigal 2006). Trained observers rated attention and deportment using the Swanson, Kotkin, Agler, M-Flynn, and Pelham (SKAMP) rating scale (Wigal et al. 1998) during individual structured activities within a 30-minute period at 1, 2, 3, 5, 7, 9, 10, 11, and 12 hours after the first dose on each treatment laboratory school day. Results were scored in two subscales: Combined-Attention (i.e., problems leading to decreased academic productivity) and Deportment (i.e., problems leading to classroom disruptions), with higher scores indicating greater impairment (McBurnett et al. 1997; Wigal et al. 1998). Laboratory school teachers also rated the overall effectiveness of treatment at the end of the laboratory school days on a four-point global assessments of efficacy scale with 0 = poor and 3 = excellent.
Activity levels were monitored during individual structured activities during each treatment day. To assess activity, children wore activity monitors (ActiGraph®) throughout the day. Because the appropriateness of a movement depends on the situation and social demands and to allow children to be more settled during the measurement sessions, only the values in the middle 20 minutes of each of nine 30-minute structured activity periods were used for efficacy analysis (Miller and Kraft 1994; Teicher et al. 1996). For each patient, the mean activity level during each of these 20-minute periods was calculated.
Safety
During treatment, investigators actively solicited reports of adverse events that were recorded and assessed for severity and relationship to study medication. Safety assessments also included physical examinations, vital signs, tic evaluations, and complete blood counts at screening and after management with study medication. Vital signs were assessed predose, and then every 1.5 to 2.5 hours until 11.5 hours postdose.
Statistical analysis
Thirty-six patients were to be enrolled to ensure that 15 patients in each study group (30 total patients) completed the three treatment periods of the study and provided evaluable PK and PD data for analysis. Mean PK parameters were compared among treatments within each group of patients. PK parameters evaluated included maximum plasma concentration (Cmax), time to Cmax (Tmax), area under the plasma drug concentration–time curve from 0 to 11.5 hours (AUC(0–11.5)), and bioavailability (%). The study used a 20% criterion to evaluate food effect (i.e., a 20% change in means was considered the criterion for notable change).
SKAMP Combined-Attention assessments from each time point were analyzed to evaluate therapeutic effect throughout the laboratory school day. A mixed-effects analysis of variance model was used for the analysis of the SKAMP and activity monitor data at each time point. Observed means and standard deviations for each treatment over time were computed to evaluate group differences. The analysis of variance model included the fixed-effect factors of treatment, sequence, and period, and the random-effect intersubject and intrasubject factors. Pairwise comparisons were made between OROS MPH and IR MPH at each time point. Statistical tests were assessed at the 0.05 significance level, and all tests were two-sided.
Results
Patients
Thirty-two patients were randomized to treatment, and all but 1 completed all treatment days. One patient discontinued per protocol after completing the first treatment period because of repeated systolic blood pressure measurements >130 mm Hg on day 1 (initial treatment assignment was OROS MPH high-fat breakfast). Of the 31 patients who completed all treatment days, 4 patients were excluded from the comparative noncompartmental PK analysis because they had ≤3 blood samples available during at least one treatment period and therefore had insufficient plasma concentration data. The demographic characteristics of the subjects completing the study are summarized in Table 2.
SD = standard deviation.
Pharmacokinetics
The PK parameters in group 1 (OROS MPH high-fat breakfast and fasting vs. IR MPH fasting) and group 2 (OROS MPH high-fat and normal breakfasts vs. IR MPH normal breakfast) are summarized in Tables 3 and 4, respectively, and Figure 1. Formal statistical analyses to test for the bioequivalence of OROS MPH and IR MPH under various breakfast conditions were not done because there were so few patients in each dose level of treatment. In group 1, PK values for MPH after administration of OROS MPH under high-fat breakfast and fasting conditions were similar to those observed after administration of IR MPH under fasting conditions (i.e., results were within the 20% criterion used to evaluate food effect). The plasma MPH profiles and the mean PK values for MPH after administration of OROS MPH under high-fat and fasting conditions were also similar at each dose level. Similar results were observed for PPAA PK values. The ratio of dose-adjusted Cmax for OROS MPH in the high-fat versus fasting conditions was 1.14 (standard deviation = 0.28), and for AUC the ratio was 1.05 (standard deviation = 0.17). Neither parameter met the 20% criterion for a clinically important difference.
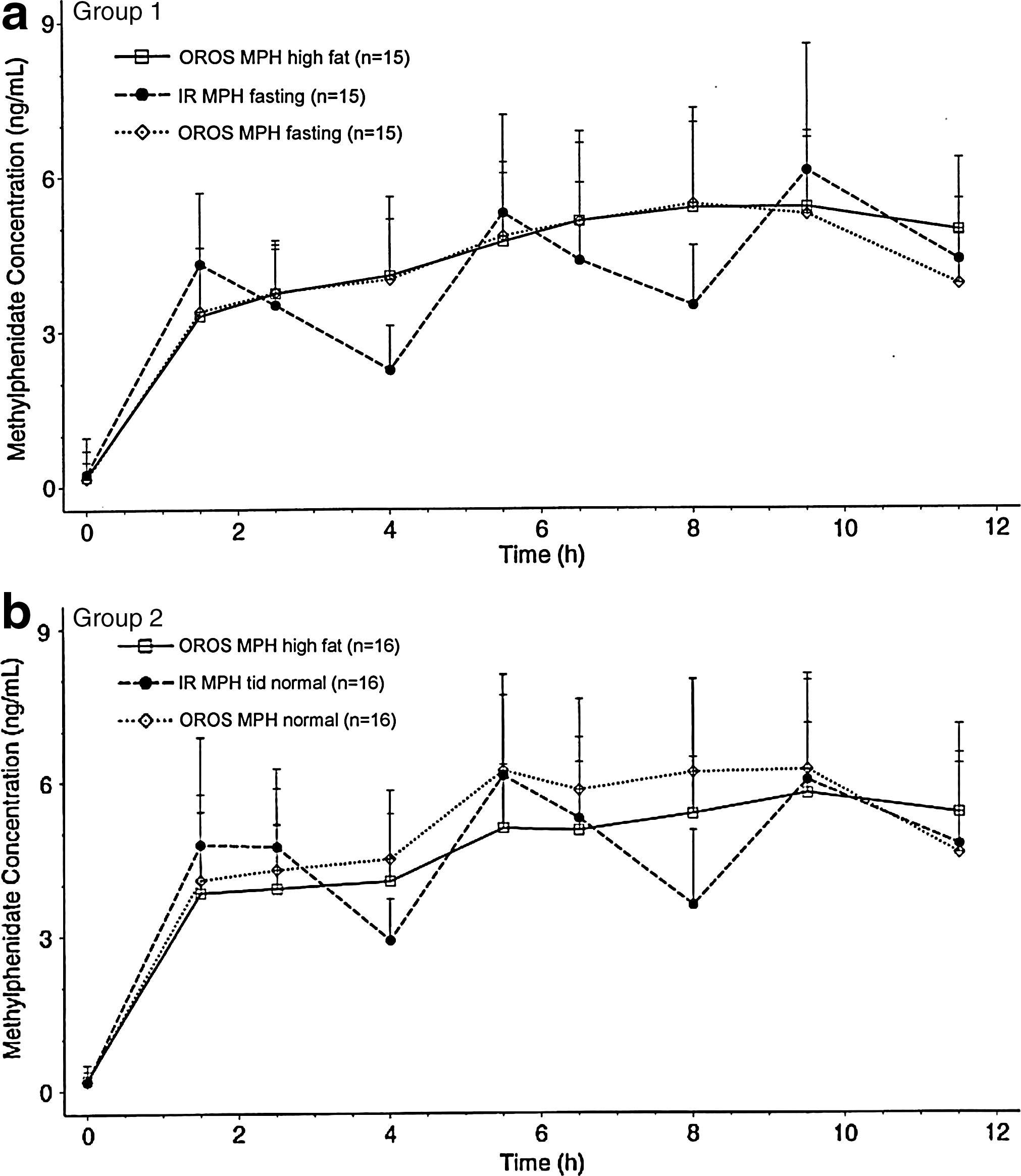
Mean (standard deviation) plasma MPH concentration profiles for group 1
Cmax = maximum plasma concentration; Tmax = time to Cmax; AUC0–11.5 = area under the plasma drug concentration time curve from 0 to 11.5 hours; OROS MPH = OROS® methylphenidate; IR = immediate release; TID = three times daily.
Cmax = maximum plasma concentration; Tmax = time to Cmax; AUC0–11.5 = area under the plasma drug concentration time curve from 0 to 11.5 hours; OROS MPH = OROS® methylphenidate; IR = immediate release; TID = three times daily.
Similar results were observed in group 2, where PK values for MPH after administration of OROS MPH under high-fat and normal breakfast conditions were similar to those observed after administration of IR MPH after a normal breakfast. PK values for PPAA also were similar between treatment groups. Overall, these data suggest that food or type of meal does not affect the PK profile and parameters of MPH after administration of either OROS MPH or IR MPH.
The mean drug-to-metabolite ratios for all treatment groups were similar across administration regimens in both group 1 and group 2 (Table 5). This suggests that there were no apparent differences in drug metabolism between OROS MPH and IR MPH and that food appears to have no effect on drug metabolism.
Mean ± SD for all dose levels.
MPH = methylphenidate; IR = immediate release; TID = three times a day.
Pharmacodynamics
The therapeutic effects of OROS MPH QD and IR MPH TID were similar as assessed by the SKAMP Combined-Attention assessment score (Fig. 2) and the SKAMP Deportment score (Fig. 3), regardless of the breakfast condition. For SKAMP Combined-Attention scores, there were no significant overall differences between treatment groups except for assessments at 1 (p = 0.034) and 7 hours (p = 0.019) in group 1 and at 5 hours (p = 0.033) in group 2. For the SKAMP Deportment subscale, overall scores were also similar between groups except for assessments at 10 hours (p = 0.017) for group 1 and at 1 hour (p = 0.042) for group 2.

Change in mean Combined-Attention scores over time for OROS MPH once daily and IR MPH TID in group 1

Change in mean Deportment scores over time for OROS MPH once daily and IR MPH TID in group 1
Global assessments of efficacy were “good” or “excellent” for the majority (of patients and were similar for all of the treatments (Fig. 4). Results of global assessments showed no statistically significant differences between OROS MPH and IR MPH in either group 1 or group 2.

Global assessments of efficacy: Percentage of subjects rated as “excellent” or “good” by treatment group. No statistically significant differences between OROS MPH and IR MPH TID treatments in either group. MPH = methylphenidate; IR = immediate release; TID = three times a day.
Activity levels, as assessed by actigraphy, were similar between treatment groups. There were no statistically significant treatment differences (p ≤ 0.05); however, greater differences between some treatments were observed for the younger patients in classroom 1 versus classroom 2. It should be noted that there were small numbers of patients in each group and classroom (n = 6–9).
Safety
All treatments were well tolerated. There were no serious adverse events and no deaths reported during the study. Eighteen (56.3%) patients experienced at least 1 adverse event. The percentages of patients experiencing at least 1 adverse event were similar across treatment groups: OROS MPH fasting (20%), OROS MPH high-fat breakfast (22%), OROS MPH normal breakfast (25%), IR MPH TID normal breakfast (25%), and IR MPH TID fasting (33%). The most common adverse events were headache, accidental injury, twitching, and anorexia (Table 6). There was no clear trend in the distribution of subjects who reported at least one adverse event across dose levels.
Adverse events reported in >5% of total subjects. Number for each COSTART term indicates number of patients reporting that event. Patients may be reported under >1 COSTART term.
There were no statistically significant differences in mean systolic or diastolic blood pressure or pulse rate between treatment groups. A majority of patients had at least one blood pressure reading above the 95th percentile for age, sex, and height during the study; however, the majority of all blood pressure measurements were below the 95th percentile. As mentioned previously, one patient had repeated systolic blood pressure elevations above the 95th percentile (121–137 mm Hg compared to 95th percentile of 118 mm Hg) on study day 1 and was discontinued early from the study
Discussion
OROS MPH is an extended-release formulation that is designed to deliver MPH in a controlled manner for ∼10 hours and provide efficacy through 12 hours (Pelham et al. 2001; Swanson et al. 2003; Coghill and Seth 2006; Wigal et al. 2006). QD formulations are more convenient for children who require medication throughout the day and into the evening, but only if they maintain efficacy. OROS MPH is an effective controlled-release formulation and has been associated with improved adherence (Claxton et al. 2001; Swanson 2003; Marcus et al. 2005; Faraone et al. 2007). The OROS formulation of MPH has also been demonstrated to be associated with higher parent preference compared with the IR MPH formulation (Pelham et al. 2001).
This study demonstrated that varying the breakfast conditions (i.e., high-fat or normal breakfast or fasting) had no effect on the PK profile and parameters, and therapeutic effect of MPH in children with ADHD receiving OROS MPH. These results are generally consistent with previous studies evaluating the effect of food on the PK values of OROS MPH or IR MPH (Chan et al. 1983; Modi et al. 2000; Auiler et al. 2002; Teo et al. 2004). For example, Auiler and colleagues (2002) evaluated the effect of a high-fat breakfast on early drug exposure from morning doses of OROS MPH and an extended-release formulation of amphetamine (Adderall XR®) in healthy adult volunteers. Peak (i.e., maximum plasma concentration) and total (i.e., area under the curve) MPH exposure produced by OROS MPH were unaffected by the consumption of a high-fat breakfast (Auiler et al. 2002). In another study, involving 55 healthy adult volunteers, Modi et al. (2000) demonstrated that a high-fat meal had no significant effect on the absorption of OROS MPH at 18 and 36 mg, although peak plasma concentrations and area under the curve values of MPH were 10% to 30% higher and the time to peak concentration occurred ∼1 hour later in the presence of food. The authors concluded that these PK differences were minor and not clinically significant. Similar to the current study, Modi et al. (2000) also found that the MPH-to-metabolite ratios with the OROS delivery system were not affected by food, indicating that food does not affect the metabolism of MPH.
In this study, the relative overall bioavailability of OROS MPH was similar to that of IR MPH under normal breakfast and fasting conditions. These results are comparable to findings in adults regarding relative bioavailability of OROS MPH QD and IR MPH TID (Concerta [package insert] 2010).
The results of this study are consistent with those of previous studies that have demonstrated similar effects of OROS MPH QD and TID MPH in the management of symptoms of ADHD in children (Pelham et al. 2001; Coghill and Seth 2006). Because QD formulations that are administered in the morning may or may not be taken with food, the consistency of drug exposure under a variety of breakfast conditions is important to ensure consistent control of ADHD symptoms. In this study, the statistically significant SKAMP Combined-Attention score differences seen at 1 hour and 7 hours in group 1 and at 5 hours in group 2 appear to be isolated findings that are not indicative of any overall treatment difference. Similarly, SKAMP Deportment scores at 10 hours for group 1 and at 1 hour for group 2 appeared to be isolated findings. Overall, the data suggest that OROS MPH is consistent in its therapeutic effect regardless of breakfast condition.
The safety results seen in this study are comparable to the frequency and severity of adverse events seen in other short- and long-term studies of OROS MPH in children with ADHD (Pelham et al. 2001; Wolraich et al. 2001; Swanson 2003; Wilens et al. 2005). The most common adverse events in this study (for both OROS MPH and IR MPH) included headache, accidental injury, twitching, and anorexia. There were no new safety issues identified during the study, and there were no severe adverse events, except for one patient who was discontinued early because of systolic blood pressure elevations on study day 1.
The study was designed to quantify the magnitude of the difference between treatments. This sample size was enough to determine a difference of 20% or more in PK parameters. The study was not designed to document bioequivalence. Other potential limitations of the study include the short study duration (i.e., the duration may be insufficient to provide comprehensive assessments of efficacy), the small patient population, the lack of a diverse patient population (i.e., patients were primarily white and male), and the lack of a control group (i.e., unmedicated subjects without ADHD) for comparison. Also, an IR MPH TID group that received a high-fat breakfast was not included in the study, which would have added to the comparisons of the PK and PD under different conditions. An inactive (placebo) control condition was not established, so only a positive (IR MPH TID) control condition was available to evaluate the efficacy of the experimental (OROS MPH) condition. The expectation was that the PK results and PD efficacy of OROS MPH would match the TID dosing regimen of IR MPH. There also were limitations inherent to the laboratory school design that could be expected to influence the children's behavior. For example, because all subjects in the laboratory classroom had ADHD, the dynamics of the classroom were likely different from those of a normal classroom. Further, the number of observers in the laboratory classroom was higher than the number in the traditional classroom, which may indirectly influence the subjects' behavior.
The results of this study may not be generalizable to other age groups. The obvious assumption is that food does not affect the exposure of MPH or its effects on behavior in adolescent or adults, but the effect of food on the PK and PD of OROS MPH would need to be evaluated in these patient populations to support this conclusion.
Conclusions
The PK and PD parameter values after OROS MPH treatment after a high-fat breakfast, a normal breakfast, and fasting state were similar. This demonstrates that food does not affect the PK or PD values of OROS MPH in children with ADHD. The efficacy and safety of OROS MPH treatment were similar in all three conditions, demonstrating that food does not appear to have an effect on efficacy or safety of OROS MPH in children with ADHD. These results demonstrate that OROS MPH is similar to IR MPH TID in providing efficacy and that food does not have an effect on efficacy.
Footnotes
Disclosures
The study was sponsored by ALZA Corporation Mountain View, CA. Sharon Wigal, Ph.D., is an Advisory Board Member/Consultant for Abbott, ALZA, Celgene, Celltech, Cephalon, Eli Lilly, McNeil Consumer & Specialty Pharmaceuticals, Next Wave Pharm., NIMH, Novartis, Shire US Inc., and TAISHO; receives research support from Addrenex, ALZA, Celgene, Celltech, Cephalon, Eisai, Eli Lilly and Company, Gliatech, McNeil Consumer & Specialty Pharmaceuticals, NIMH, Novartis, Psychogenics, Quintiles, Shionogi Pharma, Shire US Inc., and Sigma Tau; and is a member of Speaker's Bureaus of ALZA, Cephalon, McNeil Consumer & Specialty Pharmaceuticals, Novartis, and Shire US Inc.
Suneel Gupta, Ph.D., is an Employee of Impax Pharmaceuticals. Previously, he was an employee of ALZA and Johnson & Johnson, who are the developer and marketer of Concerta. H. Lynn Starr, M.D., and Erica Heverin, PharmD, are employees of Ortho-McNeil Janssen Scientific Affairs, LLC, and stockholders of Johnson & Johnson Corporation.
Author roles in the production of this article include the following: Erica Heverin for contributions to the interpretation of the results and writing of the article; H. Lynn Starr for contributions to the interpretation of the results, writing of the article, and oversight of the publication.
Acknowledgments
Ortho-McNeil Janssen Scientific Affairs, LLC, Raritan, NJ, and McNeil Pediatrics, a Division of McNeil-PPC, funded the editorial, writing, and technical assistance provided by Wynne Dillon and Ellen Stoltzfus, Ph.D., from JK Associates, Inc., in the completion of this article. The study was sponsored by ALZA Corporation Mountain View, CA. The authors would like to acknowledge the work of James Swanson, Ph.D., University of California, Irvine, in the development of the study and its design, Erick Fineberg, M.A., Ed, Irvine, CA in study coordination, and Dolly A. Parasrampuria, Ph.D., and Steve Ascher, Ph.D., Johnson & Johnson Product Research and Development, for their contributions to the article. At the time of publication, Dolly A. Parasrampuria was no longer an employee of Johnson & Johnson Product Research and Development.