
Abstract
Objective:
To evaluate the type, frequency, duration, and severity of treatment emergent adverse events (TEAEs) of the prodrug lisdexamfetamine dimesylate (LDX) in children with and without previous exposure to stimulant medication in the treatment of attention-deficit/hyperactivity disorder (ADHD).
Methods:
This single-blind, modified laboratory school study used open-label, dose optimization of children aged 6–12 years. LDX, initiated at 30 mg, was dose titrated in 20 mg increments to a possible 70 mg over 4–5 weeks. Safety was assessed using adverse effects and LDX levels.
Results:
Twenty-eight subjects enrolled in the study, with 27 safety protocol completers (n=14 previous stimulant exposure; n=13 stimulant naïve). The stimulant-naïve group reported more trouble sleeping, stomach pain, and hyperfocus, but only previous-exposure subjects experienced dizziness. Previous-exposure subjects showed trends of more decreased appetite, less talkativeness, and less lip sucking. There were no differences in the mean duration of TEAEs. The epidemiological method of percent person-weeks applied to ADHD treatment offers a novel approach to interpreting the pattern of TEAEs.
Conclusion:
LDX reduced the core symptoms of ADHD with more severe adverse events in stimulant-naïve than previous-exposure subjects. Future controlled studies with larger samples should address the impact of previous stimulant exposure on other ADHD treatments.
Introduction
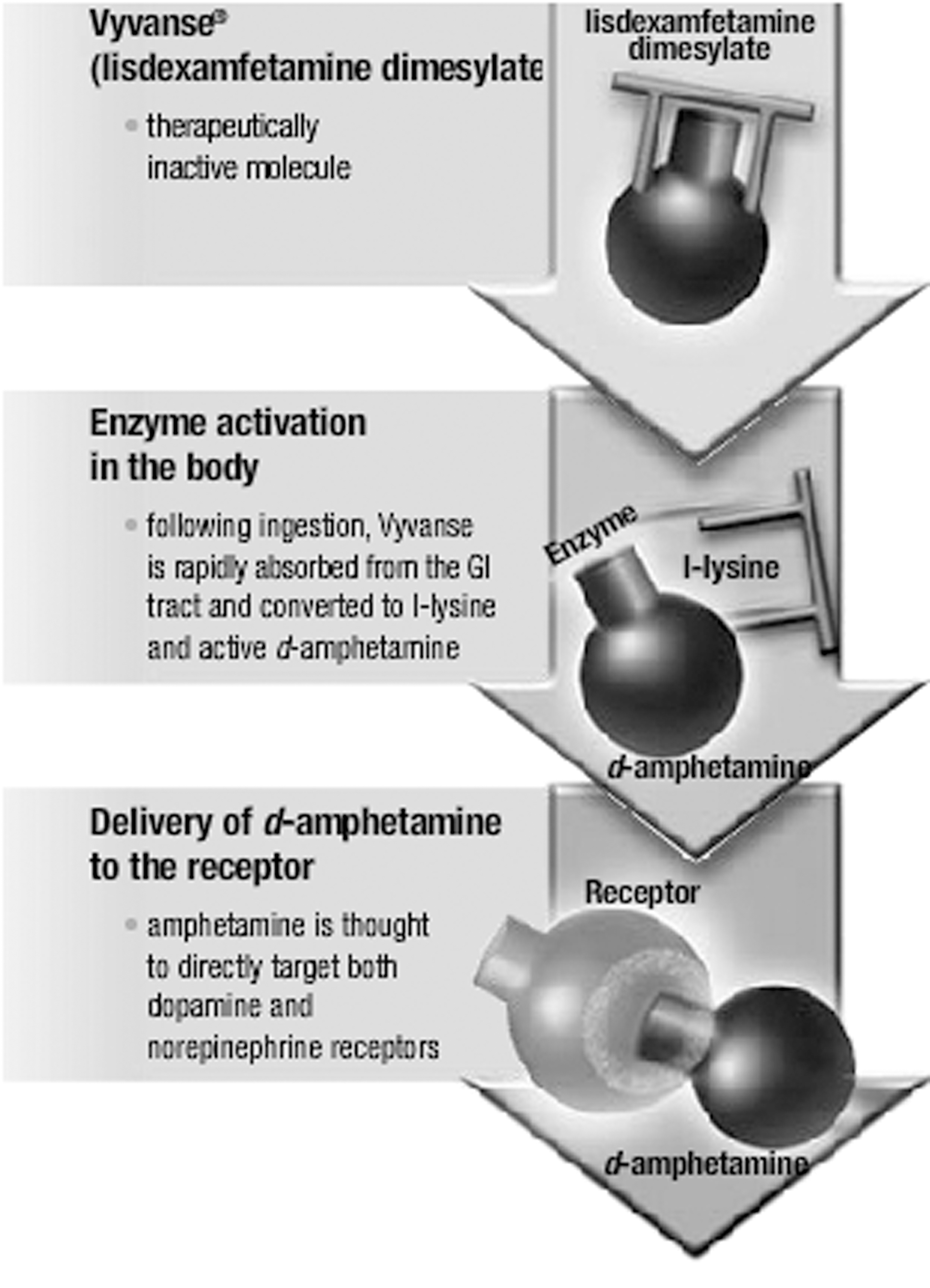
Conversion of LDX into
There is a lack of comparator treatment studies in children with ADHD that address previous medication history. For instance, the Multimodality Treatment Study of Children with ADHD (MTA) (e.g., MTA Cooperative Group 1999) is the largest ADHD clinical trial to date with 579 participants and 215 (37%) stimulant naïve. Exposure (no medication vs. medication) before MTA study enrollment was briefly described as related to growth trajectories (Swanson et al. 2007). However, detailed secondary analyses of AEs based on prestudy stimulant exposure status have not been presented or published.
One previous, unpublished presentation on LDX treatment (Biederman et al. 2007b) showed that the majority of treatment-related AEs occurred within the first week of treatment. The most common AEs were decreased appetite, insomnia, upper abdominal pain, and headache, and there was a general trend toward higher AE rates in the “not recently treated” group compared with the stimulant treatment group. However, participants were not truly treatment naïve, but rather had limited treatment exposure in the past 12 months before participation. A report on the efficacy and tolerability on modafinil, a nonapproved ADHD treatment (Wigal et al. 2006), pooled data across several clinical trials to compare previously stimulant treated patients with patients who either were stimulant naïve or previously treated with ADHD medications other than stimulants combined as a previous exposure group. The overall conclusion was that treatment improvements were more robust for medication or stimulant-naïve patients than those who received stimulant treatment earlier but that all subjects experienced modafinil-associated improvement in ADHD symptoms. In addition, those patients with previous stimulant exposure reported less AEs than those in the medication- or stimulant-naïve group.
Since there is no published research on the adverse effects of LDX treatment in true stimulant-naïve subjects versus those with previous exposure to stimulants, secondary analyses were conducted to investigate the safety profile of LDX. The safety data were originally collected as part of a study on reading performance in response to stimulant treatment (Wigal et al. 2010c). Data corresponding to adverse event (AE) monitoring including weight assessment are presented in the current article. Although examination of additional physiological measures (blood pressure, heart rate, electrocardiography, and laboratory) is presented in a separate paper (Wigal et al. 2010a), a brief synopsis of these and the efficacy findings are included in the present article for the ease of the reader. The design of the original study was dose optimization rather than forced dose titration, starting with a 30 mg dose and titrating up to a maximum of 70 mg during subsequent study weeks if needed. A benefit of this approach is that it better reflects what occurs in naturalistic medical visits. By incorporating epidemiologic methods (Cascade et al. 2010), we can address the varied drug exposure times that result from participants titrating individually.
The present post hoc analysis of a clinical study describes the type, frequency, duration, and severity of treatment-emergent adverse events (TEAEs) of LDX in 27 children aged 6 to 12 years in whom ADHD was diagnosed. Two naturalistic subgroups were identified based on a parental report of stimulant exposure before study entry. We hypothesized that stimulant-naïve status would be associated with a greater incidence, longer duration, and greater severity of TEAEs while taking LDX than subjects with previous stimulant exposure.
Methods
The study protocol was approved by the University of California (UC), Irvine local institutional review board, and the State Research Advisory Panel of California. All parents or caregivers gave written informed consent, and the subject's assent was obtained before any study-related procedures were performed. All study activities were performed in accordance with good clinical practice guidelines and in accordance with the Declaration of Helsinki and its amendments and applicable local regulations. Shire Development Inc. provided study medication and support for study-related care. In addition, parent(s)/legally authorized representatives of participating children signed an Authorization of Release of Personal Health Information for Research Purposes (HIPAA) form when giving legal informed consent for participation in the study.
Subjects
A total of 28 eligible subjects aged 6 to 12 years at the time of consent were enrolled (with 27 safety completers) who had a diagnosis of ADHD confirmed at the time of screening based on structured clinical interviews of Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV TR) (American Psychiatric Association 2000). All subjects had total scores of at least 1.5 standard deviations (SDs) above the subjects' age and gender norms on the Clinician administered ADHD Rating Scale-Version IV (ADHD-RS-IV) at baseline (DuPaul et al. 1998). Subjects were also required to be intellectually functioning at an age-appropriate level as determined by an intelligence quotient (IQ) score of ≥80 on the Kaufman Brief Intelligence Test (Kaufman and Kaufman 2006). Excluded from the study were potential subjects who had additional clinically significant psychiatric illness (other than oppositional defiant disorder) indicated by the Kiddie-Schedule for Affective Disorders and Schizophrenia-Present and Lifetime Version psychiatric evaluation (Kaufman et al. 1997), and/or clinically significant chronic medical conditions. Subjects with a history of no response or intolerable adverse effects to amphetamine treatment were excluded as well for ethical reasons. Subjects were not recruited to the study based on treatment history of stimulant naïve and previous stimulant exposure. However, there was a fairly balanced distribution of subjects across the two subgroups.
Study design
This single-blind, modified laboratory school study (Wigal and Wigal 2006) of LDX was conducted as a single-site study at UC Irvine. After screening for ADHD, eligible participants were washed out from their previous ADHD treatment (if applicable), completed a baseline visit, and then started on LDX during an open-label dose optimization period (4–5 weeks in duration). Subjects were titrated from a starting dose of 30 mg LDX by 20 mg increments to a maximum dose of 70 mg or downward titrated (only one such dose reduction permitted) based on Clinical Global Impressions severity and improvement scores, with the latter reaching scores of 1 (very much improved) or 2 (much improved) since initiation of treatment, ADHD-RS-IV scores that were reduced to ≥30% and tolerability of AEs until reaching an acceptable response. Ratings were completed by licensed practitioners who were blinded to treatment conditions. The LDX dose administered at Visit 3 was determined to be the subject's optimal dose and was also administered at the final clinic, Visit 4. Figure 2 depicts the study visit schedule with each visit ∼1 week apart. AEs were elicited by open-ended general inquiry as well as spontaneous reporting of AEs by the child and/or parent rather than a specific interview with a detailed, structured interview format (Rabkin et al. 1992; Greenhill et al. 2003). The AEs were described or ranked by study physicians in terms of duration (beginning and end date), severity (mild, moderate, severe, and serious), and relation to the study medication (with TEAEs defined as study medication related AEs with an onset after exposure to treatment; e.g., Wigal et al. 2009).
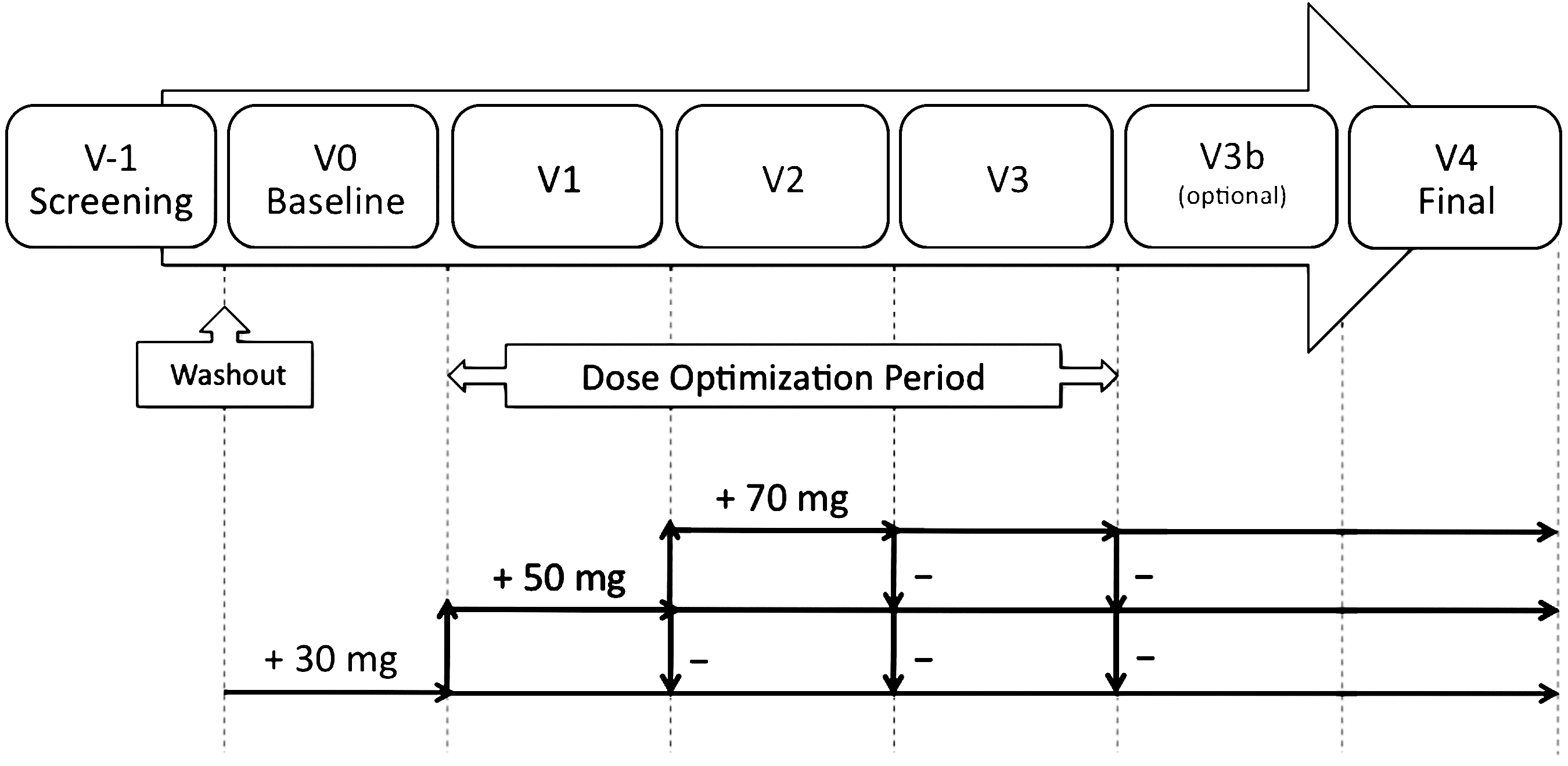
Study design.
Statistical analysis
Post hoc subgroup analyses were conducted to examine the existence of group differences between the two exposure groups, and stratified descriptive statistics were calculated. Continuity-corrected Chi-square tests were performed for those TEAEs with at least a 10% incidence to examine whether there were differences in reporting rates between the two groups. t-tests were used to evaluate group mean differences in the continuous measures (i.e., duration and count totals). Since this study's dose-optimization design allowed for subjects to increase or decrease in dose as needed at the start of each study week, the epidemiologic measure “person-weeks” was calculated to denote the sum of study weeks that the subjects were exposed to specific LDX doses (Cascade et al. 2010). This measure is a form of “person-time” defined as the sum of individual units of time that the persons in the study population have been exposed to a condition of interest (Hennekens and Buring 1987; University of Michigan 2010). Thus, at each dose, incidence rates were calculated by dividing the number of AEs reported at that dose by the “person-weeks” of exposure.
Results
A total of 28 subjects enrolled in the study and were exposed to LDX. Of the original 28 subjects, 2 stimulant-naïve subjects terminated early from the study after LDX treatment: 1 with a TEAE of extreme talkativeness (included in the study sample); and 1 with withdrawn parental consent (not included in the study sample). Subjects with previous stimulant exposure composed 51.9% (n=14), while the stimulant-naïve group made up 48.1% (n=13). See Table 1 for the demographics of the total study population and the breakdown of characteristics by previous-exposure and stimulant-naïve groups. LDX significantly reduced total symptoms as well as hyperactive/impulsive and inattentive symptoms of ADHD from Baseline to the Final visit. In these same subjects, LDX treatment resulted in some improvement of reading performance: Reading rate, not reading accuracy, or reading comprehension improved in the short-term by controlling inattentive symptoms (see Wigal et al. 2010c for the complete report of LDX efficacy).
SD=standard deviation; ADHD-RS-IV=Attention-Deficit/Hyperactivity Disorder Rating Scale-Version IV.
Overall, 19 subjects had an optimal dose of 30 mg LDX (70.4%), 6 ended up at 50 mg LDX (22.2%), and 2 ended up at 70 mg LDX (7.4%); see Table 1. Only two subjects titrated up to the 70 mg dose, and they were both not only previous-exposure subjects but also heavier subjects (85.49 and 73.06 pounds).
Incidence of AEs
The total number of TEAE incidents reported across the study period was 118. The median number of incidents per person was four. Reporting rates for the most common TEAE's are presented for each exposure group in Table 2. Fifty-nine percent of all AE incidents occurred in the stimulant naïve-group. The stimulant-naïve group as well as the previous-exposure group reported trouble sleeping and stomach pain with a greater incidence for stimulant-naïve subjects (p=0.004, and p=0.0034, respectively). Hyperfocus (p=0.025) was only seen in the stimulant-naïve subjects. Only previous-exposure subjects experienced dizziness (p=0.037), with a trend toward more reports of decreased appetite. Previous-exposure subjects actually displayed a trend toward fewer incidents of talkativeness, and fewer problems with sucking lips.
p<0.05 level.
Since weight loss is commonly reported with stimulant treatment, and >5% weight loss can affect medical outcomes (Sermet-Caudelus et al. 2000), the AE of weight loss is included here. Six previous-exposure subjects and five stimulant-naïve subjects experienced >5% weight loss. Of note is that there was no significant difference in weight loss between the two exposure groups.
Duration of AEs
TEAEs lasted between 1.0 and 30.0 days overall. Since the number of incidents is relatively small without regard to individual participants, their presentation is for qualitative review (see details in Table 3).
Severity of AEs
There were no serious AEs that would lead to hospitalizations or deaths during this study. Across participants, 118 TEAEs were recorded: 72% mild, 24.6% moderate, and 3.4% severe. Stimulant-naïve subjects were statistically more likely to have a severe AE while taking LDX (p=0.041). All four severe TEAEs were reported by stimulant-naïve subjects: two subjects with trouble sleeping, one subject with hyperfocus, and one subject with extreme talkativeness leading to early termination from the study. No severe AEs were recorded in previous-exposure subjects. Person-weeks were defined as the number of study weeks that subjects were administered specific LDX doses. The incident rate for TEAEs by severity during the cumulative person-time exposure to each of the LDX doses across all subjects is depicted in Figure 3.
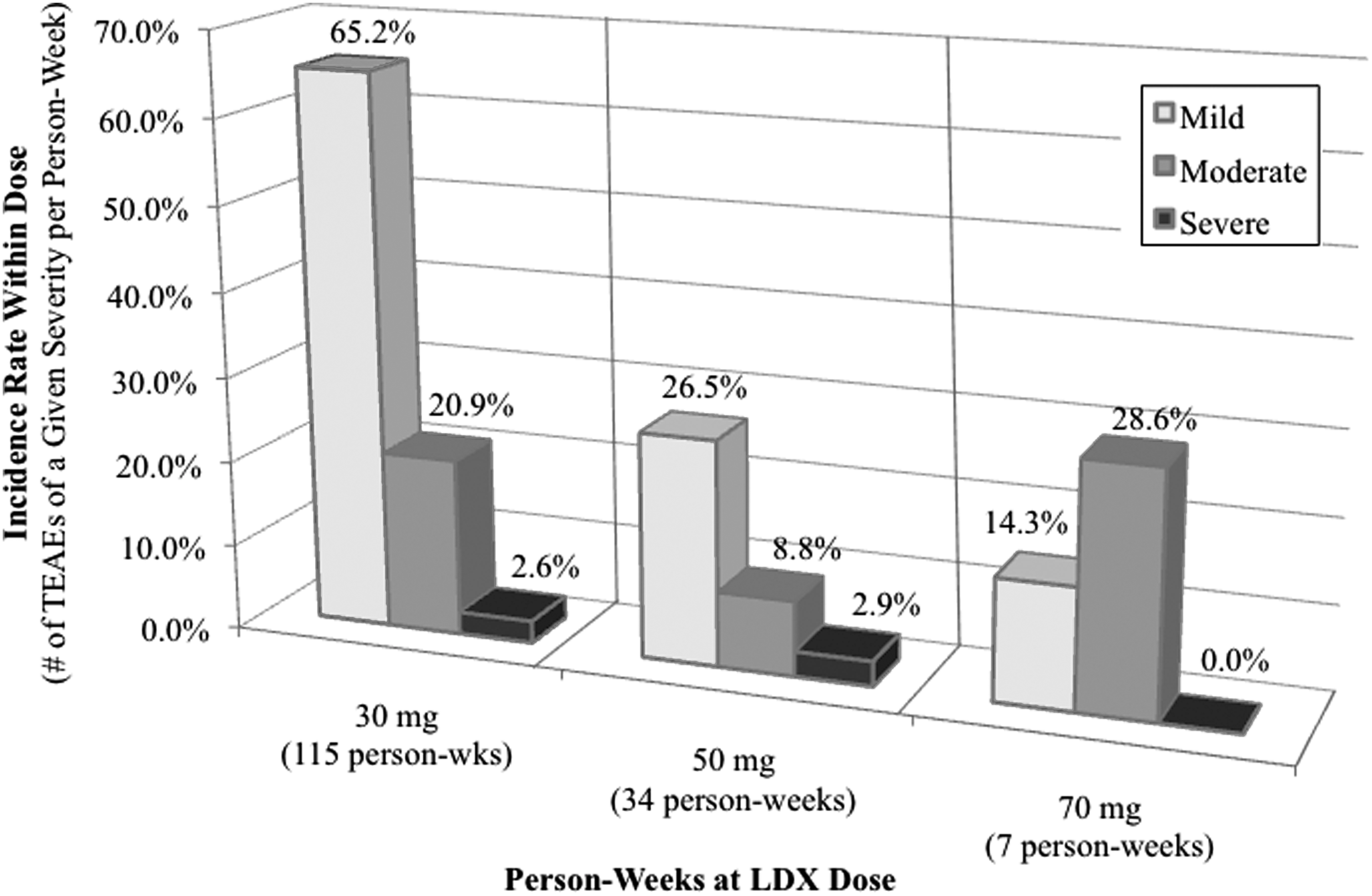
Incidence rate of TEAE severity within dose using person-weeks. TEAE=treatment emergent adverse event.
Discussion
As in other published studies of LDX in this age group (e.g., Biederman et al. 2007a; Wigal et al. 2009, 2010b, 2010c), the present study demonstrated significant improvement of ADHD symptoms with LDX treatment, and overall, LDX was well tolerated. The most common TEAEs reported in this study were decreased appetite, trouble sleeping, stomach pain, irritability, talkativeness, moodiness, vomiting, and headache, which overlap with the most common AEs previously reported (Biederman et al. 2007a, 2007b; Wigal et al. 2009).
In the present study, there was clearly a greater incidence of TEAEs among stimulant-naïve patients than previous-exposure patients. Although previous exposure to stimulant medication also affects the severity of TEAEs associated with LDX, it does not appear to affect the duration. More research is needed to determine whether a greater incidence of TEAEs in stimulant-naïve populations is also true for exposure to other stimulant treatments, is specific to amphetamines, or is unique to LDX. A placebo treatment reference arm should be included in future studies designed to specifically examine such subgroup differences to better understand the contribution of specific medications versus treatment in general on TEAEs. Thus, additional research specifically designed to characterize samples of children in this way may address whether previous medication status is an important modulator of treatment response to predict more positive efficacy and/or greater severity of TEAEs. For instance, Spencer et al. (2001) reported more robust responses to atomoxetine in stimulant-naïve patients although both those patients with and without previous exposure to stimulants responded well to atomoxetine. A recent study identified patient characteristics in the indication of schizophrenia that predicts subsequent switching of treatments (Nyhuis et al. 2010). One of the top six variables identified was the lack of antipsychotic use in the previous year. These papers coupled with our findings raise the need to clarify the role of previous treatment to systematically evaluate both positive and negative efficacy and safety reporting.
Although there appears to be a large number of TEAEs in this study, such risks did not outweigh the benefits of LDX treatment. In fact, most of the TEAEs occurred at 30 mg, and they were mild in severity and could be monitored by physicians, parents, and legally authorized guardians. The benefit from LDX treatment is evident in this small, but well-characterized, group of children with ADHD: ADHD-RS-IV scores (SD) reduced from 43.07 (5.19) at baseline to 10.19 (5.42) by the final visit. Despite the TEAEs, subjects were able to continue with the LDX treatment and titrate to their clinically best dose to reduce their ADHD symptoms, with the tendency for previous-exposed participants to be titrated to higher doses of LDX than those who were treatment-naïve (Wigal et al. 2010a). No significant differences in pulse and blood pressure results were present between exposure groups at baseline or at the end of the study, and benign cardiovascular findings support the continued practice of reviewing family history of cardiac issues in pediatric and psychiatric clinical settings (American Academy of Pediatrics/American Heart Association 2008; Elia and Vetter 2010).
This study also demonstrates new methods of reporting TEAEs by person-week (Cascade et al. 2010) as well as analyzing TEAEs by dose, neither of which is usually presented. Although most ADHD clinical trials report the severity of the AEs experienced by the subject population, they typically do not report their frequency, duration, or corresponding dose. In addition, the reporting of such AEs typically is secondary to the primary research question rather than the focus of a priori hypotheses, or, as in the present study, post hoc subgroup analyses. One reason that research on exposure groups and specifically on AEs in detail may be rare is because study of AEs requires detailed reporting, close observation, and can be influenced by many variables, such as how to standardize severity between subjects. In addition, analyzing AEs by incidence rate is a new method to closely evaluate the dose response, especially in dose-optimized study protocols where subjects are not all exposed to the same dose of study drug for equal periods of time. This analysis is especially important, because dose titration closely mimics medication management in clinical settings. It also provides a way to link dose and severity to determine at which dose (in this case, for LDX), the most severe AEs are reported.
As with any clinical research, AE reporting is dependent on the reliability and recall of subjects and/or their parents or guardians. Another observation is that because parents of stimulant-naïve subjects are not experienced in close observation of daily medication treatment effects, their participation in clinical research actually serves to educate them on how to more objectively evaluate their child's benefits and AEs. For instance, stimulant treatment may have favorable outcomes on baseline characteristics of ADHD that are not AEs as typically understood (Sonuga-Barke et al. 2009). So whether, in this study, LDX treatment effects reflect primarily direct pharmacological activity versus secondary effects on ADHD symptoms is not understood. Parent accuracy in AE reporting may actually increase with study participation, although this was not measured. In addition, the initial clinical presentation of AEs commonly associated with stimulant medications, even one of mild severity, might be considered by family members of stimulant-naïve children to be a more severe event and they may tend to be reactive to all AEs than families of previous-exposed children. Parents of treatment naïve children may initially be more cautious about their child's treatment, and, therefore, may be more accepting of modest benefits. Over time and with more experience, such parents may realize the increased need for higher medication doses in order to further treatment benefits for their child. Those with previous exposure or parents familiar with treatment effects tend not to overreact to minor changes.
Limitations of this study include the small sample size, particularly among female subjects as is typically seen with ADHD (American Psychiatric Association 2000), only one of whom had previous stimulant exposure. In addition, as in the MTA study (Swanson et al. 2007), naturalistic subgroups were compared, and there is a lack of random assignment to these subgroups. In the present study, all subjects received LDX treatment (unlike the assignment of initial treatment conditions and then choices over time in the MTA). Randomization to placebo and LDX within each of the two exposure groups, naïve or treated, would allow the comparison to adjust for any potential placebo effects that differ in parallel. Such a study design would also minimize the potential impact of self-selected subjects level of willingness to participate or not due to prior positive or negative treatment experience. In addition, the inclusion of an untreated group as well as a longer medication exposure time period (i.e., >4–5 weeks) and the inclusion of other active comparator treatments would strengthen future investigations. This requires a larger sample size that would diminish “undue inference” or the likelihood of possible chance findings due to increasing the number of post hoc comparisons (Freemantle, 2001). Finally, interpretation of dose relationship to AEs may be affected by the dose-titration sequence, which in the present study, was not a forced dose titration study. Typically, this would be problematic for interpretation, because duration at each dose and even the delivery of higher doses across participants are uneven in dose optimization protocols. This underscores the value of calculating incidence rate to equilibrate the exposure time at each dose with AE recording.
Conclusion
Future research with exposure groups taking other ADHD medications or intermediate doses of LDX may provide patients and their families with better means to tolerate and manage AEs. Since LDX has a relatively low incidence and severity of TEAEs among subjects with previous exposure to stimulants, and because of its unique prodrug formulation, LDX may be a good treatment choice for patients who currently are untreated for ADHD symptoms or who are unsatisfied with their current ADHD therapy due to factors such as insufficient time course or AEs. Multiple measures (incidence, duration, severity, and incidence rate) provided a better understanding of the clinical impact of TEAEs.
Clinical Significance
LDX was efficacious, and ADHD symptom improvements were not related to previous stimulant treatments, making LDX a possible treatment option for both previously stimulant-treated and stimulant-naïve children with ADHD.
Disclosures
Dr. Sharon B. Wigal is a consultant for Abbott, McNeil, NeuTec, Shire, Taisho, and the NIMH; has received grant/research support from Addrenex, Eli Lilly, McNeil, Next Wave Pharmaceuticals, Otsuka, Psychogenics, Quintiles, Rhodes, Shionogi Pharm., Shire, NICHO, and the NIMH; is on the speaker or advisory boards for McNeil, the NIMH, Shire, Next Wave Pharmaceuticals, Shionogi Pharm., and UCB.
Dr. Marc Lerner is a consultant for McNeil, and Shire; has received grant/research support from Addrenex, Eli Lilly, McNeil, Next Wave Pharmaceuticals, Psychogenics, Quintiles, Rhodes, Shionogi Pharm., Shire, and the NIMH; is on the speaker or advisory boards for Eli Lilly, McNeil, and Shire.
Dr. Robin Steinberg-Epstein is a consultant for McNeil, and Shire; has received grant/research support from Addrenex, Eli Lilly, McNeil, Next Wave Pharmaceuticals, Psychogenics, Quintiles, Rhodes, Shionogi Pharm., Shire, and the NIMH; is on the speaker or advisory boards for Eli Lilly, McNeil, and Shire.
The study sponsor approved the study design; however, the collection, analysis, and interpretation of data were made by the independent authors, as was the writing of this article and the decision to submit this article for publication in Journal of Child and Adolescent Psychopharmacology.
Footnotes
Acknowledgments
The authors would like to acknowledge Audrey Kapelinski and Stephanie Maltas for their contributions to this research.