
Abstract
Objective:
The aim of this study was to evaluate the effects of aripiprazole treatment on individual Young Mania Rating Scale (YMRS) line items in pediatric subjects with manic or mixed episodes associated with bipolar I disorder to better understand the discrete symptom improvements.
Methods:
This was a post hoc analysis of the YMRS line item data from a 4-week, multicenter, randomized, double-blind, placebo-controlled study. Two hundred ninety-six eligible subjects were randomized to aripiprazole 10 mg/day (n = 98), aripiprazole 30 mg/day (n = 99), or placebo (n = 99). The primary endpoint was the mean change in YMRS total scores from baseline to week 4. Effect sizes and treatment effect on individual line items were calculated.
Results:
Of the 296 subjects, 237 (80.1%) completed the 4-week study. Seven of the 11 YMRS line items showed a statistically significant improvement in both aripiprazole treatment groups versus placebo. Using the data for the pooled doses, the three YMRS line items with the greatest effect size at week 4 were irritability (effect size = 0.7; treatment effect = 1.43; p < 0.001), aggressive behavior (effect size = 0.7; treatment effect = 1.38; p < 0.001), and increased motor activity/energy (effect size = 0.6; treatment effect = 0.86; p < 0.001).
Conclusion:
Aripiprazole improved a broad spectrum of symptoms across the YMRS scale.
Introduction
The need for safe and effective therapies for bipolar I disorder has been well recognized. Psychotherapeutic, psychosocial, educational, and pharmacotherapeutic interventions are currently available for the treatment of bipolar I disorder in pediatric patients (Chang 2008). Indeed, with the rise in recognition of pediatric bipolar disorder, there is an increase in the need for validated treatment approaches. Among pharmacotherapeutic options, atypical antipsychotics have been recognized as having a role in treatment, and there are currently four FDA-approved medications for this population: aripiprazole, olanzapine, quetiapine, and risperidone (Abilify 2009; Seroquel 2009; Risperdal 2010; Zyprexa 2010).
Aripiprazole is an atypical antipsychotic with a novel mechanism of action, exerting partial agonist activity at dopamine D2 and D3 and serotonin 5-HT1A receptors and antagonist activity at 5-HT2A receptors (Burris et al. 2002; Jordan et al. 2002; Shapiro et al. 2003; Jordan et al. 2004; Tadori et al. 2008). Aripiprazole has shown efficacy in reducing Young Mania Rating Scale (YMRS) total scores in pediatric subjects in multiple studies (Biederman et al. 2007; Findling et al. 2009; Tramontina et al. 2009).
This report describes a post hoc analysis of results from a pivotal trial (Findling et al. 2009) evaluating aripiprazole for the treatment of an acute manic or mixed episode associated with bipolar I disorder in pediatric patients aged 10–17 years. The primary efficacy outcome measure in that trial was the total score of the 11-item YMRS, a validated measure recommended for the evaluation of treatment effects on mania symptom severity (Tohen et al. 2009). Because the YMRS total score represents a collection of several different discrete symptoms, which may themselves have a varying response to treatment, we conducted a post hoc analysis of the individual YMRS line items to better understand which particular symptoms of mania are affected (or not) by aripiprazole treatment.
Methods
This is a post hoc analysis of the YMRS line item data from a multicenter, randomized, double-blind, placebo-controlled, 4-week study. The study compared aripiprazole (10 or 30 mg/day) versus placebo for the treatment of outpatient and hospitalized, or partially hospitalized, pediatric subjects (10–17 years) with bipolar I disorder experiencing a manic or mixed episode. Full methodology has been previously described (Findling et al. 2009).
The Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR) diagnosis of bipolar disorder, manic or mixed episode, with or without psychotic features for each subject was made by a board-certified or eligible child and adolescent psychiatrist. The diagnosis was then confirmed using the Schedule for Affective Disorders and Schizophrenia for School Aged Children: Present and Lifetime Version at the time of screening. A five-member, independent Data Safety Monitoring Board provided frequent assessment of subject safety.
After screening and medication washout, subjects were randomly assigned to target doses of aripiprazole (10 or 30 mg/day) or matching placebo once daily for 4 weeks. Study medication could be administered at any time of day without regard to meals. Aripiprazole dosing started at 2 mg/day (days 1 and 2), 5 mg/day (days 3 and 4), and 10 mg/day (day 5). Subjects in the 10 mg/day group remained at that target dose, and titration continued for the 30 mg/day group with 10 mg/day (days 5 and 6), 15 mg/day (days 7 and 8), 20 mg/day (days 9 and 10), and 25 mg/day (days 11 and 12) and concluded with the target dose of 30 mg/day on day 13. Matching placebo was administered according to the same titration schedule. Study medication was dispensed at weekly visits in child-resistant blister cards containing a 1-week supply.
The primary endpoint was the mean change in YMRS total scores to week 4. Mean changes from baseline to endpoint in the YMRS total score and individual items, in both aripiprazole treatment arms combined and each treatment arm versus placebo, were compared using analysis of covariance (ANOVA) using the last observation carried forward for dataset, with baseline measurements as a covariate and treatment arms as main effects. Treatment effect was calculated as the difference between the aripiprazole (10 or 30 mg/day) arms and placebo arm on those measures. Cohen's d effect sizes at week 4 were calculated using the following formula: 2*t/(d.f.), where t is the t statistic derived from an ANOVA model with treatment as a factor and d.f. is the degrees of freedom. Safety assessments included the frequency and severity of treatment-emergent adverse events (TEAEs) and discontinuation due to TEAEs, among others.
Results
Subject characteristics
The baseline demographic characteristics of subjects are shown in Table 1. A total of 413 subjects were screened, and 296 subjects were randomized in this study and included in the efficacy sample: 98 to the aripiprazole 10 mg/day arm, 99 to the aripiprazole 30 mg/day arm, and 99 to the placebo arm. A total of 294 subjects (99.3%) were treated and included in the safety analyses; two subjects from the placebo arm were excluded from the safety analyses because they did not receive at least one dose of study drug. A total of 237 (80.1%) subjects completed the 4-week study.
SD=standard deviation.
YMRS total score results
Aripiprazole 10 and 30 mg/day provided significant improvements in YMRS total score from baseline to week 4 compared with placebo (p < 0.001). Mean changes in YMRS total score from baseline to week 4 were −14.2 with aripiprazole 10 mg/day, −16.5 with aripiprazole 30 mg/day, and −8.2 with placebo (both p < 0.001 aripiprazole vs. placebo). Pooled data for both groups of aripiprazole-treated subjects showed statistically significant greater decreases than placebo in the YMRS total scores starting at week 1 and at each time point thereafter.
Line item analyses
Mean change from baseline to week 4 by treatment group (10 or 30 mg/day) versus placebo for individual YMRS line items are shown in Figure 1A. Seven of the 11 line items showed a statistically significant improvement in both the aripiprazole treatment groups (10 and 30 mg/day) compared with placebo. The seven items showing improvement were elevated mood, increased motor activity/energy, sleep, irritability, speech, language/thought disorder, and aggressive behavior. The YMRS line item abnormal thought content also showed statistically significant improvement with aripiprazole 30 mg/day compared with placebo. Effect sizes by treatment group (10 or 30 mg/day) compared with placebo are shown in Figure 1B.

Young Mania Rating Scale line item analysis of
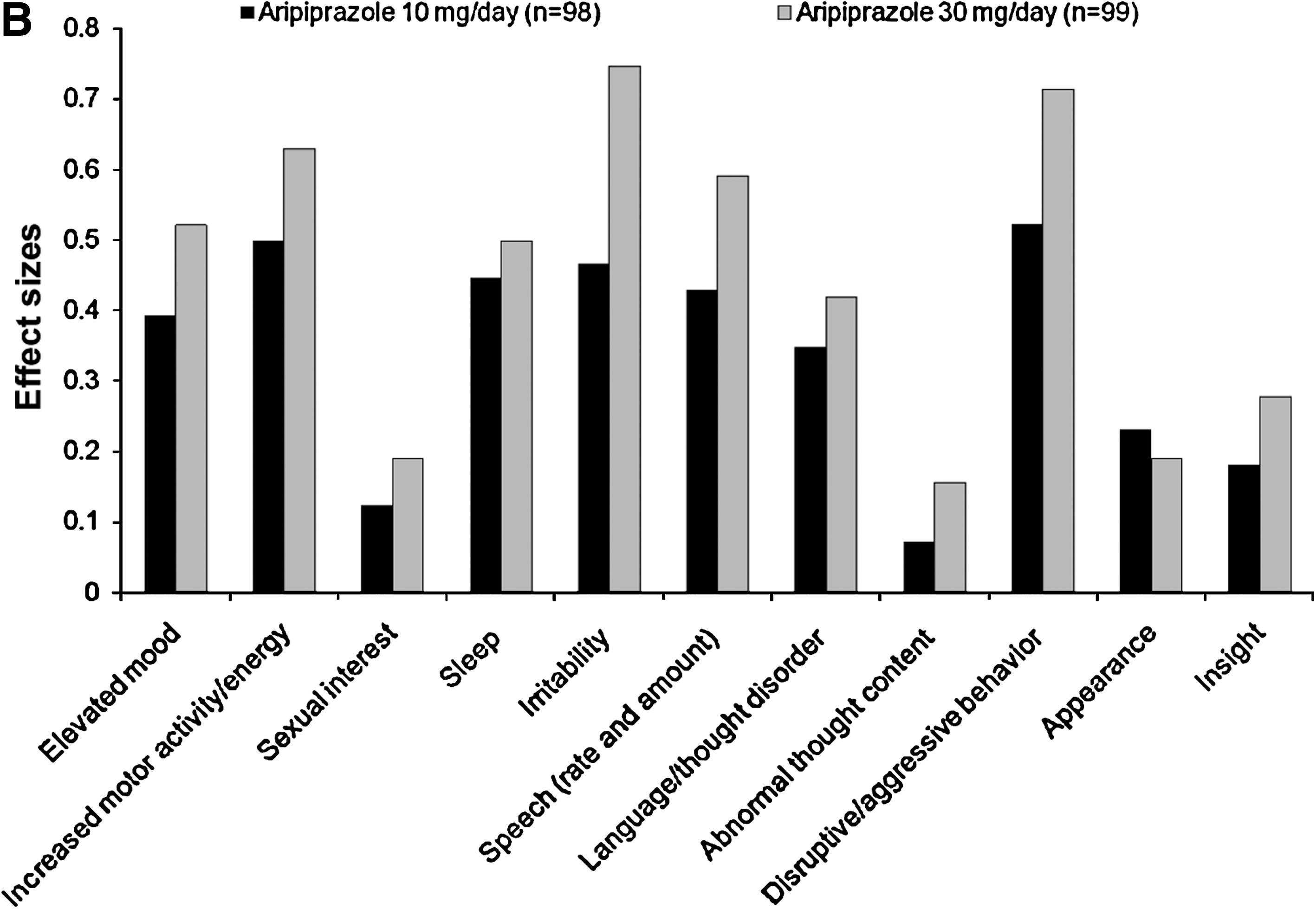
With the pooled aripiprazole dataset, significant improvements versus placebo were seen on the following individual YMRS line items at week 4: elevated mood (−1.5 vs. −0.9, p < 0.001), increased motor activity/energy (−1.6 vs. −0.7, p < 0.001), sleep (−1.2 vs. −0.7, p < 0.001), irritability (−2.4 vs. −0.9, p < 0.001), speech (−2.4 vs. −1.3, p < 0.001), language/thought disorder (−1.0 vs. −0.6, p < 0.001), content (−1.6 vs. −1.2, p < 0.05), and aggressive behavior (−2.3 vs. −0.9, p < 0.001). The three YMRS line items with the greatest effect size with the pooled aripiprazole group at week 4 were irritability (effect size = 0.7), aggressive behavior (effect size = 0.7), and increased motor activity/energy (effect size = 0.6). Nonsignificant improvements with the pooled aripiprazole group versus placebo on individual YMRS line items at week 4 were seen on sexual interest (−0.4 vs. −0.3, p = 0.105), appearance (−0.4 vs. −0.3, p = 0.182), and insight (−0.5 vs. −0.3, p = 0.067).
Safety results
A total of 204 individuals experienced TEAEs. Over the 4 weeks, the five most common TEAEs (>5% and more than twice the placebo rate) were (aripiprazole vs. placebo) somnolence (22.8% vs. 3.1%), extrapyramidal disorder (19.8% vs. 3.1%), fatigue (11.2% vs. 4.1%), nausea (10.7% vs. 4.1%), and akathisia (9.6% vs. 2.1%). A total of 16/294 (5.4%) subjects discontinued study medication because of a TEAE: 6/98 (6.1%) in the aripiprazole 10 mg/day arm, 8/99 (8.1%) in the aripiprazole 30 mg/day arm, and 2/97 (2.1%) in the placebo arm.
The most commonly reported TEAEs resulting in discontinuation of study medication (reported by more than one subject overall) were extrapyramidal disorder (aripiprazole 30 mg/day, n = 3), sedation (aripiprazole 10 mg/day, n = 2), fatigue (aripiprazole 10 mg/day, n = 2), and exacerbation of bipolar disorder (two subjects in the aripiprazole 30 mg/day arm).
Discussion
The purpose of this post hoc analysis was to evaluate systematically the effects of aripiprazole on individual YMRS line items in pediatric subjects with a manic or mixed episode associated with bipolar I disorder. Aripiprazole treatment resulted in statistically significant improvements in the majority of YMRS line items at week 4 and often sooner episodes. Symptoms of irritability, aggressive behavior, and increased motor activity/energy appeared to be the most responsive to treatment. Thus, aripiprazole may confer favorable outcomes for patients in whom these symptoms predominate. It has been proposed that severe irritability constitutes one of the cardinal symptoms of mania in children and adolescents, and irritability and aggressive behavior can be among the most worrisome and disruptive of symptoms for patients and caregivers. Improvements in other line items were of variable magnitude, and although there was only a trend toward improvement in insight, it is interesting to speculate whether this could be improved further with longer-term treatment, which would also include psychosocial therapies. Sustained improvements in insight are particularly important as these may be directly affecting adherence to therapy.
The findings in this pediatric cohort are consistent with those observed by Frye at al. in an adult population (Frye et al. 2008). Irritability and disruptive aggressiveness were most improved in terms of effect sizes in adults; this was seen across all subgroups: manic, mixed, those with psychosis, and those with rapid cycling (Frye et al. 2008). It is important to note, however, that psychiatric disorders in pediatric subjects may present with variable symptom profiles that are not always congruent with typical adult presentations.
Although other atypical antipsychotics have been previously shown to be effective in the treatment of pediatric subjects with bipolar I disorder, this analysis is of clinical interest because it specifically addresses the effects of specific individual mania symptoms as assessed by YMRS. It is also important, from a clinical standpoint, to understand the tolerability profile that may be expected with this treatment option; the safety and tolerability of aripiprazole in this patient population has been previously described (Findling et al. 2009). Briefly, it is worth noting that the most common TEAEs reported were somnolence, extrapyramidal disorder, and fatigue.
Limitations of this study include the fact that it was a post hoc analysis; because of the exploratory nature of the analysis, adjustments were not made for multiple comparisons. Further, the study duration was 4 weeks; more information from long-term data on specific symptom improvements is warranted.
In conclusion, pediatric subjects experiencing an acute manic or mixed episode associated with bipolar I disorder demonstrated an early, sustained, statistically significant improvement with aripiprazole compared with placebo. Aripiprazole improved a broad spectrum of symptoms across the YMRS scale, most notably irritability, aggressive behavior, and increased motor activity/energy.
Footnotes
Acknowledgments
Editorial support for the preparation of this manuscript was provided by Ogilvy Healthworld Medical Education. Funding for this study was provided by Bristol-Myers Squibb.
Disclosures
Raymond Mankoski is an employee of Bristol-Myers Squibb. Joan Zhao, William H. Carson, and Robert A. Forbes are employees of Otsuka Pharmaceutical Development & Commercialization, Inc. Suja Mathew is an employee of Otsuka America Pharmaceutical, Inc.