
Abstract
Objective:
Previous population-based studies have identified factors accounting for differential utilization of psychotropic medications among young patients with attention-deficit/hyperactivity disorders (ADHDs); yet, few analyses have addressed changes in such factors that can occur in the help-seeking process. The aim of this study was to examine patient- and service provider-level predictors for methylphenidate (MPH) initiation and discontinuation.
Method:
This cohort study included 10,153 newly diagnosed ADHD patients under 18 years of age in 2000, identified from the National Health Insurance Research Database. The risk association was estimated by time-dependent survival analyses, as indexed by hazard ratio.
Results:
Approximately 30% of young people received MPH treatment within the year of their ADHD diagnosis, and virtually none remained in treatment beyond 12 months. Regardless of co-morbidity status, the following were significantly associated with earlier initiation of MPH treatment: older age (e.g., adjusted hazard ratio [aHR] for age 12–17 = 4.5–7.6), lower socioeconomic status (aHR = 1.2–1.4), southern residence (aHR = 1.4–1.6), receiving the diagnosis while school was in session (aHR = 1.3–1.4), receiving the diagnosis from a physician specializing in pediatrics or psychiatry (aHR = 7.3–16.8), and receiving the diagnosis in a district hospital/clinic (aHR = 1.3–1.7). However, once treatment started, older ages appeared to increase the risk of early discontinuation by 15%, and the corresponding estimates for receiving initial MPH in a regional hospital or district hospital/clinic were 27% and 32%, respectively. Change in treatment location upon subsequent visit was associated with a 58% reduction in early discontinuation.
Conclusions:
This information about time-varying predictors for MPH utilization throughout treatment may provide insight into the delivery of pediatric mental health services and has important implications for the design of clinical treatment programs.
Introduction
Numerous randomized and observational studies have demonstrated the efficacy or safety of stimulant medications for ADHD in younger populations (Schachter et al. 2001; Bloch et al. 2009; Wigal 2009). In the case of immediate-release methylphenidate (MPH) treatment, a meta-analysis study found that the effect sizes on both hyperactivity-impulsivity and inattention fell between 0.5 and 1.5 (Faraone and Buitelaar 2010); the effect size has also been reported to be less salient in pre-school children (Greenhill et al. 2006). Also, although trend analyses suggest a rise in the utilization of stimulant medications in European and North American countries over the past two decades (Zito et al. 1999; Zuvekas et al. 2006; Trip et al. 2009; Zoega et al. 2009), gaps in diagnosis and treatment apparently remain. For example, a recent national survey on community-dwelling children in the United States found that roughly one-third to one-half of children with ADHD currently have had received no medication treatment (Froehlich et al. 2007; Visser et al. 2007). This observed gap may surface as a reflection of multifactor and intertwined processes, including differential accessibility to pharmacological or nonpharmacological therapy, concerns for adverse consequences or stigma, overdiagnosis, and insurance coverage (Winterstein et al. 2008; Brinkman et al. 2009).
To date, population-based evidence on factors associated with psychostimulant utilization in children and adolescents has generally relied on health surveys or medical claim data (Zito et al. 1999; Cox et al. 2003). In a study analyzing psychotropic experiences of ADHD-diagnosed children in the U.S. National Survey of Children's Health data, Visser et al. (2007) found that younger age, higher socioeconomic status, having health contact within 12 months, and having psychological difficulties were associated with medication utilization. Also, previous research has established that not only the need and utilization of pharmacotherapy but also the outcome may differ by co-morbid psychiatric condition in children diagnosed with ADHD (Boles et al. 2001; Radign et al. 2005; Chen et al. 2009); however, the results were inconsistent in terms of association patterns, probably because of variation in sample characteristics, definition for co-morbidity, or assessment time frame for co-morbidity condition (Jensen et al. 1997). In addition to individual sociodemographic background, co-morbidity, and medical history (e.g., cardiovascular disease) (Nissen 2006; Winterstein et al. 2007), the effects of service providers have also been implicated, such as physician specialty, insurance type, and level of medical institution (Zito et al. 1999; Lipkin et al. 2005; Marcus et al. 2005; Faber et al. 2006; Zuvekas et al. 2006; Gau et al. 2008).
Nevertheless, the majority of prior research on the utilization of psychotropic medications among young ADHD patients has centered on cross-sectional correlates (Zito et al. 1999; Radigan et al. 2005); the remaining has focused on the determinants of either treatment initiation or continuity (Winterstein et al. 2008; Chen et al. 2009; McCarthy et al. 2009; Olfson et al. 2009), and for medication continuity the findings are primarily associated with sociodemographic backgrounds (e.g., age) (Marcus et al. 2005). Few studies have been undertaken to examine factors associated with medication utilization longitudinally from initiation to discontinuation. Finally, although treatment seeking and compliance is a dynamic process, studies have often failed to take into account the time-varying effects of individual or service provider factors over the treatment process (e.g., patient's health condition and service-providing hospital). As a result, we have little information concerning whether the same array of factors may exert different effects on medication initiation and discontinuation or how changes in such factors taking place throughout the treatment process may influence young medication recipients' retention or even adherence.
The present study was designed to extend prior findings by identifying a group of more than 10,000 young people who recently received the diagnosis of ADHD. Through the pharmacy and medical claim data from the National Health Insurance Research Database (NHIRD), we retrieved 5-year records for these young patients across a wide variety of health conditions and healthcare utilizations. By introducing into an analytic framework the time-varying individual clinical conditions and the service providers experienced throughout the treatment-seeking process, this exploratory study sought to examine the extent to which individual and service providers may be differentially associated with (i) the initiation of MPH treatment following initial diagnosis of ADHD and (ii) discontinuation within the year of treatment in children and adolescents. A better understanding of similarities and differences in the factors associated with “initiation” and “treatment retention” would be helpful both for clinical practice in treatment of young individuals with ADHD and for health educational efforts delivered at family or school.
Methods
Data source
The data for the present study are from the 1997 to 2002 NHIRD, a database obtained from the National Health Insurance Program (NHIP), which has provided universal health coverage (i.e., curative care, dental service, preventive medicine, and prescription drugs) to eligible residents in Taiwan since 1995. The NHIP coverage rate for those younger than 19 years old was estimated as 98.7% in 2004 (Chen et al. 2007). The NHIRD is currently managed by the National Health Research Institutes (NHRI). For each insured a unique encrypted identification number has been created to link different data files, including the registry for beneficiaries (e.g., gender), registry for contracted medical facilities (e.g., level of medical institution), registry for drug prescriptions, ambulatory care expenditures by visit (e.g., diagnosis of ADHD, cardiovascular disorders), and details of ambulatory care orders (e.g., MPH and psychiatric medications by visit). All information pertaining to identifiers (e.g., personal identification number, hospital name, or any other variables that can be linked to individual subject or hospital) was encrypted, thus removing the need for patient informed consent. Approval of this study was granted by NHRI's institutional review board (EC0990804-E).
Measures
Records of ambulatory healthcare (mainly outpatient services) were used to retrieve newly diagnosed cases of ADHD. For the purpose of this analysis, we have identified a total of 10,153 individuals who (i) were 17 years old or younger; (ii) had received a diagnosis of ADHD in the calendar year of 2000; and (iii) had received no diagnosis of ADHD in preceding 3 years (i.e., 1997–1999). ADHD was defined by 314.XX codes in the International Classification Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). In the NHIP, for each visit in ambulatory service (i.e., outpatient care), reimbursement was made on the basis of no more than three diagnoses. If an individual had been diagnosed with a developmental disorder other than 314 prior to the diagnosis of ADHD, then he or she may be considered a co-morbid ADHD case in the present study. In clinical practice, the majority of the diagnoses and corresponding ICD codes were written and keyed-in in the medical charts and hospital health records, which later became the information basis for applying health insurance reimbursement.
Individual characteristics
For each young subject with newly diagnosed ADHD, the information pertaining to individual sociodemographic characteristics (i.e., gender, age, enrollee's category [EC], region, and urbanicity), prior history of medical condition, healthcare providers (i.e., medical institutions and specialty), and pharmacological treatment were subsequently retrieved. For sociodemographic background, we used EC as a proxy measure for socioeconomic status, defined by the job type of the enrollee or, more often, of the parents of the young insured. In general, EC I comprised employment in the government, government-run businesses, and public educational institutions, whereas EC II comprised mainly private enterprises; EC III comprised agriculture, fishing, mining, and private educational institutions; and EC IV the military and work that brought in less than the minimum wage. Compared with the enrollees from EC I and II, those from EC III or IV are more likely to be of lower socioeconomic status. We also divided parents or primary caregivers of enrollees' employment locations into four regions: northern, central, southern, and eastern. Utilizing an urbanization index comprising five factors—population density, the percentage of residents with higher education, the percentage of residents >65 years old, the percentage of residents involved in agriculture, and the quality of health-service resources—the young insured were regrouped into three categories: urban, suburban, and rural areas. In this study, both region and urbanicity were adopted as proxy measures to reflect differential accessibility toward mental health services in Taiwan. An individual's prior diagnoses of other psychiatric disorders was defined by ICD-9-CM (codes 290–313, 315–319) on the basis of outpatient care records from January 1, 1997, through the day before ADHD diagnosis. Similarly, from outpatient and inpatient healthcare records from January 1, 1997 onward, ICD-9-CM codes 390–448 and 746 were adopted to retrieve prior history of cardiovascular disorders (e.g., acute rheumatic fever and congenital heart disease).
Service provider characteristics
As to the attributes of healthcare providers, medical institutions where the young insured received their first diagnosis of ADHD were categorized into three groups: medical centers, regional hospitals, and local hospitals/clinics. The same grouping rules were applied to classify the medical institutions that prescribed the index MPH treatment. For physicians (i) who made the first diagnosis of ADHD or (ii) who initiated MPH treatment, their specialties were categorized into pediatrics, psychiatry, and other (e.g., rehabilitation). In the present study, a second doctor visit was defined when the young ADHD case had a visit to a doctor who was different from the one who gave the initial diagnosis; similarly, “change in treatment location” in subsequent visit was indicated if the young ADHD cases started to receive an MPH prescription in a hospital/clinic different from the one that initiated treatment.
MPH treatment characteristics
Information pertaining to MPH treatment was obtained from the outpatient healthcare records. The event of initiation was defined if one has started receiving MPH prescription following the initial ADHD diagnosis; for discontinuation, the event was defined if there was a gap of 90 days or more in MPH treatment. Four categories of psychiatric medications commonly involved in concomitant use with MPH to treat ADHD in Taiwan included the following: (i) tricyclics (imipramine, desipramine, nortriptyline, and amitriptyline), (ii) cyclic antidepressants (bupropion and fluoxetine), (iii) alpha 2 agonist (clonidine and guanfacine), and (iv) antipsychotics (risperidone, thioridazine, and chlorpromazine). As to the variable concerning timing of diagnosis, “school recess” would be coded if the first ADHD diagnosis was made during the school vacation periods (i.e., February 2–22 or July 1 through August 31 in the 2000 calendar year) and coded as “school days” if the diagnosis was made in the rest of 2000 (i.e., while school was in session). After the MPH treatment was started, those young people who had transited from kindergarten to elementary school, from elementary to middle school, or from middle to high school would be considered to have positive experience for school transition.
Analysis
All the data preparation and analyses were performed using SAS 9.1 software (SAS Institute, Inc., Cary, NC). Considering that patients' help-seeking or physicians' prescription dispensing for ADHD may be different by one's prior history of other mental disorders, we first summarized the distribution of individual sociodemographic background and medical history, service provider characteristics, and MPH utilization among newly diagnosed ADHD cases with stratification by prior co-morbidity. Next, we plotted smoothed estimates for cumulative hazard rates of MPH treatment on a monthly basis, from the day after diagnosis to 1 year later; the log-rank test was adopted to test possible hazard variation existing between subgroups defined by prior history of other psychiatric disorders via Proc LIFETEST. Finally, to investigate individual and service provider factors accounting for (i) the initiation of MPH treatment with the year of ADHD diagnosis and (ii) the discontinuation during the first year after initiation of pharmacological treatment, we turned to time-dependent survival analyses. Time to MPH treatment initiation was calculated since the date of initiation of ADHD diagnosis; discontinuation of MPH treatment was considered if the ADHD cases did not receive MPH prescriptions for 90 days or more in two consecutive refills, with the elapsed time calculated since the expiration date of the last prescription. Cox's proportional hazard models, via Proc PHREG procedures in SAS, were carried out first to obtain crude hazard ratios (cHRs), followed by statistical adjustment with time-dependent covariates (e.g., age, prior history of cardiovascular diseases, second-opinion seeking, a change in the treatment location, and concomitant utilization of psychiatric medications) and time-invariant covariates (e.g., gender, medical institutes and specialty for initial diagnosis) in order to estimate adjusted HRs (aHRs) and 95% confidence intervals (CIs).
Results
Among children and adolescents who received initial diagnosis of ADHD in 2000, an estimated 28% (n = 2,838) had a history of other mental disorders, among which more than 35% had developmental delay or disorders (ICD = 315) and 8% had autism. With stratification by co-morbid mental disorders, characteristics of 10,153 newly diagnosed ADHD cases are summarized in Table 1. Roughly three-quarters were male; half received their diagnoses from medical centers and more than half were diagnosed by specialists in psychiatry. An estimated 4% of those with prior mental disorders had cardiovascular diseases, significantly higher than the 2.3% for those without prior mental disorders. In general, the young ADHD cases with other mental disorders were more likely to receive their diagnoses before elementary school (age <6 years) or at regional hospitals and start MPH treatment sooner, compared with their counterparts.
p < 0.001.
The columns do not add up to 100% because of missing data.
Chi-square test.
Defined by the 1997–1999 outpatient service records.
ICD-9-CM code is 390–448 and 746 in outpatient and inpatient healthcare records from January 1, 1997, until the day before receiving initial ADHD diagnosis.
ADHD = attention-deficit/hyperactivity disorder; MPH = methylphenidate.
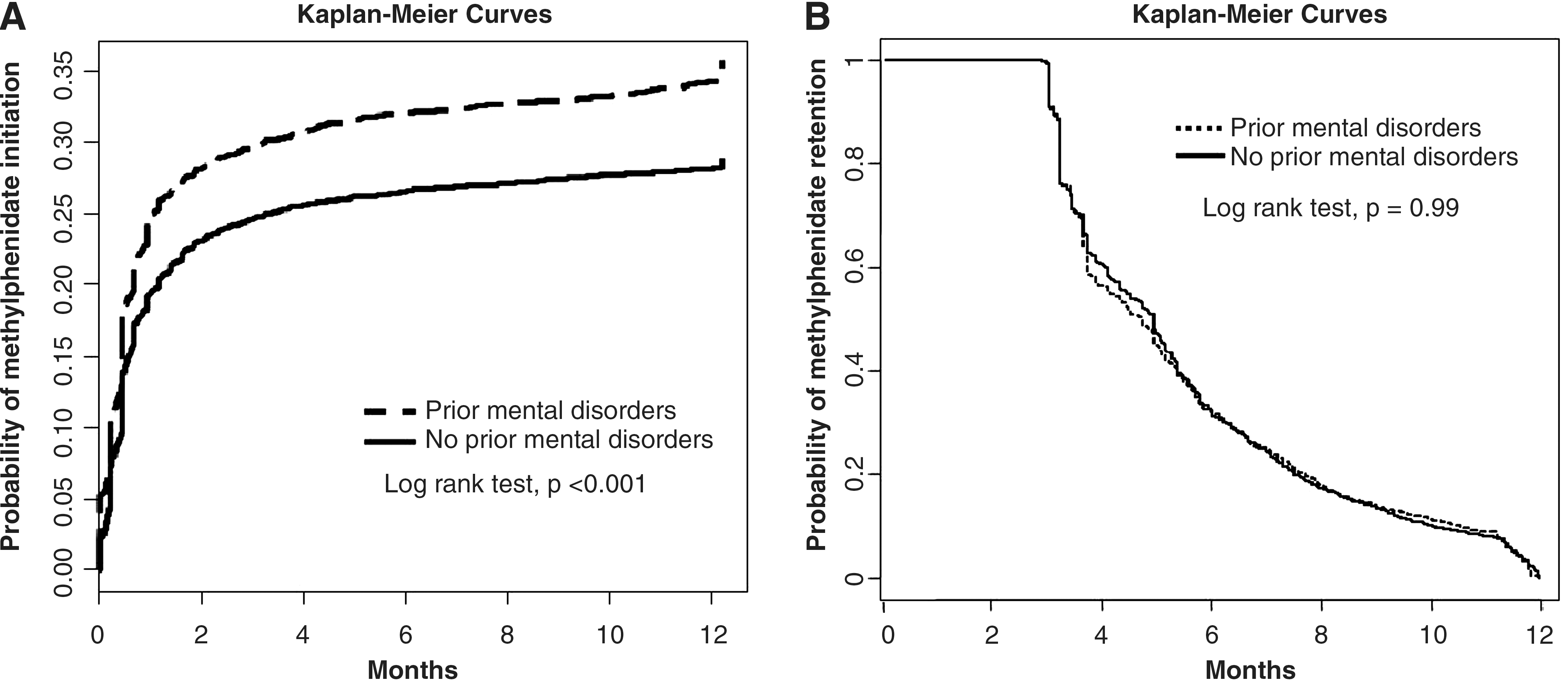
Within the first month of receiving ADHD diagnosis, roughly 25% of ADHD cases with a prior history of mental disorder initiated MPH treatment; the corresponding estimate among those without such a history was estimated as 18% (Fig. 1, Panel A). After 11 months, the proportion of MPH utilization gradually reached 36% among those with prior mental disorders, significantly greater than those without (28%, p < 0.001). In addition, the test of proportionality assumption indicates a violation (p < 0.001), suggesting that the differences associated with prior history of mental disorders in the hazard of MPH initiation appear time-varying. On the other hand, among those who started MPH treatment, approximately 65% discontinued within 6 months and less than 10% remained by the end of the first year. No differences were found between MPH treatment retention and prior history of mental disorder (log-rank test, p = 0.71) (Fig. 1, Panel B).
With stratification by prior history of mental disorders, Table 2 shows the estimated hazard ratio (HR) linking individual and service provider characteristics with receiving MPH treatment within the year of ADHD diagnosis, and the aHR estimates were obtained with simultaneous adjustment for all listed variables. Among the newly diagnosed ADHD cases without prior mental disorders, those who are male, in lower socioeconomic status, had older ages, received the diagnosis during school days, at a district hospital/clinic, from specialties of pediatrics or psychiatry, or had a second doctoral visit were more likely to initiate their MPH treatment. A second doctor visit was associated with a 38% increased hazard of receipt of MPH treatment (aHR = 1.38; 95% CI: 1.24–1.52). For co-morbid ADHD, the increased risks appeared significant only for time-invariable variables, including older ages, lower socioeconomic status, southern region residence, and receiving the diagnosis during school days, at a district hospital/clinic, or from specialties of pediatrics or psychiatry.
p < 0.05.
p < 0.01.
p < 0.001.
Time-varying variables.
Obtained via Cox's proportional hazard rate model.
Adjusted for all listed variables.
ICD-9-CM codes 390–448 and 746 in outpatient and inpatient healthcare records from January 1, 1997, until the day before (i) receiving the first prescription of MPH or (ii) the 365th day after ADHD diagnosis.
CI = confidence interval; ADHD = attention-deficit/hyperactivity disorder.
We found that, consistent with the results shown in Panel B of Figure 1, the history of mental disorder was not significantly associated with the discontinuation of treatment (aHR = 0.95, 95% CI: 0.86–1.05) (Table 3). An estimated 93.2% of children and young people discontinued MPH prescription within a year (n = 2,870), and overall, after adjusting for all listed variables, the analyses suggest that the discontinuation of MPH treatment was more related to service providers' attributes than to individual sociodemographics. ADHD cases who received their initial MPH from district hospitals or clinics were 1.32 times more likely to discontinue prescription (95% CI: 1.17–1.49), and a change in hospital/clinic was associated with a subsequent 58% reduced risk of treatment discontinuation. Other time-varying variables—including school transition, the diagnosis of cardiovascular disease, and concomitant use of other psychotropic medications—were found to have little effect on the discontinuation of MPH treatment.
p < 0.05.
p < 0.01.
p < 0.001.
Time-varying variables, covering the period from the first prescription through the day before (i) the 366th day (1 year) since the first MPH prescription or (ii) the discontinuation of MPH prescription.
Obtained via Cox's proportional hazard rate model with adjustment for all the listed variables.
ICD-9-CM codes cover 390–448 and 746 in outpatient and inpatient healthcare records from January 1, 1997, through the day before (i) the 366th day (1 year) since the first MPH prescription or (ii) the discontinuation of MPH prescription.
Discussion
In the context of a national single-payer healthcare system, the present study found that approximately 30% of children or adolescents received MPH treatment within the year of their ADHD diagnosis. Regardless of psychiatric co-morbidity, young patients who were from lower socioeconomic status (e.g., enrollment status III) or the southern region and received the diagnosis at older ages, during school days, in a community hospital/clinic, or by specialists in pediatrics or psychiatry tended to start MPH treatment sooner. In the non–co-morbid ADHD, male gender and the change in doctor at subsequent visits were found to be associated with increased hazards to start MPH medication by 36% and 38%, respectively. The retention rates for MPH treatment declined after 3 months, and only one-third of the youth remained in treatment by the end of the 6th month. Both older ages and having initial MPH prescription from the hospitals other than medical centers were associated with greater hazards of discontinuation; having changed the treatment location at subsequent visit may increase treatment retention.
Recent analyses of MPH treatment continuity in pediatric populations consistently support that patients with older ages tend to have shorter treatment duration or greater likelihood of premature discontinuation (Marcus et al. 2005; McCarthy et al. 2009). Our data extend prior findings by demonstrating that older ages were associated with a higher hazard of MPH discontinuation, even though older ages were also associated with earlier engagement in MPH treatment. The somehow contradictory association estimates suggest that ages (or developmental stage) may have different effects in determining medication utilization in pediatric populations. These effects may be explained by factors such as age (or development)-related differences in clinical manifestation of ADHD, willingness to adhere to medication regimens, side effects, parental engagement, and social expectation toward role performance (Biederman and Spencer 2008; Gau et al. 2008). Given that most ADHD symptoms may persist into adulthood, further longitudinal studies would be appropriate to examine health or developmental outcomes in those who received their initial ADHD diagnosis in adolescence and to understand potential reasons to prematurely discontinue treatment.
Our findings challenge the current controversial views, based on cross-sectionally statistical adjustment approach, about co-morbidity in medication utilization patterns among ADHD-affected children (Boles et al. 2001; Radigan et al. 2005; Chen et al. 2009; Faber et al. 2010). Specifically, following a group of newly diagnosed ADHD children for 1–2 years, we found that the role of co-morbidity was not uniform throughout the treatment process; the predictor profile for MPH initiation appears dissimilar across two groups defined by prior history of mental disorders. Although the exact reason for these observed differences is unclear, there are several potential explanations. First, prior co-morbid psychological condition may affect physicians' choices to prescribe MPH; similarly, it is very likely that children's prior experience or response toward medication treatments may affect family's or children's willingness to initiate MPH treatment. Another explanation is that patients with a prior diagnosis of mental disorders may have different medical help-seeking processes from those without. The differences may partly explain why the factor “second doctor visit” was significant only for MPH initiation in ADHD-only children (aHR = 1.38), reflecting that parents or primary caregivers may seek second opinions to determine whether the ADHD child should receive stimulant treatment. Our findings may reinforce the importance of education about ADHD to parents or children upon the first suggestion of diagnosis and subsequent referrals (particularly those having limited experience with mental health professionals). Of particular interest for improving prescription utilization among ADHD children is comparing the MPH adherence and clinical outcomes between those who sought second opinions and those who did not (Faber et al. 2006; Thompson et al. 2009).
Although the results of most previous studies indicate the influence of service providers in determining stimulant medication utilization among ADHD children (Zito et al. 1999; Faber et al. 2006; Gau et al. 2008; Chen et al. 2009), the evidence was limited in terms of temporality or possible time-varying effects. For MPH treatment initiation, the observed medical institution variation in hazards may partly be the result of complex processes involving help-seeking process (e.g., patients were referred to medical centers by regional hospitals) and medication prescribing behaviors regulated by insurance policies. The longitudinal analyses suggest that receiving the ADHD diagnosis from a district hospital/clinic may increase children's engagement in MPH treatment; however, having an index prescription from a district hospital/clinic was associated with early discontinuation of treatment. Further, having the change in the prescribing hospital/clinic was associated with a 58% reduction in early MPH discontinuation. Possible explanations for our findings might be the level of medical institution-related differentials in clinical evaluation prior to stimulant prescription, titration process at initial treatment, and subsequent monitoring and follow-up procedures. Further, the observed lower likelihood of early discontinuation associated with medical center prescribing index MPH and change in prescribing hospitals/clinics may possibly indicate that ADHD cases may change their service providers to more specialized mental healthcare.
Some diagnosis-timing differences were found in relation to MPH treatment initiation. These differences were to be expected, given that the potential short-term benefit (e.g., improvements in school adjustment and academic performance) may increase parents' or primary caregivers' willingness to pursue stimulant treatment (Biederman and Spencer 2008; Scheffler et al. 2009). Despite clinical concerns of an association between cardiovascular risk and stimulant medication (Nissen 2006), we did not find an association between one's history of cardiovascular diseases and MPH initiation as well as discontinuation. This observation may be, partly, due to the small number of children with cardiovascular diseases (<5%) in our sample.
To our knowledge, this population-based study is the first report to longitudinally examine an array of individual, clinical, and service provider attributes affecting both the initiation and discontinuation of MPH treatment in children and adolescents newly diagnosed with ADHDs. The large sample size of ADHD children identified through the data of a single-payer healthcare system allows us to probe this important pediatric mental health issue with national representativeness that may limit selection bias or generalizability problems associated with insurance-specific enrollment criteria (e.g., low income in the U.S. Medicaid system). Our study also appears to be one of just a few to evaluate determinants associated with medication utilization while taking time-varying nature into account. This approach grants us the ability to capture what happened after the initiation of MPH and to evaluate faithfully the de facto effects of clinical and service providers over the course of treatment.
Some potential limitations of this study should be considered before more detailed discussion. One noteworthy limitation is that all the information was solely derived from the source of medical utilization (i.e., the NHIP data). The medical claim data limited the scope of the present study and restrained our ability to control for other important factors that may exert their influences differentially throughout pharmacological treatment. For example, preliminary evidence suggests that the presence of hyperactivity symptoms appear strongly associated with ADHD medication utilization (Chen et al. 2009), yet insignificant for continuity of treatment (Olfson et al. 2009). The lack of information concerning detailed clinical manifestation of ADHDs (e.g., severity or clinical profiles) limits this study's ability to further probe subtype variation in MPH utilization among children with newly diagnosed ADHD; a relevant issue is that we were unable to provide direct evidence with respect to clinical validity for ADHD diagnosis. Also, possible gaps might occur between dispensing prescription and treatment adherence. A recent survey on immediate-release MPH utilization in children found that factors such as later onset age, higher frequency of daily MPH administration, and nonmedical centers are associated with increased odds of poor adherence. It is possible that the aforementioned factors may indirectly operate on early discontinuation of MPH treatment through poor adherence or clinical outcome. In addition, as the immediate release formulation was the only form dispensed for the young ADHD cases in the National Health Insurance Plan from 2000 to the end of 2003, we were not allowed to assess the effects of dose, acting period, or prescription shift on the discontinuation of MPH treatment. Finally, our findings represent MPH utilization patterns of children with newly diagnosed ADHD in Taiwan. Although the discontinuation rate resembles those of other countries, generalizing the observed associations would be problematic, especially to the populations with different healthcare systems or different health insurance plans.
Conclusions
Findings from our study support the notion that the initiation and continuation of MPH treatment in children and adolescents were differentially affected not only by individual background, but also by service provider characteristics. Youngsters with ADHD may benefit from the development of mental healthcare services that address socioeconomical- or geographical-related differences in accessibility and from the delivery of pharmacological treatment tailored to individual developmental contexts (e.g., age, school cycle, or co-morbidity). A full investigation of the compliance and outcomes on ADHD children receiving treatment at different levels of hospital/clinics is worthy of future research.
Clinical Significance
This information about time-varying effects of individual and service provider factors on MPH utilization throughout treatment process may provide insight into the delivery of pediatric mental health services and has important implications for the design of clinical treatment programs. Clinically, the delivery of pharmacological treatment for ADHD in younger population should be initiated with close follow-up and assured continuity with regular monitoring. In addition, to reduce early dropout and to ensure service continuity, treatment plans are suggested to integrate local community resources (e.g., schools or clinics).
Footnotes
Acknowledgments
The authors thank those who manage the NHIRD in NHRI's Department of Research Resources. Dr. C.-Y. Chen has received grant funding for this study from the NHRI: NHRI 98A1-PHPP44-021.
Disclaimer
NHRI had no role in the study design; in the collection, analysis, or interpretation of data; in the writing of the report; or in the decision to submit the article for publication.
Disclosures
Dr. K.-M. Lin has received research grant support from Lundbeck and a fellowship at the Center for Advanced Study in the Behavioral Sciences at Stanford University (CASBS), 2008–2009. Ms. H.-H. Yeh, Mr. K.-H. Chen, Dr. I.-S. Chang, and Dr. E.C.-H. Wu have no financial relationships to disclose.
Funding/support: This work was supported by a grant from the National Health Research Institutes (98A1-PHPP44-021) to Dr. Chuan-Yu Chen.