
Abstract

To the Editor
Case Report
A 28-month-old, previously healthy girl of 13 kg was brought to the hospital emergency department because of decreased consciousness for 30 minutes. The girl was found playing with her father's medication 6 hours earlier, and hence, there was a suspicion of drug-induced toxicity. According to the parents, three 10 mg tablets of olanzapine were potentially missing.
On admission, the girl was sleeping with a snoring breath and did not open her eyes after stimuli. Her vital signs were oxygen saturation 98%, respiratory rate 23 breaths/min, temperature 37.8°C, and pulse 130 beats/min. She showed tachycardia in combination with hypertension, but later she became hypotensive. She had constricted pupils with normal light reflexes, and apart from low symmetric reflexes, neurological exam revealed no further abnormalities. No gastric lavage with decontamination with activated charcoal was performed, as the moment of intake was probably more than 6 hours earlier. Clinical laboratory analysis demonstrated no abnormalities.
The girl was admitted to a pediatric intensive care unit (PICU) for monitoring of her vital signs, because she was still unconscious. During the subsequent hours, she remained unconscious. However, intubation was not indicated. She received nasal oxygen and a single bolus of intravenous normal saline (20 mL/kg) upon which tachycardia normalized. Six hours after admission to the PICU, she spontaneously opened her eyes. However, she was agitated and tearful and talked with slurred speech. Meanwhile, intoxication with olanzapine was confirmed by a measured serum olanzapine level of 888 ng/mL (therapeutic level: 5–75 ng/mL). Because of the reported long elimination half life of olanzapine (37.2 hours in pediatric patients) (Grothe et al. 2000), the girl was discharged from the PICU to the general pediatric department for further observation. Initially, her movements were still uncoordinated; later on this improved, and she was able to walk. After 36 hours, she had fully recovered and was alert. She was also able and willing to eat and diuresis began. Finally, 42 hours after the presentation, she was discharged.
Additional olanzapine serum levels, analyzed by liquid chromatography coupled with tandem mass spectrometry (Department of Clinical Pharmacology and Pharmacy, VU University Medical Center, Amsterdam, The Netherlands), were measured after the patient was discharged (Fig. 1). Serum levels at 30 and 42 hours after probable ingestion were 197 and 106 ng/mL, respectively. The calculated half life was 11.6 hours.
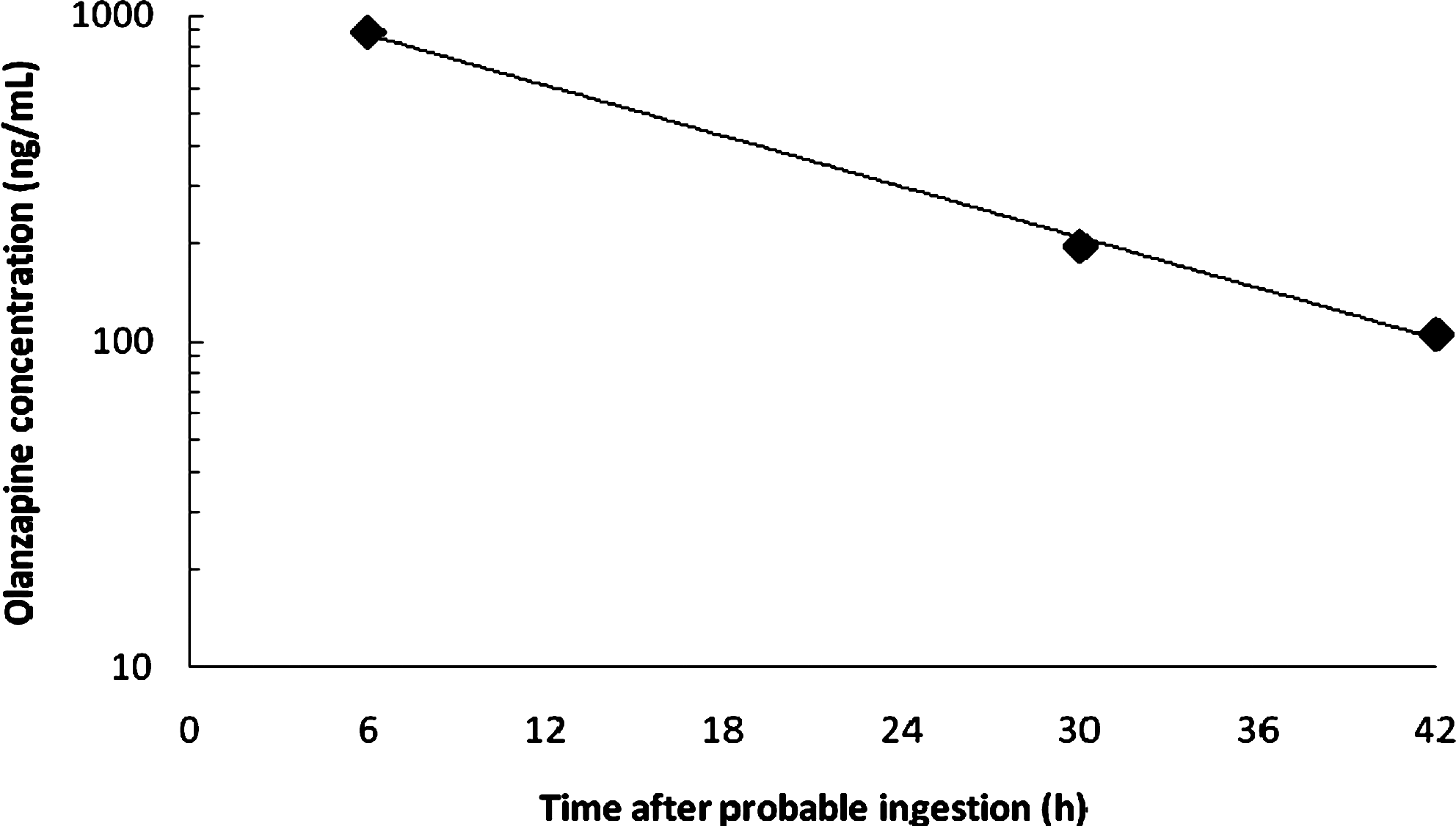
Olanzapine serum concentrations after an unintentional overdose.
Discussion
Here we describe an olanzapine intoxication in a 2-year-old girl with a very high olanzapine serum level of 888 ng/mL. During therapeutic olanzapine use, serum levels between 5 and 75 ng/mL are considered therapeutic (Robertson and McMullin 2000). Severe toxicity may occur at serum levels as low as 100 ng/mL and deaths due to olanzapine toxicity have been observed even at levels below 500 ng/mL (Robertson and McMullin 2000).
Only a few cases of pediatric overdoses of olanzapine have been reported thus far (Dougherty et al. 1997; Chambers et al. 1998; Yip et al. 1998; Bond and Thompson 1999; Bonin and Burkhart 1999; Catalano et al. 1999; Litovitz et al. 1999; Jacobs et al. 2001; Kochhar et al. 2002; Etienne et al. 2004; Palenzona et al. 2004; Watson et al. 2004; Theisen et al. 2005; Powell et al. 2010). Most of these cases concerned suicide attempts in adolescents. The highest olanzapine level reported after an overdose in a pediatric case is 1,503 ng/mL in a 14-year-old girl (Theisen et al. 2005). In younger children the highest reported olanzapine level is 340 ng/mL in a 1-year-old boy (Bonin and Burkhart 1999). In both cases the eventual clinical implications were relatively mild, but the initial symptoms were serious (Bonin and Burkhart 1999; Theisen et al. 2005).
The predominant clinical symptoms in our case were loss of consciousness, with later on slurred speech and agitation, similar to those reported in other cases (Chambers et al. 1998; Yip et al. 1998; Bond and Thompson 1999; Catalano et al. 1999; Jacobs et al. 2001; Kochhar et al. 2002; Theisen et al. 2005). These can be explained by the receptor binding profile of olanzapine: Central nervous system depression due to histamine H1-receptor blockade; anticholinergic effects, for example, agitation due to muscarine M1-receptor blockade; dyskinesia, for example, slurred speech due to dopamine D2-receptor blockade (Theisen et al. 2005). Symptoms of intoxication emerged at 6 hours after the probable moment of ingestion of olanzapine and did therefore correlate with the peak plasma level. Together with a rapid decline in olanzapine serum levels, the symptoms improved within 24 hours and the clinical situation normalized within 36 hours. Thus, eventually the clinical course of the intoxication was mild. This is in concordance with most of the previously published pediatric case reports in which the patients recovered within 48 hours after ingestion of olanzapine (Dougherty et al. 1997; Yip et al. 1998; Bonin and Burkhart 1999; Catalano et al. 1999; Jacobs et al. 2001; Kochhar et al. 2002; Palenzona et al. 2004; Theisen et al. 2005).
The peak serum olanzapine level in our case was 888 ng/mL at probably 6 hours after ingestion. The following measured serum levels after 30 and 42 hours (197 and 106 ng/mL) were still within the toxic range. Olanzapine levels as high as 888 ng/mL have not been reported before in a toddler.
Olanzapine shows linear kinetics over the clinical dosing range (Callaghan et al. 1999; Theisen et al. 2005). This was also observed in the measured time window of our case (Fig. 1). However, the elimination half life (t ½) of 11.6 hours calculated in our case is much shorter than the reported half life of 37.2 hours (coefficient of variation (CV%) = 13.8) in children and adolescents treated with olanzapine (Grothe et al. 2000). A possible explanation for this discrepancy is extensive redistribution of the drug throughout the body with a large volume of distribution (10–22 L/kg), which may contribute to the rapid decline of serum levels (Callaghan et al. 1999; Theisen et al. 2005). Moreover, distribution pharmacokinetics of olanzapine are reported after large overdoses, in which a phase with an initial half life of 24 hours during the first 3 days after ingestion was followed by a phase with a half life of about 60 hours (Lennestal et al. 2007). As in our case only serum levels until <40 hours after ingestion were available, this observation cannot be substantiated.
Given the high peak serum level of 888 ng/mL and a reported volume of distribution of 10–20 L/kg (130–260 L) (Grothe et al. 2000), it can be deduced that the girl has ingested around 115–230 mg of olanzapine. This amount is much higher than the reported ingestion of 30 mg of olanzapine. On the other hand, assuming that the amount of ingestion actually was around 30 mg, then the apparent volume of distribution would be around 34 L (2.6 L/kg). Such a large deviation in the apparent volume of distribution could also be a possible explanation for the very short elimination half life observed in our case.
Conclusion
Despite a very high olanzapine serum level, the severity of symptoms was limited to decreased level of consciousness, and recovery was seen within 36 hours. Remarkably, the elimination half life of olanzapine in this case was much shorter than the reported half life in children (11.6 vs. 37.2 hours) (Grothe et al. 2000). This may imply that the pharmacokinetics of olanzapine after an overdose differ from the kinetics in the clinical dosing range.
Disclosures
None of the authors has any relationship with commercial entities that may have a direct bearing on the relevant subject matter. Drs. Lankheet, Padberg, Kluiver, Wilhelm, van Woensel, Beijnen, and Huitema have no conflicts of interest or financial ties to disclose.