
Abstract
Objective:
The diagnosis and treatment of youth with severe nonepisodic irritability and hyperarousal, a syndrome defined as severe mood dysregulation (SMD), has been the focus of increasing concern and debate among clinicians and researchers. Our main objective was to assess the effectiveness of risperidone for youths with SMD.
Methods:
An 8-week open label trial with risperidone was conducted. We extensively assessed 97 subjects with semistructured and clinical interviews and enrolled 21 patients in the study. Risperidone was titrated from 0.5 to 3 mg/day in the first 2 weeks. Evaluations were performed at baseline and weeks 2, 4, 6, and 8. Clinical outcome measures were (1) Aberrant Behavior Checklist–Irritability Subscale, (2) Clinical Global Impressions, and (3) severity of co-morbid conditions.
Results:
We found a significant reduction of the Aberrant Behavior Checklist–Irritability scores during the trial after risperidone use (p < 0.001). The scores at week 2 (mean = 12.03; standard error [SE] = 2.94), week 4 (mean = 15.48; SE = 2.93), week 6 (mean = 12.29; SE = 2.86), and week 8 (mean = 11.28; SE = 3.06) were significantly reduced compared with the baseline mean score (mean = 25.89; SE = 2.76) (p < 0.001). We also found an improvement in attention-deficit/hyperactivity disorder, depression, and global functioning (p < 0.001).
Conclusion:
Risperidone was effective in reducing irritability in SMD youth. To the best of our knowledge, this is the first psychopharmacological trial in this group of patients with positive results. Further randomized, controlled studies are needed.
Introduction
Until recently, controversy surrounded the role of irritability in the diagnosis of pediatric bipolar disorder (BD) (Birmaher et al. 2006; Carlson and Meyer 2006; Blader and Carlson 2007). However, longitudinal studies helped to clarify this issue, showing that episodic irritability is correlated with mania, family history of bipolar disorder, and suicide attempts, whereas patients with chronic irritability show a trend to depressive and anxious disorders in adulthood (Bhangoo et al. 2003; Brotman et al. 2006; Stringaris et al. 2009).
To standardize diagnostic criteria for pediatric BD, Leibenluft et al. (2003b) proposed a classification according to four clinical phenotypes. The (1) narrow phenotype is exhibited by patients who meet full Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatry Association 1994), criteria for mania or hypomania, including the duration, the episodicity, and hallmark symptoms of elevated mood or grandiosity. The intermediate phenotypes include (2) mania not otherwise specified, in which patients have clear episodes and hallmark symptoms but the episodes last between 1 and 3 days, or (3) irritable mania, in which patients have demarcated episodes with irritability but not elevated mood. Finally, the (4) broad phenotype is exhibited by patients who have a chronic, nonepisodic illness that does not include elevated mood or grandiosity but rather severe and chronic irritability and hyperarousal. The authors proposed the denomination severe mood dysregulation (SMD) for this broad phenotype and characterized the condition as featuring an abnormal baseline mood (i.e., irritability, anger, and/or sadness, noticeable to others and present most of the time) (Leibenluft et al. 2003b). In addition, SMD involves hyperarousal (i.e., at least three of the following: insomnia, physical restlessness, distractibility, racing thoughts or flight of ideas, pressured speech, intrusiveness) and increased reactivity to negative emotional stimuli (e.g., temper outbursts) at least three times per week. Although some investigators still consider SMD as a developmental presentation of bipolar disorder in children, several different research lines suggest that it has different demographic characteristics, co-morbidities (Dickstein et al. 2005), familial diagnoses (Brotman et al. 2007), neuropsychological patterns (Dickstein et al. 2007; Rich et al. 2007; Rau et al. 2008; Brotman et al. 2010; Rich et al. 2010), and longitudinal outcomes (Brotman et al. 2006; Stringaris et al. 2009, 2010).
Although the clinical characterization of SMD has attracted significant attention, treatment strategies have been poorly studied. A double-blind randomized study using lithium was carried out, but the drug failed to show benefit in reducing irritability, mood dysregulation, and temper outbursts (Dickstein et al. 2009). Some other therapeutic efforts have been made in the last years concerning management of aggressive children. Stimulants alone (Galanter et al. 2003) or in conjunction with behavior therapy (Waxmonsky et al. 2008) proved effective in patients with the association of ADHD and maniac symptoms. In a recent trial, Blader et al. (2009) showed that the addition of divalproex to the psychopharmacological treatment of ADHD patients whose chronic aggression was underresponsive to a stimulant trial increased the likelihood of remission. However, it should be stressed that the clinical starting point of these studies was not SMD, but rather patients with ADHD plus disruptive symptoms and/or maniac symptoms. Thus, the diagnosis of SMD was done retrospectively and by proxy. Risperidone, an atypical antipsychotic, is the only medication approved by the Food and Drug Administration (FDA) for irritability the SMD core symptom, in children and adolescents (Pappadoulos 2003; Stigler and McDougle 2008). The approved indication was based on trials in patients with pervasive developmental disorders (PDDs) (Aman et al. 2002; McCracken et al. 2002; Reyes et al. 2006; Pandina et al. 2007). Studies of risperidone in patients with disruptive disorders, such as conduct disorder (Findling et al. 2000) and rage outbursts (Carlson et al. 2010), have suggested its effectiveness also for treating irritability in children with average intelligence. Carlson et al. examined the safety and efficacy of liquid risperidone to reduce duration of rages in children with SMD and BD in an inpatient unit. Risperidone was effective in shortening the duration of rage episodes regardless of the diagnosis (Carlson et al. 2010). In addition, risperidone has a serotonergic mechanism of action (Klampfl et al. 2010), which may play an important role in the treatment of SMD youth, because longitudinal studies have shown a trend to depressive and anxious disorders, instead of bipolar disorder, as outcome in adulthood (Brotman et al. 2006; Leibenluft et al. 2006; Stringaris et al. 2009).
We hypothesized that risperidone might be effective in reducing irritability in children and adolescents with SMD, as shown in patients with disruptive disorders. The purpose of this open-label trial was thus to evaluate the efficacy and safety of risperidone in children and adolescents with SMD and also to further the understanding about the demographic and clinical characteristics of this very recently proposed new diagnostic entity.
Methods
This was an 8-week, open-label trial of risperidone (registered at
Subjects
Ninety-seven patients were screened by a child and adolescent psychiatrist (F.V.K.) in a clinical interview. Twenty one were invited to participate because they fulfilled the following SMD criteria: (1) age between 7 and 17 years; (2) irritability, defined by markedly increased reactivity to negative emotional stimuli manifested verbally or behaviorally at least three times weekly; (3) abnormal mood (anger or sadness), present at least half of the day, most days; (4) hyperarousal (at least three of insomnia, agitation, distractibility, racing thoughts or flight of ideas, pressured speech, intrusiveness); (5) severe impairment in at least one setting (home, school, or peers) and at least mild impairment in a second setting; (6) symptom onset before age 12 and present for at least 12 months without symptom-free periods greater than 2 months; (7) no psychotropic use within 6 months before the study.
We excluded patients with irritability who also had (1) elevated/expansive mood, grandiosity, inflated self-esteem, or episodically decreased need for sleep; (2) euphoric mood or distinct hypomanic or mania episodes greater than 1 day; (3) intelligence quotient (IQ) <70; (4) pervasive developmental disorder; (5) unstable medical illness; (6) substance abuse within the past 2 months; (7) psychosis; (8) known hypersensitivity to risperidone; and (9) current use of psychotropic medication.
Assessments
The Kiddie Schedule for Affective Disorders–Present and Lifetime version (KSADS-PL) (Kaufman et al. 1997), a semistructured diagnostic interview, was administered to parents and children by a child and adolescent psychiatrist (G.F.P.). SMD was assessed using a specifically developed KSADS supplementary module (Leibenluft et al. 2003b). Diagnosis was based on a consensus between two child psychiatrists, the one who screened the patients and the one who administered the KSADS-PL. The Wechsler Intelligence Scale for Children III (WISC III) was used to measure intelligence at initial assessment. Laboratory evaluation of liver function, cholesterol, glucose, complete blood cell count, and prolactin was performed at baseline and at the end of the study. Most patients were drug naive and the others had not been using psychotropic medications for at least 6 months.
All patients underwent an extensive evaluation with a comprehensive battery of scales assessing severity of irritability, concomitant symptoms of ADHD, anxiety, depression, mania, oppositional defiant disorder (ODD), global functioning, and adverse events. The Irritability Subscale of the Aberrant Behavior Checklist (ABC) was the main outcome variable and has 15 items. Its scores range from 0 to 45 and higher scores indicate greater severity (Aman et al. 1985a, 1985b). It includes questions about aggression, self-injury, tantrums, agitation, and unstable mood. Although it was developed for cognitively impaired patients, it is a well-validated measure for irritability (Accardo 2003). In this study, it was rated by the parents. The Clinical Global Assessment Scale (CGAS) and Clinical Global Impressions (CGI)–Severity (APA Task Force, 2000) were used to measure global functioning and were rated by the physician. The Swanson, Nolan, and Pelham Scale, version IV (SNAP-IV), a 26-item scale, was used to measure the presence and severity of ADHD and ODD symptoms and was rated by the parents (Swanson et al. 2001). The Children's Depression Rating Scale (CDRS) and the Young Mania Rating Scale (YMRS) were used to measure depressive and “B” symptoms of mania, respectively, and was rated by the physician (Poznanski et al. 1979; Youngstrom et al. 2002). The Screen for Child Anxiety-Related Emotional Disorders (SCARED) is a self-report scale for anxiety symptoms and was applied to patients above 8 years old (Birmaher et al. 1997). In addition, as a complementary source of evaluation, we assessed SMD symptoms through the Mood Symptom Questionnaire (MSQ), a recently developed scale not yet validated and it was rated by the clinician. Finally, side effects were evaluated through a list where patients and parents indicated the presence of any adverse event. The patients were evaluated by a child psychiatrist (F.V.K.) at weeks 0, 2, 4, 6, and 8 and all scales were applied in the five evaluations.
Pharmacological intervention
Risperidone was titrated to 0.06 mg/kg/day. An initial dose of 0.5 mg was given at bedtime and was increased to 1 mg on day 4. In the second week, dosage adjustment was based on efficacy and tolerability. Subjects reporting drowsiness could have medication administered as a single nightly dose or divided into twice-daily dosing. Titration was completed by the end of week 2 and the dose was maintained unless disabling side effects ensued. No other medication was allowed during the trial.
Statistical analyses
Statistical analyses were carried out using the SPSS for Windows, version 18. Tests were two-tailed and p-values of 0.05 or less were considered statistically significant. Analyses of primary and secondary outcome measures were performed using the Generalized Estimating Equation (GEE) (Zeger and Liang 1986), which provides a flexible framework for repeated measures while accounting for missing data. For the primary outcome (ABC–Irritability), we controlled for age, gender, medication dosage, co-morbidities, and body mass index separately. In the final model, we included risperidone dosage, presence of ADHD, and major depressive disorder, which were the three variables that showed a statistically significant interaction with the outcome. For secondary measures (CGI, CGAS, SNAP-IV, YMRS, CDRS, MSQ), we controlled only for risperidone dosage to avoid multiple analyses. Bonferroni test was used for post hoc analyses. For the nonsymmetric distribution of prolactin levels, we used the Wilcoxon test. For weight and laboratory data, t-test pairs were used.
Results
Nineteen patients completed the 8-week study and two patients dropped out after the baseline evaluation. Of those, one moved to another city and did not use the medication and the other was not able to begin the treatment because of family dysfunction. These two patients were included in the baseline data. The demographic and clinical characteristics of the sample are presented in Table 1. Of note, the sample was composed mainly of girls (57.1%), who had a mean age of 10.38 ± 2.78 years and a Caucasian predominance (66.7%), and the patients were from middle class (100%). Mean estimated IQ was 93.18 ± 9.22 and ADHD, anxiety disorder, and ODD were co-morbid, respectively, in 71.4%, 66.7%, and 81% of the sample. Of the 21 patients, only 4 (19%) had received previous pharmacological treatment. The mean daily dose of risperidone by the end of the study was 1.28 ±0.58 mg (range: 0.5–3 mg).
IQ = intelligence quotient.
The mean baseline and the other four-point evaluation (weeks 2, 4, 6, and 8) scores of primary and secondary outcomes are presented in Table 2. Baseline scores on ABC–Irritability were considered to be significantly elevated (mean = 25.89; standard error [SE] = 2.76), because data from studies of developmentally disabled children indicate that a score of 18 or more is considered severe impairing irritability (Marshburn and Aman 1992). Also, patients showed elevated mean baseline scores in the CGI (mean = 4.53; SE = 0.11), CDRS (mean = 34.28; SE = 1.52), SNAP-IV (mean = 1.77; SE = 0.14), SCARED (mean = 34.67; SE = 4.23), and MSQ (mean = 37.38; SE = 1.31) scales. Although mania was an exclusion criterion, we used the YMRS to evaluate “B” symptoms of mania, and the mean score at baseline was 12.66, with an SE of 1.06.
Means followed by same letters do not differ statistically considering a significance of 5%. Means followed by different letters differ statistically (p < 0.05).
Controlled for dosage, presence of attention-deficit/hyperactivity disorder, and depression.
Controlled for dosage.
ABC–Irritability = Aberrant Behavior Checklist—Irritability Subscale; MSQ = Mood Symptom Questionnaire; SCARED = Screen for Child Anxiety-Related Emotional Disorders; CDRS = Children Depression Rating Scale; YMRS = Young Mania Rating Scale; CGI = Clinical Global Impressions—Severity Scale; CGAS = Clinical Global Assessment Scale; SNAP-IV = Swanson, Nolan, and Pelham Scale—version IV; SE = standard error.
Scores of the ABC–Irritability revealed a significant reduction a long time after risperidone introduction (p < 0.001; Fig. 1). The ABC–Irritability scores at week 2 (mean = 12.03; SE = 2.94), week 4 (mean = 15.48; SE = 2.93), week 6 (mean = 12.29; SE =2.86), and week 8 (mean = 11.28; SE = 3.06) were significantly reduced compared with the baseline mean score (mean = 25.89; SE = 2.76) (p < 0.001). Interestingly, there was a slight increase in scores at week 4 compared with weeks 2 (p = 0.03), 6 (p =0.005), and 8 (p = 0.01). These analyses were limited to ADHD and MDD diagnoses and to dosage of risperidone and followed by Bonferroni test. The effect size (ES) compared with baseline was 1.39 at week 2, 1.51 at week 4, 1.77 at week 6, and 1.83 at week 8.
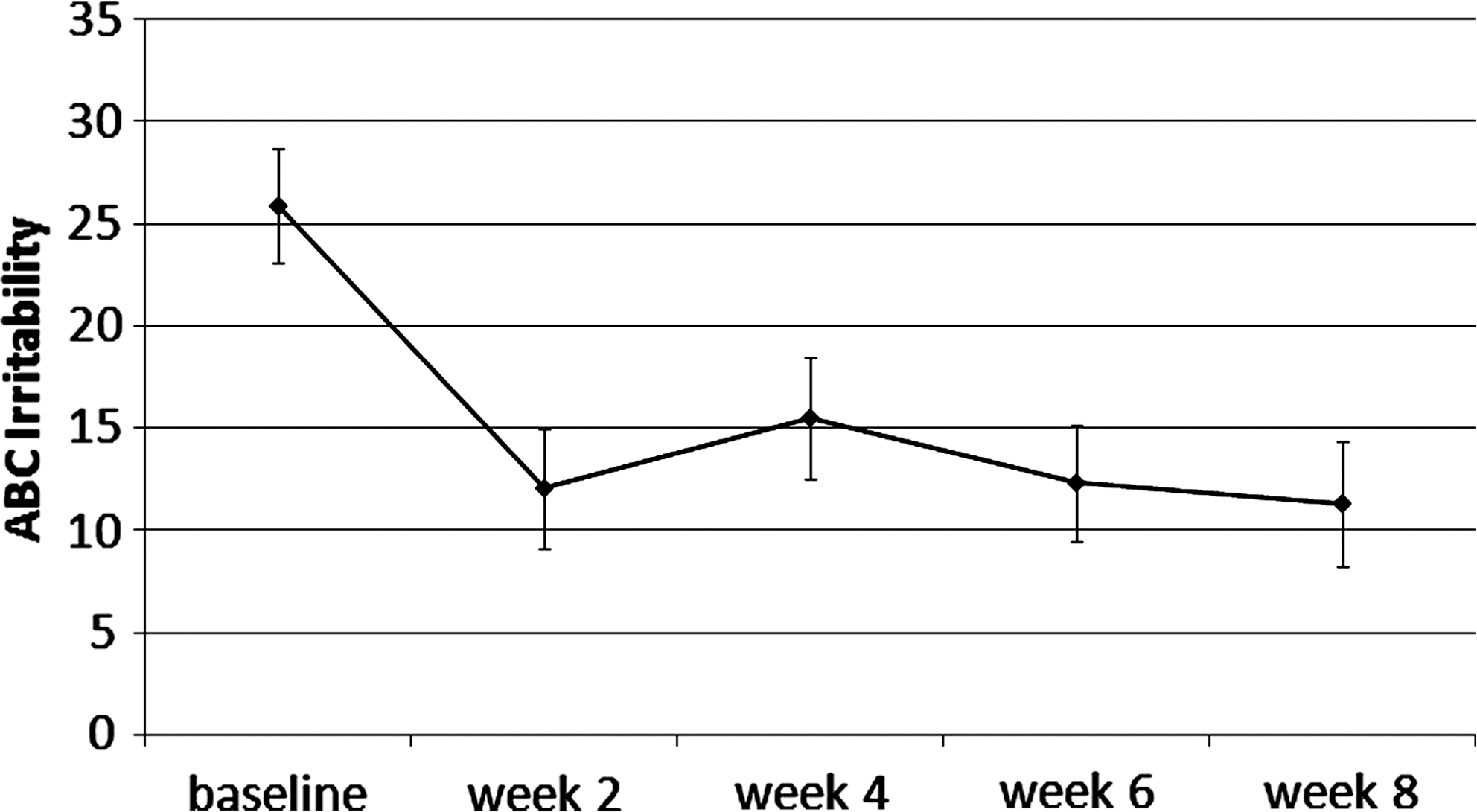
Mean scores and standard error of primary outcome during the 8-week trial.
The CGI mean scores showed a statistically significant (p < 0.001) decrease from baseline (mean = 4.53; SE = 0.11) to weeks 2 (mean = 2.85; SE = 0.10), 4 (mean = 2.96; SE = 0.20), 6 (mean = 2.69; SE = 0.19), and 8 (mean = 2.64; SE = 0.14) controlled for risperidone dosage. In addition, CGAS scores at weeks 2 (mean = 63.42; SE = 2.60), 4 (mean = 64.02; SE = 2.81), 6 (mean = 66.78; SE = 2.43), and 8 (mean = 70.97; SE = 1.87) showed a statistically significant (p < 0.001) improvement compared with baseline (mean = 46.90; SE = 1.28). Further, CGAS at week 8 showed a statistically significant improvement compared with weeks 2 (p = 0.017) and 4 (p = 0.014).
The SNAP-IV scores also decreased significantly at weeks 2 (mean = 1.11; SE = 0.12 p < 0.001), 4 (mean = 1.28; SE = 0.14 p = 0.006), 6 (mean = 1.05; SE = 0.13 p < 0.001), and 8 (mean = 1.00; SE = 0.14 p < 0.001), controlled for risperidone dosage. In addition, score at week 6 was also significantly decreased from week 4 (p = 0.03). The scores of CDRS and YMRS showed a statistically significant (p < 0.001) decrease from baseline (mean = 34.28; SE = 1.52; and mean = 12.66; SE = 1.31, respectively) at week 2 (mean = 24.11; SE = 1.32; and mean = 4.86; SE = 0.76), week 4 (mean = 26.40; SE = 2.01; and mean = 5.94; SE = 0.71), week 6 (mean = 25.93; SE = 1.59; and mean = 5.34; SE = 0.63), and week 8 (mean = 22.50; SE = 0.77; and mean =4.57; SE = 0.73). The MSQ mean scores showed a statistically significant (p < 0.001) decrease from baseline (mean = 37.38; SE = 1.31) at weeks 2 (mean = 17.48; SE = 1.88), 4 (mean =21.07; SE = 1.66), 6 (mean = 16.41; SE = 1.61), and 8 (mean =14.26; SE = 1.64). In addition, MSQ score at week 8 decreased significantly compared with week 4 (p = 0.04). Finally, the SCARED scores showed a statistically significant (p < 0.05) decrease from baseline (mean = 34.67; SE = 4.23) to weeks 4 (mean = 24.94; SE = 4.02), 6 (mean = 20.66; SE = 3.53), and 8 (mean = 20.99; SE = 4.32) controlled for risperidone dosage, followed by a significant decrease in week 6 compared with weeks 2 (p = 0.03) and 4 (p = 0.08) as well as in week 8 compared with weeks 2 (p = 0.01) and 4 (p = 0.042).
Safety and tolerability
The adverse events that emerged after risperidone onset compared with baseline levels are presented in Table 3. The most common side effects were increased appetite and sleepiness, reported roughly by half and a third of the sample, respectively.
All adverse events were scored through a self-report questionnaire.
The prolactin levels showed a statistically significant increase from baseline (10.27; standard deviation [SD] = 8.77) to week 8 (33.26; SD = 26.50) (p < 0.05). Body weight increased at week 8 (43.5; SD = 13.8) compared with baseline (41.3; SD = 13.7) (p < 0.001), with a mean variation of 6%.
Discussion
We detected a robust effect of risperidone in reducing irritability in patients with severe mood dysregulation. Our primary outcome, scores of the ABC–Irritability rated by the parents, showed a significant reduction from baseline to subsequent weeks. Although we observed a slight increase in the scores at week 4 compared with weeks 2, 6, and 8, the reduction from baseline remained significant (Fig. 1). Further, ADHD (SNAP-IV), depressive symptoms (CDRS), and global functioning (CGI and CGAS) also significantly improved from baseline. In addition, risperidone was also effective in reducing hyperarousal symptoms and the frequency of temper outbursts observed in the MSQ scores.
To the best of our knowledge, only one previous study aimed at improving symptoms in patients with SMD was described in the literature. Dickstein et al. compared lithium and placebo in a double-blind design and failed to show a significant benefit (Dickstein et al. 2009). Our a priori hypothesis was based on clinical trials of risperidone for irritability in PDD and subaverage intelligence patients (McCracken et al. 2002). Our findings concur with those previously reported of risperidone effectiveness in reducing irritability (Aman et al. 2002; Pandina et al. 2007).
Longitudinal studies in SMD showed a trend to lead to depressive and anxiety disorders and not BD as an outcome in adulthood (Brotman et al. 2006; Stringaris et al. 2009). This might explain why lithium did not show efficacy in those patients, suggesting that they do not need just a mood stabilizer. On the other hand, risperidone has a strong 5-HT2 action, which may have contributed to the improvement demonstrated in this trial (Thyssen et al. 2010).
Our sample baseline profile concurs with previous studies of this recently proposed new diagnostic entity because our patients presented high levels of impairment in school, home, and peer relations (Stringaris et al. 2010). The patients showed a mean score in CGI and CGAS of 4.53 (4 = moderately ill) and 46.9, respectively. Further, we found a similar set and prevalence of co-morbidities as reported in other studies of SMD (Dickstein et al. 2005). Criteria for ODD were met by 81% of the patients, whereas ADHD and anxiety disorders were seen in 71%. The small sample size precluded statistical analyses of co-morbidity profile.
The positive effects of risperidone occurred at a relatively low average dosage of 1.28 mg/day at the end of the study. The dose was administered using a once-daily regimen for most subjects, which may help promote adherence. Only two patients were considered noncompliant. Haas et al. (2009) showed that risperidone in low doses (0.5–2.5 mg) for children and adolescents showed a better benefit–risk profile than higher doses.
The medication was well tolerated throughout the 8-week study. No unexpected adverse events occurred. Although extrapyramidal signs are a major concern with the use of many antipsychotic drugs, they were uncommon in this trial (Table 3). The most common side effect was appetite increase and the mean weight showed a statistical increase from baseline to week 8. Weight gain may cause concern with the use of antipsychotics (Calarge et al. 2009); however, reports suggest that weight gain with risperidone is less than that with other atypical antipsychotics (Correll et al. 2009). Prolactin levels were elevated, but were not associated with clinical impairments such as galactorrhea. However, the long-term implications of prolactin elevation in children need to be better understood (Roke et al. 2009).
Our findings should be understood in the context of some limitations. We did not have a placebo arm in this trial, so we had no internal control for any effect of time (regression to the mean) or expectancy bias. However, it is important to note that there was an important overall symptomatic reduction during follow-up, according to parents in both the ABC and the SNAP-IV and to patients in the SCARED. Another limitation is that some scales were completed by the same child psychiatrist (CDRS, YMRS, MSQ, CGI, and CGAS) without a previous reliability assessment. Our sample size was small, but not significantly smaller than the only previous study in literature. The majority of the patients were of a European ancestry. So, our findings might not generalize to other ethnic groups.
Conclusion
Low doses of risperidone produced both statistically and clinically significant improvement in patients with SMD, particularly in reducing irritability. Our findings suggest that risperidone might be an efficacious and well-tolerated therapeutic choice. However, the design of our study allowed us to provide only class IV evidence for this therapeutic effect, and further controlled trials have now a clear rationale to assess symptoms in this group of children with severe irritability, temper outbursts, and other emotional symptoms.
Clinical Significance
This is the first trial with positive results in youth with severe mood dysregulation. Although this entity awaits validation, children and adolescents with chronic irritability, temper outbursts, and mood liability are common in clinical settings. Thus, the need for studies targeting therapeutic interventions for this population is clear.
Footnotes
Disclosures
Drs. Fernanda Krieger, Gabriel Pheula, and Silzá Tramontina have nothing to disclose. Roberta Coelho and Thamis Zeni have nothing to disclose. Dr. Cristian Zeni has received travel grants from Abbott to attend national research meetings. Dr. Luis Augusto Rohde was on the speakers bureau and/or acted as consultant for Eli-Lilly, Janssen-Cilag, Novartis, and Shire in the last 3 years (less than US$10,000 per year and reflecting less than 5% of his gross income per year). He also received travel awards (air tickets and hotel) to take part in two Child Psychiatric Meetings from Janssen-Cilag and Novartis in 2010. The ADHD and Juvenile Bipolar Disorder Outpatient Programs chaired by him received unrestricted educational and research support from the following pharmaceutical companies in the last 3 years: Abbott, Bristol-Myers Squibb, Eli-Lilly, Janssen-Cilag, and Novartis.
The medication was provided by Aché Pharmaceutical Company without any interference in the study.
Acknowledgments
The authors thank Laboratorios Aché, for providing the medication without any interference in the study. Finally, the authors thank the patients and families who participated and made this study possible.