
Abstract
Background:
This study evaluated the potential benefits of a centrally acting selective serotonin reuptake inhibitor, sertraline, versus placebo for prevention of symptoms of posttraumatic stress disorder (PTSD) and depression in burned children. This is the first controlled investigation based on our review of the early use of a medication to prevent PTSD in children.
Methods:
Twenty-six children aged 6–20 were assessed in a 24-week double-blind placebo-controlled design. Each child received either flexibly dosed sertraline between 25–150 mg/day or placebo. At each reassessment, information was collected in compliance with the study medication, parental assessment of the child's symptomatology and functioning, and the child's self-report of symptomatology. The protocol was approved by the Human Studies Committees of Massachusetts General Hospital and Shriners Hospitals for Children.
Results:
The final sample was 17 subjects who received sertraline versus 9 placebo control subjects matched for age, severity of injury, and type of hospitalization. There was no significant difference in change from baseline with child-reported symptoms; however, the sertraline group demonstrated a greater decrease in parent-reported symptoms over 8 weeks (−4.1 vs. −0.5, p=0.005), over 12 weeks (−4.4 vs. −1.2, p=.008), and over 24 weeks (−4.0 vs. −0.2, p=0.017).
Conclusions:
Sertraline was a safe drug, and it was somewhat more effective in preventing PTSD symptoms than placebo according to parent report but not child report. Based on this study, sertraline may prevent the emergence of PTSD symptoms in children.
Introduction
Preventative strategies for PTSD are needed, because this disorder has been described in up to 50% of burned children in a series of studies at a major pediatric burn center (Stoddard et al. 1989, 2002, 2006b; Saxe et al. 2005). Further, PTSD has been diagnosed in between 20% and 40% of burned children and adults in other studies. Strategies to prevent PTSD such as those studied here are also important, because PTSD causes tremendous problems for a child's social, educational, and biological development. Children with PTSD are often so preoccupied with intrusive recollections and so hyperaroused that they have difficulty processing social information. These symptoms can continue into adulthood. This preoccupation with the trauma and extreme levels of arousal interfere with learning at school. Traumatized children frequently are so frightened that the traumatic event will recur that they avoid social situations and school. Children with trauma histories may also develop mood, anxiety, sleep, conduct, elimination, learning, and attentional problems (Pelcovitz and Kaplan 1996; Pynoos 1996; Stoddard et al. 2002, 2006b; Saxe et al. 2005).
Although no studies based on our review have investigated sertraline in preventing childhood PTSD, research and clinical practice at a major pediatric burn center and elsewhere indicate that it is effective in treating anxiety disorders and depression in children (Table 1). Sertraline showed efficacy in the Pediatric OCD Treatment Study (POTS) Team (2004) and the Child/Adolescent Anxiety Multimodal Study (Walkup et al. 2008; Compton et al. 2010). However, for PTSD, the most recent large double-blind study of sertraline treatment of PTSD in children did not show it to be effective (Robb et al. 2010). There is no Federal Drug Administration (FDA)-approved drug treatment for PTSD in children (Patient Medication Guide, 2009; Foa et al. 2009). Research indicates that sertraline is effective in treating PTSD in adults, perhaps by stimulating production of brain-derived neurotropic factor (BDNF) (Table 2). In fact, sertraline and paroxetine are the only two FDA-approved medications for the treatment of PTSD in adults (National Center for PTSD Fact Sheets 2008). Sertraline was approved by the FDA in 2000 (Henney 2000).
DB=double-blind; DBPC=double-blind placebo-controlled; MDD=major depressive disorder; TF-CBT=trauma-focused-cognitive behavioral therapy; OCD=obsessive compulsive disorder; CGAS=Children's Global Assessment Scale; RCT=randomized controlled trial; GAD=generalized anxiety disorder; PTSD=posttraumatic stress disorder.
DB=double-blind; DBPC=double-blind placebo-controlled; PTSD=posttraumatic stress disorder.
The use of antidepressants to treat PTSD in burned children and in adults has become common in clinical practice, despite limited empirical evidence to support this (Ciraulo et al. 2004; Stoddard et al. 2006a). In this article, we examine empirical support for medications to prevent PTSD. Our research team previously demonstrated that the risk of PTSD can be diminished via the use of psychoactive agents in the acute traumatic period, that is, that the dose of morphine a burned child received while in hospital predicted the attenuation of PTSD symptoms over 6 months after discharge (Saxe et al. 2001, 2005; Stoddard et al. 2009). Subsequent research has supported this effect of morphine with adult patients with PTSD (Bryant et al. 2009; Holbrook et al. 2010). This finding led to a search for other agents to diminish the risk of PTSD in children. This study presents the results of the double-blind placebo controlled study of sertraline and is a primary result of this line of research.
In contrast to the prevention of pain, the pharmacologic prevention of anxiety disorders associated with burns and injuries was not, until this study, a major focus of research. Although acute treatment of anxiety with benzodiazepines is widely practiced, and one study in adults was suggestive that they might result in increased PTSD symptoms (Gelpin et al. 1996), this has not been substantiated. PTSD is the most prominent of several anxiety disorders associated with burns/injuries, with others including phobias, panic disorder, and generalized anxiety disorder. PTSD is associated with co-morbid depression in up to 50% of cases (Stoddard et al. 1989; Shalev et al. 2008). In light of the increased understanding of its course and neurobiology, prevention of PTSD may now be possible (Pitman and Delahanty 2005). This study is an investigation of sertraline, one candidate medication in common therapeutic use.
Methods
Subject selection
The following inclusion and exclusion criteria were used when screening for eligible participants: The inclusion criteria were as follows: All English- and Spanish-speaking children between the ages of 6 and 20 years admitted to a major pediatric burn center for an acute burn or for reconstructive burn surgery. Their experience of acute trauma should meet the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association 1994) A1 stressor criterion, that is, actual or threat of serious injury evaluated with the Diagnostic Instrument for Children and Adolescents, and the child's response meets DSM-IV A2 response criterion: Fear, helplessness, or horror based on Diagnostic Instrument for Children and Adolescents. The parent or guardian should have proficiency in English or Spanish that is sufficient for the consent and survey process. The acute stressor for the patients with acute burn was the burn (n=12), and for the patients who had undergone reconstructive surgery, it was the surgery (n=14), which may trigger burn-related PTSD symptoms. The exclusion criteria were as follows: No memory of the injury, current use of antidepressants, known hypersensitivity to sertraline, diagnosis of bipolar disorder, diagnosis of PTSD immediately before burn injury or reconstructive surgery, mental retardation, or a traumatic brain injury. No remuneration was provided to participants, in accord with the policies of the major pediatric burn center.
The study assessed sertraline as a potential preventive agent for PTSD. The research team managed the implementation of the study protocol. The protocol was approved by the Human Studies Committees of Massachusetts General Hospital and Shriners Hospitals for Children. The team worked in close collaboration with the clinical care burn teams in the acute, reconstructive, and outpatient services. The study rigorously screened and carefully enrolled eligible subjects. The a priori randomization ratio of drug:placebo was 2:1.
Twenty-six children enrolled in the study. One participant withdrew consent before starting study medication. The final sample included 17 participants assigned to the treatment group and 9 participants assigned to the control group. The sample size had 80% power to detect an effect size of 1.20. Eighty families of patients declined to participate. The reasons for declining were obtained for 70 nonparticipants as detailed in Table 3.
FDA=Federal Drug Administration; SSRI=serotonin-selective reuptake inhibitor.
The mean age of the participants who received study medication (n=26, 9 females and 17 males) was 12.35 years (standard deviation=3.71). The racial and ethnic makeup of these participants was as follows: 46.2% of the participants identified as White/Caucasian, 30.8% of the participants identified as Black or African-American, and 23.1% of the participants identified as Latino (Table 4). Of those children admitted to the major pediatric burn center, 12 were admitted for an acute burn, and 14 of the children were admitted for burn reconstructive surgery. The burn injuries were primarily due to flame injuries, and the average total body surface area (TBSA) among children with burns was ∼36.2%, with a range of 4%–85%, similar to that in the population of children admitted to the major pediatric burn center.
TBSA=total body surface area burned; mg=milligrams.
As previously stated, one participant withdrew consent before starting the study medication. In this study, in accord with our previous experience, sertraline was a safe and useful medication for children with severe trauma. The factors that reduced recruitment included few eligible English-speaking admissions and the black box warning by the FDA regarding increased risk of suicidality in children. A section was added to the Consent Form about risk of worsening depression or suicidal ideation (Zohar et al. 2002). There was increased frequency and scrutiny in clinically assessing anxiety, agitation, and suicidal ideation and monitoring for any spontaneous reports. One subject, whose burn was due to matchplay, was reported after discharge by his mother to have “tremors” and a single incident of suicidal ideation when stressed with his mother. The tremors stopped after 1 week. No suicidal ideation was present when this was evaluated, nor on follow-up monitoring. This was reported to the Data Safety Monitor, who concurred with reducing the “dose” (the Monitor did not advise breaking the blind) from 75 to 50 milligrams (mg)/day. He completed the study.
Recruitment of subjects was conducted by the principal investigator, the attending surgeon, and study staff, educating families about the purpose of the study and protocol. Once deemed appropriate for inclusion, the patient and the parents/legal guardian were informed of the risks and benefits of the study. If the child and family agreed, they signed Informed Consent and Research Assent and the HIPPA Confidentiality Form.
Child measures
Diagnostic Interview Schedule for Children and Adolescents
This is a semistructured interview schedule that was administered to English-speaking children to assess PTSD symptoms at Baseline, weeks 8, 12, and 24. The Diagnostic Interview Schedule for Children and Adolescents (DICA) is normed for use with English-speaking populations (Reich 2000).
Children's PTSD Inventory
The Children's PTSD Inventory (CPTSDI) was administered for Spanish-speaking children. The CPTSDI is normed for use with Spanish-speaking populations. (Note, see also Results: One Spanish speaking subject was enrolled. He was in the control group, and his parent ratings for PTSD were not completed) (Saigh et al. 2000).
The Child Depression Inventory
This is a 27-item, age- and gender-normed self-report instrument assessing current depressive symptoms in children and adolescents. Scores on the Child Depression Inventory (CDI) range from 0 to 54, with higher scores indicating more severe depressive symptomatology (Smucker et al. 1986). The CDI has high internal consistency, moderate test-retest reliability, and correlates positively with related constructs such as self-esteem, negative cognitive attributions, and hopelessness (Kendall et al. 1989; Kazdin 1990). The CDI is normed for use with both English- and Spanish-speaking populations. The CDI was administered to children at Baseline, as well as at weeks 2, 4, 8, 12, and 24 (Kovacs 1985).
Parent/guardian measures
Diagnostic Interview Schedule for Children and Adolescents
This is a semistructured interview schedule that is administered to English-speaking parents/legal guardians to assess the child's PTSD symptoms at Baseline, weeks 8, 12, and 24 (Reich 2000).
A Safety Monitoring Board monitored for possible behavioral complications or adverse drug effects, to assure optimal care. In one instance, the child psychiatrist safety monitor determined that a child, who had consented and developed a seizure disorder before starting the study medication, had withdrawn from the study and never received the study medication. In the other instance, described above, the patient completed the study.
Design
The design of the study follows a random double-blind assignment of 26 children to either the treatment (n=17) or placebo-control condition (n=9) stratified by potential moderators of treatment outcome such as age, TBSA/injury severity, and type of hospitalization (acute vs. reconstructive). The statistician generated the random number sequences, whereas the pharmacist assigned participants to their groups. The drugs were administered for 24 weeks on a flexible fixed schedule beginning at 25 mg/day and increasing as high as 150 mg/day. Both groups received the assigned medication and dose over a 24-week period.
All children and families were assessed at six time points: Baseline, and weeks 2, 4, 8, 12, and 24. Follow-up assessments were completed at the hospital, clinic, or, if the child had been discharged, by telephone or at home. The assessments were to be done with families in both the sertraline and placebo conditions at each follow-up assessment point whether or not the study medication treatment was terminated.
In addition to these assessments, there was weekly monitoring through 14 weeks and at 18 weeks with the child and parent to assess the effects of the study medication, and of its discontinuation at week 12. At week 12, the medication was tapered at a rate of 25 mg every 3 days until it was discontinued. All investigators were blind to the medication status of the subjects.
Data Analysis
The primary independent variable was the child's medication assignment to either the sertraline or placebo group. The primary dependent variable was the child's posttraumatic stress symptoms as measured by both parent- and child-rated questionnaires. Two sample t-tests were conducted to determine whether there were any significant differences between the two treatment groups in the change of child- and parent-reported PTSD symptoms over the follow-up periods (see Tables 4 and 5).
PTSD=posttraumatic stress disorder.
Results
All subjects participated without adverse effects except for one subject as noted previously. Table 4 displays the demographic information and medication doses for all the randomized participants in the study.
The mean CDI score was slightly higher in the placebo group (10.7 vs. 6.5, p=0.076) at baseline. The mean CDI score decreased from baseline in both groups during the follow-up period; however, the placebo group showed significantly greater decreases than the sertraline group at week 8 (−7.6 vs. −1.6, p=0.05) and week 12 (−7.5 vs. −2.4, p<0.001).
The mean child-reported DICA PTSD symptoms decreased from 8.8 at baseline to 4.3 at week 24 in the sertraline and from 10.0 to 6.3 in the placebo group. The change from baseline was not significantly different between the two groups at follow-up (Table 5). However, the parent-reported DICA PTSD symptoms showed significantly greater improvement in the sertraline group at all three follow-up times (Table 6 and Fig. 1): −4.1 versus −0.5 at week 8 (p=0.005), −4.4 versus −1.2 at week 12 (p=0.008), and −4.0 versus −0.2 at week 24 (p=0.017). As indicated in Table 6 and Figure 1, two parents in the placebo group did not complete the parent-reported PTSD symptom assessments at week 8, and one of them also did not complete the assessment at week 12. They both reported higher-than-group average parent-reported PTSD symptoms on the DICA at week 24. Therefore, the results were unlikely to change had they completed the weeks 8 and 12 assessments.
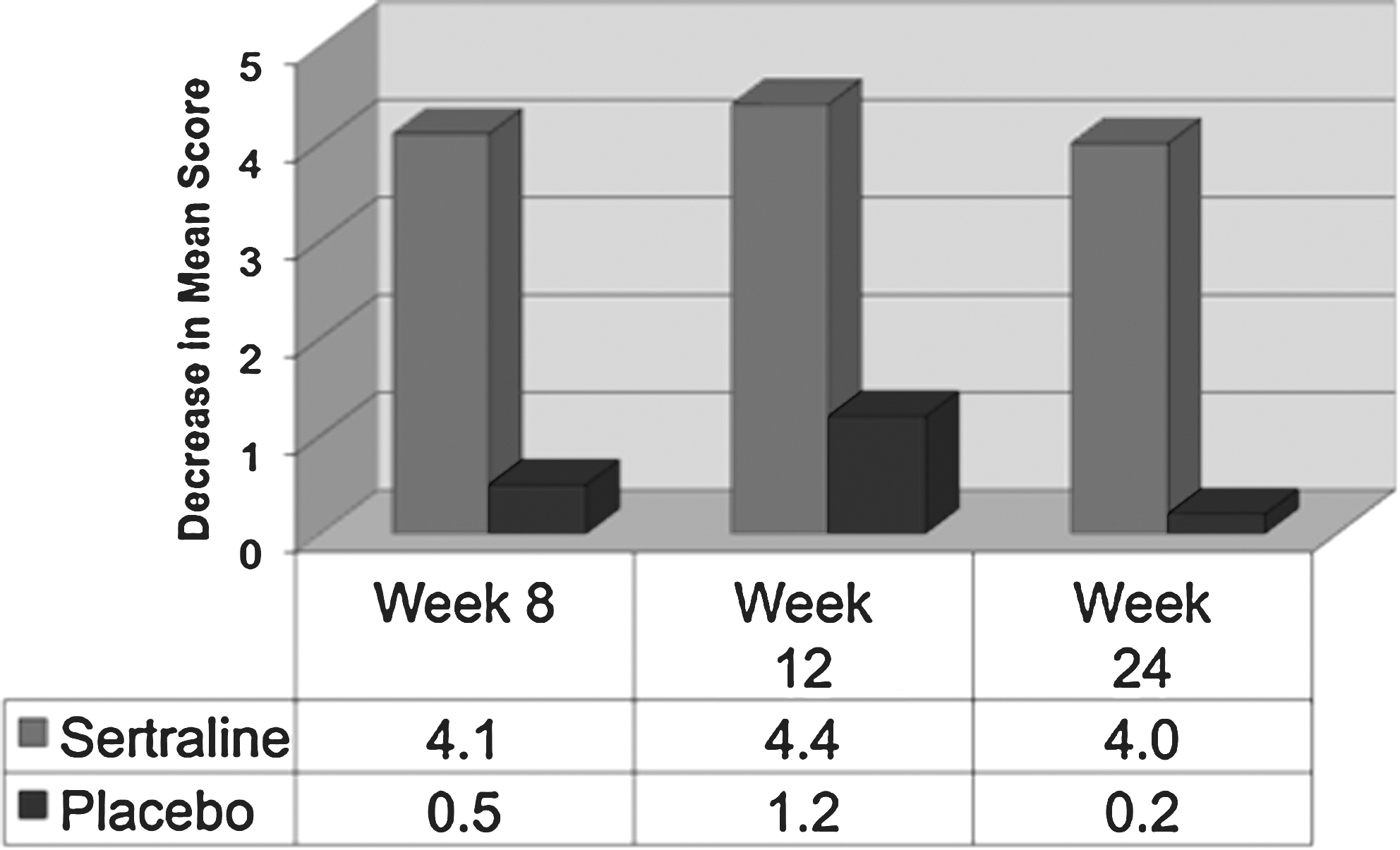
Mean parent-reported posttraumatic stress disorder (PTSD) score change from Baseline over 24 weeks: Sertraline versus placebo.
The FDA advisory on antidepressants stemmed from data suggesting a small risk of worsening depression and suicidal ideation (Ryan 2005) and determined that a Patient Medication Guide (2009) should be given to children receiving antidepressants. This study complied with the advisory and supports the safety of sertraline in this sample.
Discussion
There is continuing need for an evidence base for pharmacological agents to prevent the emergence of PTSD after trauma (Stoddard and Todres, 2001).8 Although some preventive benefit has been established for cognitive behavior therapy (CBT) (March et al. 1998), identifying the pharmacological agents most effective in PTSD prevention has been an elusive goal, in part due to the challenge of administering an agent shortly after a severe trauma, without certainty that they are at risk for PTSD.
Although the mechanism by which sertraline might prevent PTSD is beyond the scope of this study, it is of interest that cotreatment with antidepressants during stressor induction can block at least some of the stressor-induced changes in brain-derived neurotrophic growth factor (BDNF) gene expression (Smith et al. 1995). Further, Smith et al. (1997) demonstrate that BDNF and NT-3 mRNA are stress-responsive genes and that alterations in these may account for some of the effects of stress on the hippocampus. Finally, there is early research investigating stress-protective effects of sertraline on gene expression regulating the development of prefrontal cortex cytoarchitecture (Levine 2005). For these reasons, it was selected as the candidate agent to be used to prevent PTSD in burned children.
How are the findings to be understood? First is the finding on the CDI indicating that depressive symptoms in the placebo group showed significantly greater decrease than in the experimental group. Although there is no clear explanation, at baseline the placebo group had more depressive symptoms, which then tapered with usual treatment. No other patient characteristics between the groups were identified to explain this finding. Since the placebo group was more depressed initially, a rapid reduction in symptoms was likely once the acute stress ended, rendering it more difficult to demonstrate significance in the reduced depressive symptoms in the experimental group.
The findings on posttraumatic stress symptoms, based on parent report (Table 6), are significant in substantiating the original hypothesis and suggest that this pharmacotherapeutic approach to prevention may be effective. The parents' observations in the experimental subjects compared with the placebo group indicate that there was a small benefit in this population of sertraline in reducing posttraumatic symptoms in these severely burned children. This finding is consistent with clinical observations of benefit in fewer PTSD symptoms with sertraline in burned children. However, despite the evidence previously cited that sertraline and other antidepressants are effective in treatment of PTSD in adults, the child-rated PTSD symptoms in this preventive study and the previously cited treatment study by Robb et al. (2010) did not find any benefit of sertraline over placebo.
The findings based on child report are more difficult to interpret than the parent assessments (see also below, placebo group), as they did neither achieve significance nor conform to previous clinical observations. The children's ratings did show a trend in favor of the placebo group and did not substantiate the original hypothesis.
Placebo Group: A factor affecting the results is the severity of symptomatology in the control group of nine subjects who received the placebo. At baseline, this was a highly symptomatic group, with more depressive symptoms than the experimental drug group (a mean symptom score of 10.7 vs. 6.5 for the experimental group). There was no significant difference in PTSD symptoms. A secondary result of this study supports the efficacy and safety of sertraline use in children and adolescents. Evidence of increased suicidal ideation was identified very briefly in one subject who completed the study.
This rigorous, double-blind, placebo-controlled study with a severely traumatized population of burned children provides some support for the effectiveness of sertraline in reducing PTSD symptoms in traumatized children. If replicated, it has implications for preventive treatment for traumatized children, as an early intervention after trauma may mitigate against the pathological effects of the emergence of PTSD. Sertraline, therefore, should be considered on the list of possible agents to reduce PTSD symptoms in children. Other possible agents include propranolol, morphine, and imipramine, but the first has no study in children to support it, and the latter two have only pilot studies. This is the only preventive study to date of sertraline versus placebo in children using a double-blind, placebo-controlled design, and, therefore, is of particular merit.
What are the advantages of sertraline, compared with other potential agents? Walkup et al. (2008) in a treatment study of 488 children with anxiety disorders aged 7–17 provide support for the effectiveness of sertraline treatment, but even greater support for combined sertraline and CBT treatment. That study is consistent with the findings of a study of 22 children with PTSD symptoms in a randomized controlled trial (RCT) study, which found a more modest benefit of combined treatment of sertraline and CBT (Cohen et al. 2007).
This study provides support for the findings from a retrospective study of large samples, with another serotonin-selective reuptake inhibitor (SSRI) (fluoxetine) and imipramine, reported by Tcheung et al. (2005), and of an earlier pilot study of imipramine (Robert et al. 2000). Sertraline has neither the risk of cardiac arrhythmia and possible death of imipramine nor the risk of adverse effects on blood pressure of imipramine and propranolol. The FDA advisory warns about possible emergence of suicidal ideation with all antidepressants (Ryan 2005). As noted earlier, one instance of suicidal ideation occurred in the present study. In contrast with morphine, which has little practical role in general pediatrics except in the hospital, sertraline is a known agent, which is generally safe and in wide use for depression and anxiety disorders in children.
A limitation of this study is the sample size. However, one of the few other studies of children had a final sample of only 22 participants (Cohen et al. 2007). Despite very common use of a wide range of drugs in the injured, medically hospitalized, and children with trauma, it is difficult to recruit large samples for acute pharmacological studies due to the stressful situation and due to reluctance to engage in research. This results in a very limited evidence base, despite rapidly expanding use of psychopharmacological agents in children. This is a unique RCT study. The results of this study may be less robust than hypothesized, because the placebo group was more symptomatic than the sertraline group at baseline. A further reason may be that unlike in other PTSD prevention studies, the subjects were not selected based on maximal PTSD symptoms, but rather because they were experiencing a severe stressor, which is commonly associated with these symptoms. As a result of random selection, the degree of response to medication was likely less than it would have been had patients who were maximally symptomatic been selected.
Conclusions
In summary, this article presents a double-blind, placebo-controlled study of the pharmacological prevention of PTSD symptoms in severely burned children. The findings indicate that sertraline was somewhat more effective in preventing the emergence of PTSD symptoms than placebo, according to parent report but not child report. The finding of no benefit compared with placebo by child report is similar to that in the study of Robb et al. (2010).
Clinical Significance
This study is the first double-blind, placebo-controlled trial of any medication for the prevention of PTSD among children and adolescents. It is one of the few pediatric pharmacology studies of children with injuries, a population for whom preventative strategies for PTSD are much needed. Further, the study is a clinical trial of an SSRI, a class of drugs that is often prescribed for injured children without evidence of safety or efficacy. Based on this study, sertraline is a safe drug for use in this population. The study provides some support for the hypothesis that sertraline may prevent the emergence of PTSD symptoms in burned children.
Footnotes
Disclosures
The experimental drug and placebo were provided by Pfizer Pharmaceuticals. Dr. Stoddard reports no other disclosures related to this study. Dr. Rohini Luthra reports no disclosures. Erica A. Sorrentino reports no disclosures. Dr. Glenn N. Saxe reports no disclosures. Jennifer Drake reports no disclosures. Dr. Yuchiao Chang reports no disclosures. Dr. John B. Levine reports no disclosures. Dr. David S. Chedekel reports no disclosures. Dr. Robert L. Sheridan reports no disclosures.
Acknowledgments
This study was supported by Grant # 8840 from the Shriners Hospitals for Children to Dr. Stoddard. Grant Support for Dr. Levine includes the Shriners Hospital for Children—Boston—and Centers for Disease Control and Prevention, Grant number 5R01DP000339, and the John Henry Foundation, The Benson-Henry Institute for Mind Body Medicine, Massachusetts General Hospital.
Name of Department and Institution where work was done: Department of Psychiatry, Shriners Hospitals for Children-Boston, MA.
Statistical Consultant: Yuchiao Chang, Ph.D., Massachusetts General Hospital, Boston, MA.
Clinical Trials Registry: “A Study of Sertraline to Prevent PTSD,”