
Abstract
Objective:
The objective of this study was to explore whether the addition of olanzapine versus placebo increases weight gain and improves psychological symptoms in adolescents with anorexia nervosa-restricting type who are participating in a comprehensive eating disorders treatment program.
Methods:
Twenty underweight females participated in this 10-week, double-blind, placebo-controlled pilot study of olanzapine. The primary efficacy measure was change in percentage of median body weight measured at baseline and weeks 5 and 10. Secondary efficacy measures included clinician-rated and self-reported measures of psychological functioning measured at 2-week intervals and eating disorder symptoms measured at baseline and weeks 5 and 10 as well as laboratory assessments (including indirect calorimetry), which were also performed at baseline and weeks 5 and 10. A mixed models approach to repeated measures analysis of variance was utilized to detect any treatment-by-time interaction.
Results:
Fifteen of 20 enrolled females (median age, 17.1 years; range, 12.3–21.8 years; mean body mass index, 16.3) completed this 10-week pilot study. Change in % median body weight did not differ between the treatment groups at midpoint or end of study. Both groups gained weight at a similar rate and had similar improvements in eating attitudes and behaviors, psychological functioning, and resting energy expenditure. A trend of increasing fasting glucose and insulin levels was found only in the olanzapine group at week 10.
Conclusions:
These preliminary findings do not support a role for adjunctive olanzapine for underweight adolescent females with anorexia nervosa-restricting type who are receiving standard care in an eating disorder treatment program (clinical trials.gov; no. NCT00592930).
Introduction
The 5-HT neuronal systems contribute to modulation of appetite, motor activity, mood, and obsessional and impulse control. Drugs that act on the 5-HT system, such as the second-generation antipsychotic medication olanzapine, may have some efficacy in the treatment of AN (Kaye et al. 2005).
We wanted to explore whether a contributing factor to the olanzapine-induced weight gain seen in other patient populations was a reduction in resting energy expenditure (REE) and altered metabolism of energy substrates, including carbohydrate, protein, and fat, as measured by the Respiratory Quotient (RQ). We hypothesized that REE during the course of nutritional rehabilitation would be lower than expected in the olanzapine-treated group (Schebendach et al. 1997; Graham et al. 2005; Sharpe et al. 2005). We also wanted to explore whether olanzapine may be efficacious in ameliorating body image distortion.
To assess feasibility, as well as to gather preliminary data on efficacy and safety measures, a sample size of 20 females with AN-R was chosen for this randomized, parallel-group, 10-week, double-blind, placebo-controlled pilot study of adjunctive olanzapine. We hypothesized that adjunctive treatment with olanzapine, in comparison to placebo, (1) increases weight gain as measured by change in percentage of mean body weight (% MBW) in underweight adolescents with AN-R and (2) increases glucose and insulin levels, but is otherwise safe and well tolerated, (3) decreases associated eating disorder symptoms, and (4) decreases REE and substrate utilization (RQ).
Methods
Study participants
All females receiving treatment for AN at our medical center's Eating Disorder Treatment Program for adolescents over a 4-year period were screened for eligibility. Participants could be inpatient, those attending day hospital, or outpatients at study entry. Females between 12 and 21 years of age with a primary diagnosis of AN-R as determined by the Eating Disorder Examination (EDE) (Fairburn and Cooper 1993) or Eating Disorder Not Otherwise Specified if the sole criterion not met was 3 months of amenorrhea were eligible to participate. Patients were excluded if they met criteria for past or current binge/purge type in an attempt to increase homogeneity in this small sample. At our center, pharmacotherapy for the binge-purge subtype tended to consist of selective serotonin reuptake inhibitors, prescribed off-label, whereas the AN-R group was felt to be more resistant to available treatments. Patients were also excluded if they were judged to be a serious suicidal risk, had prior treatment with olanzapine, or were not on a stable medication regimen for 8 weeks prior to study entry. After a full explanation of the study, patients over age 18 signed an informed consent document approved by our medical center's institutional review board. Patients under age 18 gave written assent and a parent or guardian gave written consent. All participants received individualized medical care, nutritional management, and psychological treatment consisting of individual, group, family, and multifamily group therapy at our center's eating disorders program. Intensity of treatment was determined by the eating disorders clinical team. Inpatients were treated on an adolescent medicine unit of a children's hospital and attended the day-hospital program on weekdays. Day-hospital patients attended the program on weekdays and had three meals and two snacks supervised by staff. Outpatients generally had weekly visits with an adolescent medicine physician, a nutritionist, and a psychotherapist experienced in treating eating disorders and did not attend the eating disorder program's group or family therapy sessions. Changes in the intensity of care provided were structured such that participants could move through varying levels of care based on their clinical needs as determined by the eating disorders treatment team. Typically, treatment intensity was decreased when weight gain goals set by the clinical team were met so that inpatients were “stepped down” to day hospital and then to outpatient treatment.
Study procedures
The research pharmacist randomly assigned participants to receive olanzapine or matching placebo using a computer-generated table for inpatients or outpatients. Randomization was stratified by inpatient versus day hospital or outpatient status at study entry. Study and treatment personnel were blinded to treatment assignment. Olanzapine or matching placebo started with a 2.5 mg single oral dose in the evening or at bedtime for 1 week. The daily dose was increased by 2.5 mg each week to a target dose of 10 mg/day by week 4. Dosage was decreased if intolerable side effects occurred. Medication adherence was assessed by participants' self-report and by olanzapine serum levels drawn at weeks 5 and 10. The olanzapine levels were stored in a freezer and sent to Eli Lilly for analysis after all subjects completed the study.
Measurements
The primary efficacy measure was % MBW at weeks 0 (baseline), 5, and 10. Participants were weighed in a hospital gown and underwear after voiding and prior to eating in the morning. Body mass index (BMI) was calculated from height and weight using the following formula: BMI = weight (in kilograms) divided by the height (in meters) squared. Median BMI was defined as the 50th percentile of BMI for age and gender using the 2000 CDC growth curves for children and adolescents (Kuczmarski et al. 2000). % MBW was defined as measured BMI divided by median BMI and multiplied by 100.
Tolerability of medication was assessed weekly by the research psychiatrist by physical examination including blood pressure and pulse obtained in the sitting and standing positions and by assessment of extrapyramidal symptoms. After a physical exam and patient interview, the occurrence and intensity of adverse effects were recorded on the Treatment Emergent Side Effects Scale (TESS) Symptom Intensity Catalog (Guy 1976), a 48-item structured adverse events scale. Laboratory measures included fasting glucose, fasting insulin, complete blood counts, and electrocardiogram at weeks 0, 5, and 10. Electrocardiograms were interpreted by a consulting pediatric cardiologist who was blind to group assignment.
Changes in general psychiatric symptoms were assessed at weeks 0, 2, 4, 6, 8, and 10 by the research psychiatrist, using clinician-administered rating instruments, including the Hamilton Depression Rating Scale (HDRS) (Williams 1988) and the Brief Psychiatric Rating Scale (Woerner et al. 1988). Eating disorder symptoms were assessed by the EDE (Fairburn and Cooper 1993) and the Yale-Brown-Cornell-Eating Disorder Scale (YBC-EDS) (Mazure et al. 1994); both instruments were administered by an experienced licensed doctoral-level clinical psychologist at weeks 0, 5, and 10. The EDE is a semistructured interview schedule that assesses a patient's eating disorder symptoms. The four subscale scores (Restraint, Eating Concern, Weight Concern, and Shape Concern) represent an average of items included in that category. A total or global score comprised of an average of the four subscales is also recorded. The YBC-EDS assesses the severity of the eating disorder. The scale contains 19 individual items, 2 global severity items, and 1 reliability item. Two parallel sets of four symptom items are grouped to generate a Preoccupation Subtotal and a Ritual Subtotal, which are combined to report a Total score. A fourth group of six items forms a Motivation to Change Total spanning both eating-related preoccupations and rituals. Higher scores indicate more pathology.
To explore whether olanzapine was helpful in ameliorating body image distortion, a body image assessment adapted from the work by Williamson et al. (1987, p. 466) was administered at baseline and weeks 5 and 10. The adaptation consisted of presenting nine numbered silhouettes ranging from emaciated (1) to obese (9) on a single sheet of paper. Participants were asked to answer the following four questions: (1) “Which do you think is ideal for others?”; (2) “Which do you think is ideal for yourself?”; (3) “Which one do you think you look like now?”; and (4) “Which one do you feel you look like now?”
REE and RQ were measured after a 12–14-hour overnight fast, using an open circuit, flow-through, ventilated-hood computerized indirect calorimeter (Datex Deltatrac II; Sensor Medics, Anaheim CA). Patients remained awake and in a supine position throughout the study. The calorimeter was calibrated to a known gas prior to measurement, and oxygen consumption (VO2) and carbon dioxide (VCO2) production were measured over a 30-minute period. Calculation of REE and RQ were made by the onboard computer of the calorimetry system. Studies were conducted at weeks 0, 5, and 10.
Data analytic methods
The demographic variables of age, weight, height, days inpatient, days in day hospital, and days in outpatient treatment were compared between the two treatment groups using two-sample t-tests. BMI, % MBW, physiological data, adverse events as rated on the TESS, eating disorder symptoms, and general psychological symptoms were examined using repeated measures analysis of variance with a mixed models approach to determine whether the treatment groups behaved differently across the time points (i.e., the treatment group-by-time interaction). A priori pairwise comparisons examining changes across treatments between the groups were conducted using t-tests. All analyses were of intention-to-treat type.
Results
Of the 94 eligible participants identified from consecutive admissions to our eating disorder treatment program, 74 (78.7%) declined study participation, greatly prolonging the time needed to recruit our 20 participants (Fig. 1). The most common reasons cited for declining to participate were not wanting to gain any weight or wanting to gain weight without the use of medication. Enrolled participants did not differ in age mean, BMI, or % MBW from those who declined.
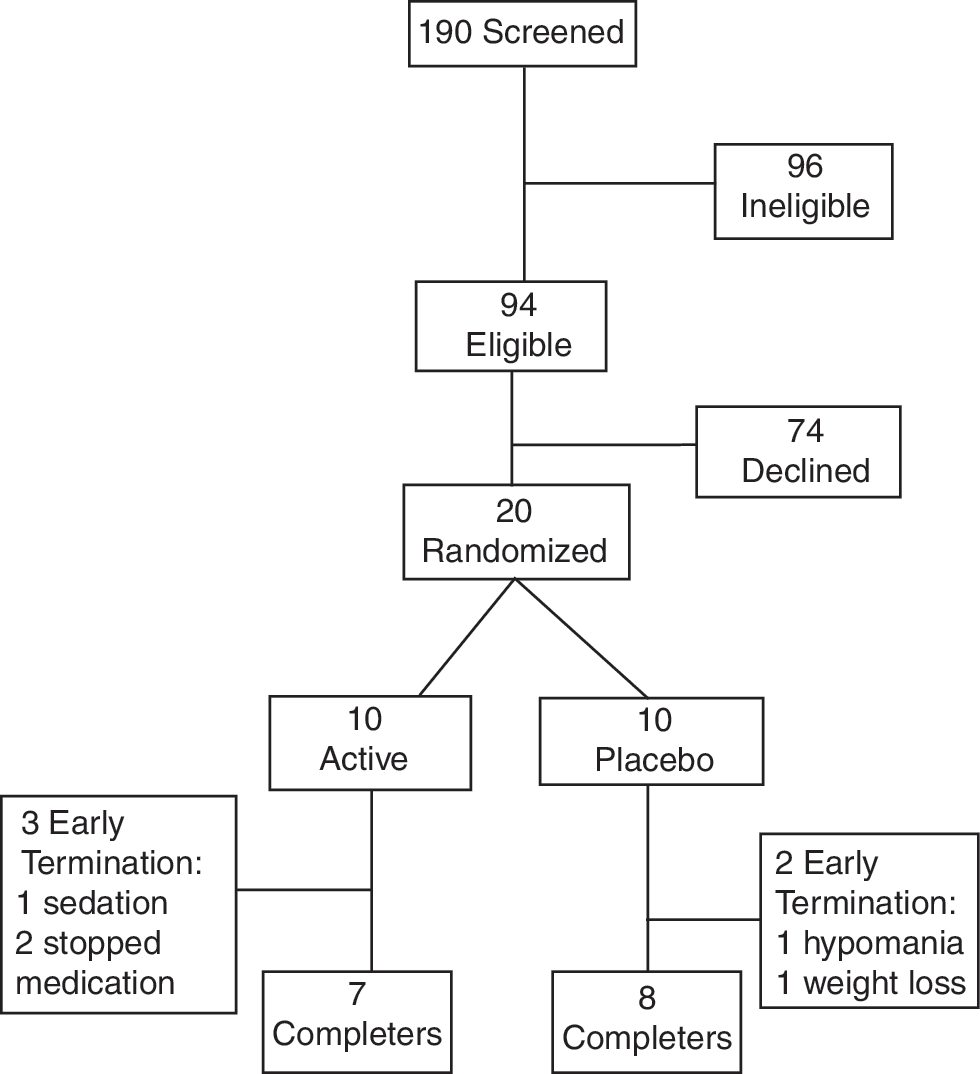
Study participant flow.
The 20 enrolled patients had a mean age of 17.1 years (range, 12.3–21.8 years) and a mean BMI of 16.4 (SD, 1.2; range, 13.4–18.2). Ethnicity reflected the eating disorder treatment population at our medical center and did not differ between the treatment arms. Sixteen (80%) of the participants were Caucasian, 2 (10%) were Asian, and 1 (5%) each was Hispanic or Black. Fourteen participants met full Diagnostic and Statistical Manual of Mental Disorders, 4th edition (American Psychiatric Association 1994), criteria for AN-R; the remaining six participants met all criteria except for 3 months of amenorrhea and were evenly distributed across the two treatment groups. At study entry, nine were inpatients, six were day-hospital patients, and five were attending the eating disorders outpatient clinic weekly.
There were no significant differences between the placebo and olanzapine groups at baseline in age in years (18.10 ± 2.04 vs. 16.41 ± 2.20, t = 1.78, p = 0.09, df = 18), weight in pounds (92.20 ± 8.11 vs. 94.77 ± 8.66, t = −0.66, p = 0.52, df = 18), or height in inches (63.87 ± 3.10 vs. 62.80 ± 2.61, t = 0.85, p = 0.40, df = 18). However, when taken together to calculate % MBW, these small differences between groups resulted in a significantly lower mean % MBW for the placebo group at baseline. To correct for this difference in % MBW, the initial repeated measures analysis of variances of all other variables contained the covariate of “% MBW” in all analyses. In each case, it did not significantly enter the model and was dropped from the final results presented in Table 1.
MBW = mean body weight.
Fifteen of our 20 enrolled patients (75%) completed this 10-week pilot study. The reasons for noncompletion differed between the groups. Three participants (15%) assigned to olanzapine treatment withdrew consent prior to the week 5 assessment, citing dissatisfaction with medication treatment, whereas the two noncompleters from the placebo arm were removed by the investigators for clinical worsening (Fig. 1). The mean daily dose of active olanzapine at week 10 was 8.5 mg. Five of seven (71.4%) participants assigned to the olanzapine arm had detectable serum olanzapine levels at weeks 5 and 10. No participants assigned to placebo treatment had detectable olanzapine levels. During their study participation, there were no significant differences between the placebo and olanzapine treatment groups in the mean number of days of inpatient treatment (5.9 ± 11.1 vs. 3.0 ± 5.0), day hospital (22.6 ± 15.4 vs. 20.9 ± 16.4), or outpatient treatment (33.6 ± 21.7 vs. 31.2 ± 22.5).
Mean % MBW improved in both treatment arms, as indicated by a significant main effect of time, with 10 weeks differing significantly from baseline (t = −2.68, p = 0.01). Contrary to our hypothesis, adding olanzapine vs. placebo to a comprehensive eating disorder treatment program did not further improve mean % MBW at any time point in the intention-to-treat analyses (Table 1). Similar results were obtained when dropouts and nonadherers to olanzapine treatment were excluded from the analyses.
On the clinician-administered TESS, there were no significant group-by-time interactions for any of the items, including increased appetite, drowsiness, increased motor activity, rigidity, tremor, dystonia, akathisia, or dyskinesia.
The group-by-time interactions approached statistical significance for fasting glucose (F(2,45) = 2.99, p = 0.06) and fasting insulin (F(2,39) = 2.61 p = 0.09). Given that we had specific hypotheses that fasting glucose and insulin levels would be elevated at week 10 compared with baseline for the olanzapine group but not for the placebo group and that the two treatment groups would differ at week 10, we conducted those pairwise contrasts. At week 10, the olanzapine group had significantly elevated glucose levels when compared with the placebo group (t = −2.02, p = 0.05). The change from baseline to week 10 approached significance for the olanzapine group (t = −1.90, p = 0.06) but was not significant for the placebo group (t = 1.51, p = 0.14). With respect to insulin levels, the olanzapine group had significantly elevated levels at week 10 compared with their baseline levels (t = −2.73, p = 0.009) and compared with the placebo group at week 10 (t = −2.44, p = 0.02). Baseline vs. week 10 was not different for the placebo group (t = 0.10, p = 0.92).
Measures of metabolic recovery (REE and RQ) and cardiac function (ECG) did not differ between treatment arms (Table 1).
On both measures of general psychopathology (HDRS and the Brief Psychiatric Rating Scale), the placebo group had elevated scores, indicating greater psychopathology, when compared with the olanzapine group at baseline; however, the group-by-time interactions were not significant. On measures of specific eating behaviors and attitudes (EDE and YBC-EDS), there was a significant improvement over time for both treatment groups on the YBC-EDS Preoccupations score and the EDE Restraint score only, but no significant group-by-time interactions. There were also no significant group, time, or group-by-time effects for the body image assessment.
Discussion
This is the first placebo-controlled study in adolescents of the adjunctive use of olanzapine for the treatment of AN-R. It is also the only placebo-controlled, longitudinal study in antipsychotic-naive AN-R patients to explore the effects of olanzapine on REE.
Contrary to our hypotheses, the addition of olanzapine vs. placebo did not result in further increases in % MBW when added to a comprehensive eating disorder treatment program for adolescents with AN-R and did not contribute to improvements in general psychopathology assessments or eating attitudes or behavior. Both treatment groups experienced some improvement over time on measures of specific eating attitudes and behaviors as indicated by the decline in EDE Restraint and YBC-EDS Preoccupation scores. However, participants did not improve on many eating disorder symptoms. The persistence of the rituals, shape, eating and weight concerns, and body image distortion coupled with low motivation to change these attitudes and behaviors may place these young women at high risk for relapse.
There were no immediate safety concerns associated with the use of olanzapine in this 10-week study. However, the increases in mean fasting glucose and insulin levels on olanzapine relative to placebo, especially given the similarities in the amount of weight gained by both groups, suggest a direct metabolic effect of olanzapine and the need for close monitoring during its long-term use. These findings add to a growing body of evidence associating olanzapine with increases in fasting glucose levels, including in adolescents (Tohen et al. 2007).
The results of this study do not support an olanzapine-induced decrease in REE as a contributing mechanism for weight gain. For both treatment groups, REE, percentage of predicted REE, and RQ improved throughout treatment. However, both groups were at a low body weight at the end of this 10-week study and, as expected, (Schebendach et al. 1997) remained hypometabolic.
To our knowledge, only two comparable placebo-controlled trials of olanzapine for the treatment of AN have been published to date, and both have involved adult populations. One found an effect for olanzapine on rate of weight gain (Bissada et al. 2008) and the other did not (Brambilla et al. 2007). Our results are mostly consistent with Brambilla and colleagues' outpatient study of 30 adults with AN who were randomly assigned to have olanzapine vs. placebo added to standardized cognitive-behavioral therapy. Similar to our results, they found no difference in weight trajectory between treatment groups as well as no benefit in symptoms specific to eating disorder pathology. Unlike our findings, they did find a benefit of olanzapine in improving symptoms of depression as measured by the HDRS. However, in their analyses of AN subgroups (AN-R and AN binge-purge type), they suggested that the positive effects for olanzapine were found primarily in the binge-purge group.
Our results contrast those of Bissada and colleagues (2008) involving treatment of 34 adults in a day-hospital setting. They reported that the olanzapine-treated group gained weight at a significantly greater rate relative to placebo and that a greater proportion of olanzapine-treated patients achieved their target BMI of 18.5. Their study design, 10-week duration of treatment and mean dose of olanzapine administered, was similar to ours, but they included both restricting (n = 16) and binge-purge (n = 18) types of AN. No examination of response by clinical subtype was reported. Given the findings of Brambilla et al. (2007), the results by Bissada et al. may also have been driven by the responses of the binge-purge subjects.
Strengths of this study include its double-blind, placebo-controlled design and the use of a comprehensive eating disorder treatment program for all participants that provided continuity of care across treatment settings up to age 21. Other strengths include laboratory measures such as fasting glucose and insulin levels, serum olanzapine levels, indirect calorimetry, and comprehensive assessment of specific eating disorder symptomatology, including a measure to assess body image distortion, along with general psychopathology measures.
The impact of including 18–21-year-olds treated in our center is not clear. Given the more positive results from the two adult patient samples, it is also possible that younger patients are less responsive to olanzapine than are adults.
Limitations of this pilot study include the small sample size, resulting in some baseline differences between groups despite randomization, and the potential self-selection of patients who were motivated to gain weight. Our ability to detect any added benefit of adjunctive olanzapine may also have been undermined by the efficacy of the psychosocial and nutritional treatments all participants received, including the opportunity to transition between inpatient, day-hospital, and outpatient settings, as needed. Although randomization was stratified by inpatient versus outpatient status at study entry and the groups did not differ in the intensity of treatment received, their transitioning between these three settings may have added to the variance in the rates of weight gain and further diminished the study's ability to detect olanzapine's effects. Future studies that include binge-purge type and limit participation to outpatients may be better able to detect olanzapine's benefits, if any.
The high study refusal rate among eligible patients was a noteworthy challenge and is consistent with other reports in the literature wherein more than half the eligible participants declined study enrollment (e.g., Bissada et al. 2008). Our 75% retention rate in a pharmacotherapy study for AN is comparable to other published studies (Halmi et al. 2005; Bissada et al. 2008).
Conclusions
The lack of support for olanzapine's efficacy relative to placebo in the context of our comprehensive treatment setting, coupled with concerns regarding increases in insulin and glucose, dissuaded us from pursuing a larger placebo-controlled study of adjunctive olanzapine for adolescents with AN-R at our setting.
Clinical Significance
Recruitment into pharmacological studies in this population continues to be a challenge (Halmi et al. 2005; Halmi 2008). The high rate of study refusal, withdrawal, and nonadherence to medication treatment across studies indicate that pharmacotherapy is not perceived as a desirable modality of treatment by many patients with AN. These factors limit the sample size and generalizability of the studies that are conducted. Assessing and addressing factors related to treatment nonadherence using cognitive and behavioral techniques may allow for greater acceptance of pharmacological treatments.
Footnotes
Disclosures
Eli Lilly had no access to the data and were not involved in data analysis or in the preparation of this manuscript. Dr. V. Kafantaris has received investigator-initiated research support in the form of donation of medication from GlaxoSmithKline, donation of medication and matching placebo from Astra Zeneca, Eli Lilly, Janssen, and Pfizer, and research funding from Pfizer for an unrelated, NIH-funded study. Dr. S. Hertz has been on the speakers' bureau for Eli Lilly, Pfizer, and Forest. Dr. N. Golden is a co-investigator on a study examining bone mineral density in adolescent girls, funded by TEVA Pharmaceuticals. There is nothing to disclose that might pose a conflict of interest for the present study. Dr. A.K. Malholtra is or has been a consultant to Eli Lilly, Merck, Janssen, BMS, and Vanda Pharmaceuticals. E. Leigh, Ph.D., Alison Berest, M.A., J. Schebendach, Ph.D., W.M. Sterling, M.S., E. Saito, M.D., C. Higdon, M.D., and S. Sunday, Ph.D., have no institutional or corporate/commercial relationships that might pose a conflict of interest.
Acknowledgments
The authors thank Victor Fornari, M.D., for his ongoing support and guidance and Tameka Fraser for her expert assistance in manuscript preparation. This study was supported by an investigator-initiated grant from Eli Lilly. Eli Lilly also supplied olanzapine and matching placebo tablets and analyzed the blinded, de-identified serum samples for olanzapine levels.
This study took place at the Division of Child and Adolescent Psychiatry at Schneider Children's Hospital of the North Shore-Long Island Jewish Health System, New Hyde Park, New York (now known as Cohen Children's Medical Center).